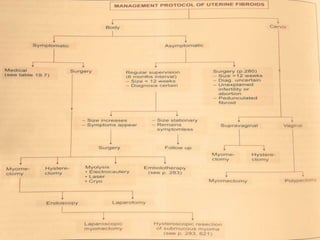
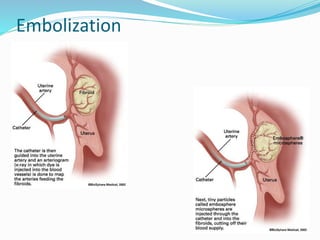
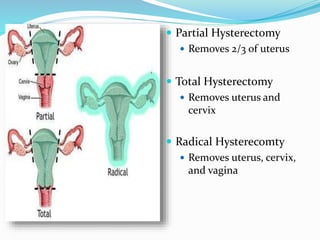
Medical management of fibroids involves hormonal treatments to control menorrhagia and improve hemoglobin levels before surgery. The objectives are to improve menorrhagia, correct anemia, minimize fibroid size to facilitate surgery, and serve as an alternative to surgery for some patients. Drugs used include iron supplements, NSAIDs, GnRH agonists/antagonists, danazol, and mifepristone. Surgical options include myomectomy to remove fibroids while preserving the uterus, hysterectomy to remove the uterus, and uterine artery embolization to reduce fibroid size and bleeding. The choice depends on desire for future fertility and uterine preservation.