Introduction to TechnologyTransfer (TT)
Core Definition: Technology transfer is defined as a "logical
procedure that controls the transfer of any process together
with its documentation and professional expertise between
developments or between manufacture sites".
Scope: It is a systematic procedure followed to pass the
documented knowledge and experience gained during
development and/or commercialization to an appropriate,
responsible, and authorized party.
Key Aspect: It is integral and critical to the drug discovery
and development process for new medical products.
3.
Goals and Objectives
Standardization: TT helps achieve a standardized process
which facilitates cost-effective production.
Quality Maintenance: It provides efficiency in the process
and maintains the quality of the product.
Commercialization: It is the process by which an original
innovator of technology makes it available to a commercial
partner to exploit the technology.
4.
Stages of TechnologyTransfer
Invention: Involves the initial idea and technology feasibility
Prototype/Scale-Up: Moving from lab scale to pilot scale .
Product Development: Refining the formulation and process.
Initial Manufacture: The first production batches.
Commercialization: Full market release.
5.
Ways Technology TransferOccurs
Government to Private: Transfer from government labs to
private sector firms.
Private to Private (Domestic): Between private sector firms
within the same country.
Private to Private (International): Between private sector
firms of different countries.
Academia to Private: From universities/research institutes
to private sector firms
6.
WHO Guidelines: Overview
Nature of Guidelines: These principles serve as a
framework to be applied flexibly rather than as rigid
guidance.
Focus: The primary focus is placed on quality aspects, in
line with WHO's mandate.
Applicability: Transfer occurs at various stages:
development, scale-up, manufacturing, production, launch,
and post-approval phase.
7.
Drivers for TechnologyTransfer
Capacity Expansion: The need for additional manufacturing
capacity.
Relocation: Moving operations to a different site or region.
Consolidation: Mergers and acquisitions often trigger intra-
and inter-company transfers.
Regulatory Recommendation: The WHO Expert Committee
recommended these guidelines to address these changing
business strategies.
8.
Requirements for Transfer
Planning: Requires a documented, planned approach using
trained and knowledgeable personnel.
Quality System: Must work within a quality system with
documentation covering all aspects of development,
production, and QC.
Entities Involved: Usually involves a Sending Unit (SU), a
Receiving Unit (RU), and a unit managing the process.
9.
General Principles (Part1)
Quality Risk Management (QRM): The project plan should
encompass quality aspects and be based on QRM principles.
Capabilities: The capabilities of the SU and RU should be
similar, though not necessarily identical.
Gap Analysis: A comprehensive technical gap analysis
(including technical risk assessment and regulatory gaps)
should be performed between SU and RU.
10.
General Principles (Part2)
•Training: Adequately trained staff must be available at the
RU, or they should be trained by the SU.
•Regulatory Interpretation: Regulatory requirements in the
countries of both the SU and RU must be taken into account
and interpreted consistently.
•Knowledge Transfer: There should be effective process and
product knowledge transfer.
11.
Criteria for Success
Documented Evidence: TT is successful only if there is
documented evidence that the RU can routinely reproduce
the transferred product, process, or method.
Predefined Specifications: The reproduction must meet a set
of specifications agreed upon with the SU.
Feedback: If the RU identifies problems, they must
communicate them back to the SU to ensure continuing
knowledge management.
12.
The Technology TransferProtocol
1. Protocol Purpose
The transfer protocol should list the intended sequential stages
of the transfer.
It serves as the roadmap for the entire transfer process,
ensuring no steps are missed.
Objective & Scope: Must clearly define what is being
transferred and the boundaries of the project .
2. Personnel & Responsibilities
• The protocol must identify key personnel involved in the
transfer.
• It must clearly define their specific responsibilities (e.g., who is
responsible for validation, who is responsible for training).
13.
3. Comparisons &Evidence
Parallel Comparison: Must include a comparison of materials,
methods, and equipment between the Sending Unit (SU) and
Receiving Unit (RU).
Documented Evidence: Each transfer stage must have evidence
that it has been satisfactorily accomplished before the next stage
commences .
4. Critical Control & Methods
CCPs: Identification of Critical Control Points in the
manufacturing process.
Analytical Methods: Must include the experimental design and
acceptance criteria for analytical methods to be transferred.
14.
5. Batches &Validation
Trial/Qualification Batches: Information on trial production
batches and qualification batches must be included.
Process Validation: Details on how process validation will be
conducted.
Change Control: A system for managing any process deviations
encountered during the transfer.
6. Product Assessment & Retention
End-Product: Procedure for the assessment of the final product.
Retention Samples: Arrangements for keeping retention samples
of active ingredients, intermediates, and finished products.
Reference Substances: Information on reference standards where
applicable.
15.
7. Approval
Conclusion:The protocol must conclude with a summary of the
transfer status.
Sign-off: Must include signed-off approval by the project
manager to officially close or approve steps.
8. Transfer Areas Addressed
Development and production (processing, packaging, cleaning).
Analytical methods for Quality Assurance and Quality Control.
Skills assessment and training.
Assessment of premises and equipment.
16.
9. Legal Implicationsin Protocol
Issues like intellectual property rights, royalties, pricing, and
conflict of interest must be addressed.
These should be resolved before and during planning to prevent
impact on technical communication.
Lack of transparency here leads to ineffective transfer.
10. Responsibilities of Units
SU Responsibilities: Provide comprehensive information (process,
API, safety).
RU Responsibilities: Review information, perform gap analysis,
and implement the process.
Some responsibilities may overlap with the "management unit".
17.
Quality Risk Management(QRM)
Definition of QRM:
Quality Risk Management is a systematic process for the assessment,
control, communication, and review of risks to the quality of the
drug (medicinal) product.
It applies across the entire product lifecycle.
Two Primary Principles
Scientific Basis: The evaluation of risk to quality should be based
on scientific knowledge and ultimately link to the protection of
the patient.
Effort vs. Risk: The level of effort, formality, and documentation
of the QRM process should be commensurate with the level of
risk.
18.
Responsibilities
Quality riskmanagement activities are usually, but not always,
undertaken by interdisciplinary teams.
Teams should include experts from the appropriate areas
• Quality Unit
• Business Development
• Engineering
• Regulatory Affairs
• Production Operations
• Sales And Marketing
• Legal
• Statistics And Clinical
• knowledgeable individuals about QRM process.
19.
The QRM ProcessSteps
Initiation: Define the problem and risk question.
Risk Assessment: Identification, Analysis, and Evaluation.
Risk Control: Reduction and Acceptance.
Risk Review: Monitoring events.
20.
Initiating a QualityRisk Management Process
Quality risk management requires systematic processes to improve
science-based decision-making.
The key steps to initiate and plan this process are:
Define the Risk: Identify the specific problem or risk question,
including assumptions about potential risks.
Gather Data: Assemble background information regarding
hazards, harm, or human health impacts.
Assign Resources: Identify a leader and the necessary resources.
Set Plan: Specify the timeline, deliverables, and the appropriate
level of decision-making.
22.
1. Risk Assessment
Risk assessment consists of the identification of hazards and the
analysis and evaluation of risks associated with exposure to those
hazards.
Quality risk assessments begin with a well-defined problem
description or risk question.
Three fundamental questions are often helpful:
1. What might go wrong?
2. What is the likelihood (probability) it will go wrong?
3. What are the consequences (severity)?
23.
A. Risk Identification
It is a systematic use of information to identify hazards referring to
the risk question or problem description.
Information can include historical data, theoretical analysis,
informed opinions, and the concerns of stakeholders.
Risk identification addresses the “What might go wrong?”
question, including identifying the possible consequences.
B. Risk analysis
Risk analysis is the estimation of the risk associated with the
identified hazards.
It is the qualitative or quantitative process of linking the likelihood
of occurrence and severity of harms.
24.
C. Risk Evaluation
It compares the identified and analyzed risk against given risk
criteria.
The output of a risk assessment is either a quantitative estimate of
risk or a qualitative description of a range of risk.
When risk is expressed quantitatively, a numerical probability is
used.
Alternatively, risk can be expressed using qualitative descriptors,
such as “high”, “medium”, or “low”, which should be defined in as
much detail as possible.
25.
2. Risk Control
Risk control includes decision making to reduce and/or accept
risks.
The purpose of risk control is to reduce the risk to an acceptable
level.
Risk control might focus on the following questions:
1. Is the risk above an acceptable level?
2. What can be done to reduce or eliminate risks?
3. What is the appropriate balance among benefits, risks and
resources?
4. Are new risks introduced as a result of the identified risks
being controlled?
26.
Risk Reduction &Communication
A. Risk Reduction
Focus on Mitigation: This step centers on processes to mitigate
or avoid quality risks when they exceed a specified or acceptable
level.
Actionable Measures: Risk reduction involves taking specific
actions to lower both the severity and the probability of harm.
Control Strategy: It also includes implementing processes that
improve the detectability of hazards and quality risks as part of
the overall risk control strategy.
27.
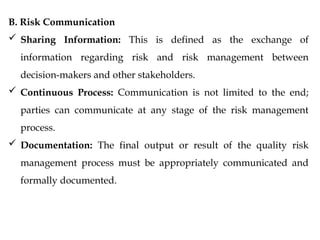
B. Risk Communication
Sharing Information: This is defined as the exchange of
information regarding risk and risk management between
decision-makers and other stakeholders.
Continuous Process: Communication is not limited to the end;
parties can communicate at any stage of the risk management
process.
Documentation: The final output or result of the quality risk
management process must be appropriately communicated and
formally documented.
28.
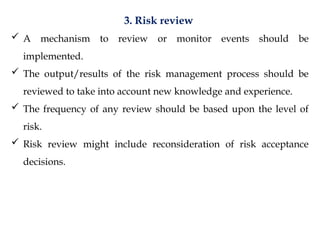
3. Risk review
A mechanism to review or monitor events should be
implemented.
The output/results of the risk management process should be
reviewed to take into account new knowledge and experience.
The frequency of any review should be based upon the level of
risk.
Risk review might include reconsideration of risk acceptance
decisions.
29.
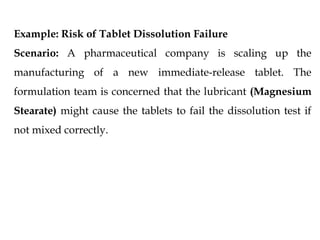
Example: Risk ofTablet Dissolution Failure
Scenario: A pharmaceutical company is scaling up the
manufacturing of a new immediate-release tablet. The
formulation team is concerned that the lubricant (Magnesium
Stearate) might cause the tablets to fail the dissolution test if
not mixed correctly.
30.
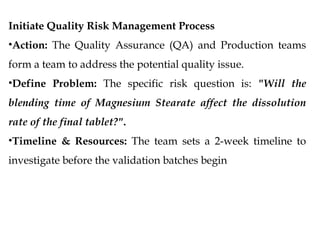
Initiate Quality RiskManagement Process
•Action: The Quality Assurance (QA) and Production teams
form a team to address the potential quality issue.
•Define Problem: The specific risk question is: "Will the
blending time of Magnesium Stearate affect the dissolution
rate of the final tablet?".
•Timeline & Resources: The team sets a 2-week timeline to
investigate before the validation batches begin
31.
2. Risk Assessment
•RiskIdentification:
• Hazard: hydrophobic nature of Magnesium Stearate.
• Risk: If the lubricant is blended for too long (over-lubrication), it
creates a water-repellent film around the drug particles, preventing
them from dissolving.
•Risk Analysis:
• Probability: High (if manual blending is not timed strictly).
• Severity: High (Dissolution is a Critical Quality Attribute; failure leads
to batch rejection).
• Detectability: Medium (Detected only at the final QC stage, which is
too late).
•Risk Evaluation:
• The team calculates the risk score (RPN). The result is found to be
Unacceptable without further controls.
32.
3. Risk Control
•RiskReduction:
• Mitigation: The team decides to automate the blending process
and strictly limit the lubrication time to 3 minutes.
• Strategy: They update the Batch Manufacturing Record (BMR)
to include a specific "Hold Time" and mixing speed parameter.
•Risk Acceptance:
• After implementing the 3-minute limit, the residual risk is re-
evaluated. The probability of failure is now Low. The risk is
deemed Acceptable.
33.
4. Risk Communication
•Action:The updated BMR and the risk report are shared with the
Production Manager and the Operators.
•Training: Operators are trained on why the 3-minute limit is critical,
ensuring they understand the risk to the patient (bioavailability).
5. Output / Result
•Document: The formal QRM report is filed, and the Critical Process
Parameter (CPP) for blending time is officially recorded in the Master
Formula Record.
34.
6. Risk Review
•Event:After the first three commercial batches are manufactured.
•Review: .
The team reviews the dissolution data from these batches. If all
pass with high margins, the risk management plan remains in
effect.
If one fails, the process loops back to Risk Assessment.
35.
QRM Tools &Methodology
Methodology Overview
QRM supports a scientific and practical approach to decision-
making.
It provides documented, transparent, and reproducible methods.
Regulators and industry use recognized tools and internal
procedures (SOPs).
Basic Facilitation Methods
1. Flowcharts: Visualizing the process to identify steps where risks
may occur.
2. Check Sheets: Simple lists to ensure all steps or checks are
completed.
3. Process Mapping: Detailed diagrams of the manufacturing
process.
These are used to organize data and facilitate decision-making.
36.
Failure Mode EffectsAnalysis (FMEA)
Focus: Evaluates potential failure modes for processes and their likely
effect on outcomes and/or product performance.
Usage: widely used to analyze reliability and identify where the
process might fail.
Output: Risk Priority Number (RPN) based on Severity, Occurrence,
and Detection.
Failure Mode, Effects and Criticality Analysis (FMECA)
Extension of FMEA: Similar to FMEA but adds a "criticality" analysis.
Focus: Charts the probability of failure modes against the severity of
their consequences.
Goal: To prioritize risks that are most critical to patient safety.
37.
Fault Tree Analysis(FTA)
Approach: A top-down approach.
Method: Starts with a hypothesized failure (top event) and works
backward to identify the root causes.
Visualization: Uses a tree structure to map out the logical
relationships between faults.
Hazard Analysis and Critical Control Points (HACCP)
Principles:
1.Conduct a hazard analysis.
2.Identify Critical Control Points (CCPs).
3.Establish critical limits for each CCP.
4.Establish monitoring procedures.
38.
Hazard Operability Analysis(HAZOP)
Focus: Brainstorming technique to identify hazards and operability
problems.
Method: Uses "guide words" (e.g., No, More, Less, Reverse) applied
to process parameters (Flow, Temp, Pressure) to identify deviations.
Application: Very common in chemical processing steps of API
manufacture.
Preliminary Hazard Analysis (PHA)
Timing: Performed early in development when there is little
information on design details.
Goal: To identify hazards and hazardous situations early to avoid
them in the design phase.
39.
Risk Ranking andFiltering
Method: A tool for comparing and ranking risks.
Process: Risks are evaluated against multiple criteria and weighted to
produce a score.
Outcome: Helps prioritize which risks require immediate attention
and resources.
Supporting Statistical Tools
Usage: Statistical tools are used to support data analysis within QRM.
Examples: Control charts, Design of Experiments (DoE), Histograms,
Pareto charts.
These tools provide the data needed to assess probability and severity
accurately.
40.
Transfer from R&Dto Production
1. Strategic Planning
Before any physical transfer begins, specific strategic decisions
must be made:
Production Type: It must be established whether the
intention is to perform single-batch manufacture, continuous
production, or "campaigns" (producing one product for a set
period).
Capacity Check: We must verify if the Receiving Unit (RU)
can accommodate the intended production capacity.
41.
Depth of Transfer:
Consideration must be given to the level of detail transferred.
Does the RU need to support further process optimization or
development?
If so, deeper developmental history is required.
2. The Process Protocol
The Sending Unit (SU) and RU should jointly develop a
protocol for the transfer of relevant information.
This ensures the RU can develop an "equivalent process" to
the one at the SU.
42.
3. Detailed CharacterizationPackage (SU Deliverables)
The SU must provide a detailed characterization of the
product, including:
Qualitative and quantitative composition.
Physical description.
Method of manufacture.
In-process controls and specifications.
Packaging components and configurations.
Special safety and handling considerations.
43.
4. History ofProcess Development
The SU must provide the "backstory" of the drug to enable the RU
to solve future problems. This includes:
Clinical Development Info: Rationale for the synthesis route,
form selection, technology selection, equipment, and clinical
tests.
Scale-Up Info: Reports on process optimization, statistical
optimization of critical parameters, and pilot-scale reports
indicating the number/disposition of batches.
Full-Scale Info: Reports on full-scale activities, deviation
reports, and change control reports that led to the current
manufacturing process.
44.
5. Health, Safety,and Environment (HSE)
The SU must provide info on health/safety issues, specifically
including the need for gowning or protective clothing.
6. Current Processing Information
The SU must provide specific details on the current process,
including
Detailed description of facility requirements and equipment.
Information on starting materials and Material Safety Data
Sheets (MSDS).
Process Description: Narrative descriptions and process
maps/flow charts.
45.
Hold Times:Qualification of in-process hold times and
conditions.
Material Addition: The specific order and method of raw
material addition.
Analytical Methods: Description of methods used for
testing.
In-Process Controls (IPC): Identification of critical
performance aspects, control points, and Statistical Process
Control (SPC) charts.
Validation & Stability: Validation plans/reports, annual
product reviews, and stability info.
46.
Packaging & CleaningTransfer
1. Packaging Transfer
Information Required: SU must provide specifications for a
suitable container/closure system, design, packing, processing,
and labelling requirements.
QC Testing: Specifications must be provided for drawings,
artwork, and material (glass, card, fibre board).
Suitability Study: The RU must perform a study to check four
key criteria:
i. Protection: Preventing degradation from environment
(moisture/light).
47.
i. Safety: Absenceof undesirable substances (leachable) released
into the product.
ii. Compatibility: Absence of interaction affecting drug quality.
iii. Performance: Functionality in terms of drug delivery.
2. Cleaning Transfer
Objective: To minimize cross-contamination from previous
manufacturing steps, operator exposure, and environmental
impact.
SU Deliverables: Cleaning procedures currently in use.
Solubility information of active ingredients, excipients, and
vehicles.
Therapeutic doses and toxicological categories (to determine
cleaning limits)
48.
Granularity of Transfer(Starting Materials)
1. Active Pharmaceutical Ingredients (API)
The SU must provide the Drug Master File (DMF) and specific details
to be checked against specifications.
The required details are:
Manufacturer: Details of the vendor.
Synthesis: Flow chart of synthetic pathway, critical steps, process
controls, and intermediates.
Definitive Form: Photomicrographs, polymorphic forms, and
solvate forms.
Solubility: Solubility profile and Partition coefficient (with
method).
49.
Dissolution: Intrinsicdissolution rate (with method).
Particle Properties: Particle size distribution (with method).
Bulk Properties: Bulk/tap density, surface area, and porosity.
Moisture: Water content, hygroscopicity, and water activity data.
Microbiology: Sterility, bacterial endotoxins, and bioburden
(if API supports growth).
Stability: Summary of studies, conclusions, and retest date
recommendations.
Impurities: Listing of potential/observed synthetic impurities and
degradants.
Potency Factor: Observed purity and justification for input
quantity adjustments.
Special Considerations: Sensitivity to heat/light/moisture.
50.
2. Excipients
Functionality:Description of functionality (why is it used?)
and justification for antioxidants/preservatives.
Specifications:
Compendial: Monographs and info affecting processing.
Non-Compendial: Complete listing of specs, analytical
methods, and justification for release limits.
New Excipients: If used for the first time in humans, provide
the same level of detail as for an API.
Safety
51.
Finished Products Characterization
TheSU must transfer physical property info relevant to the
specific dosage form:
Solid & Inhaled Dosage Forms:
o Definitive form.
o Solubility profile.
o Particle size distribution.
o Bulk/Tap density, surface area, porosity.
o Compaction properties (Solid only).
o Water content and hygroscopicity.
52.
Semi-Solid /Topical:
o Melting point range.
o pH range.
o Viscosity.
o Specific gravity.
Parenteral (Injectable):
o pH range and Ionic strength.
o Specific gravity/density.
o Osmolarity.
o Microbiological considerations.
Transdermal (Patches):
o Solubility and Partition
coefficient.
o Intrinsic dissolution rate.
53.
Premises and Equipment
1.Premises (Facility)
SU Information: Must provide layout, construction, and finish of
buildings, plus HVAC details (temp, humidity, pressure)45
.
Risk Information: Must provide info on inherent risks
(fire/explosion, reactive chemicals) and exposure limits46
.
Comparison Considerations:
RU buildings must handle the agreed quality standard and volume.
QC labs must be capable of testing all APIs/products/cleaning
samples47
.
Dedicated Facilities: Buildings for highly sensitizing nature (e.g.,
penicillins and cytotoxics) must be dedicated and located in a
different facility48
.
54.
2. Equipment
Documentation:SU provides a list of makes/models,
drawings, manuals, maintenance logs, and calibration logs.
Gap Analysis: RU performs a side-by-side comparison. If
equipment differs, a gap analysis identifies if adaptation or
new equipment is needed 50
.
Comparison Factors: Minimum/maximum capacity,
material of construction, critical operating parameters, and
critical components (filters, screens, sensors) 51
.
New Equipment: Any newly acquired equipment must
undergo qualification up to OQ level (Operational
Qualification)52
.
55.
Qualification and Validation
1.Validation Master Plan (VMP)
Validation must be documented in a VMP.
Intra-company: RU operates under the same VMP as SU.
Inter-company: RU must have its own VMP in place before transfer
2. Execution Steps
Protocol: RU prepares a Validation Protocol (VP) for each step.
Report: Successful execution is documented in a Validation Report
(VR).
Commissioning: Setting up systems must be completed before
qualification/validation begins.
56.
3. Implementation Logic
i.SU provides info
ii. RU audits its systems
iii. RU prepares site-specific SOPs/training
iv. Staff is trained
v. Qualification/Validation is executed.
4. Qualification Stages
FAT: Factory Acceptance Tests (if possible).
IQ: Installation Qualification.
OQ: Operational Qualification.
PQ: Performance Qualification (established on commencement of
trial batches)
57.
Analytical Method Transfer(AMT)
1. General Requirement
Transfer of analytical methods needs to be in place before
process validation studies of manufacturing operations can
be carried out.
2. The Protocol
The SU should prepare a protocol defining the objective, scope,
responsibilities, materials, experimental design, and acceptance
criteria.
58.
3. SU Responsibilities
Provide method-specific training.
Provide validation reports and demonstrate robustness.
Provide standard reference samples (APIs, intermediates).
4. RU Responsibilities
Ensure necessary equipment
(spectrometers/chromatographs) is available and qualified62
.
Ensure personnel are trained.
59.
5. Training Protocol(The "Exam")
A suggested training protocol includes:
SU and RU analysts assay two retained samples from SU.
SU and RU analysts assay two sub-potent (spiked) samples.
SU and RU analysts assay samples taken from RU production.
RU analyst performs replicate analyses to enable a significance
test (e.g., Student's t-test) against the SU method.
60.
Approved Regulatory Bodies
1.CDSCO (India)
Central Drug Standards and Control Organization.
Under the Ministry of Health and Family Welfare.
Functions: Prescribes standards, regulates market
authorization of new drugs, oversees clinical trials, and
supervises drug imports.
DCGI: Drugs Controller General of India (Licensing and
Quality Control).
61.
2. USFDA (USA)
Food and Drug Administration.
Under Dept of Health and Human Services.
Responsible for food safety, tobacco, supplements, drugs
(prescription/OTC), vaccines, and medical devices.
3. TGA (Australia)
Therapeutic Goods Administration.
Manages the Australian Register of Therapeutic Goods (ARTG).
Products must be in ARTG to be supplied in Australia.
4. MHRA (UK)
Medicines and Healthcare products Regulatory Agency.
Regulates medicines and devices in the UK.
62.
Technology Transfer Agenciesin India
1. APCTT (Asian and Pacific Centre for Transfer of
Technology)
UN Regional Institution (ESCAP), est. 1977.
Focus: Promotes TT to/from Small and Medium-scale
Enterprises (SMEs) in Asia-Pacific.
Goal: Facilitate import/export of environmentally sound
technologies.
63.
2. NRDC (NationalResearch Development Corporation)
Est. 1953, under Dept of Scientific & Industrial Research.
Goal: Commercialize technologies/patents from national
R&D institutions/Universities.
Repository of technologies in Drugs, Pharma, Biotech, etc.
64.
3. TIFAC (TechnologyInformation, Forecasting and
Assessment Council)
Est. 1988, under Dept of Science & Technology.
Key Work: "Technology Vision 2020" (Dr. APJ Abdul Kalam)
and "Technology Vision 2035".
Delivers technology foresight reports.
4. BCIL (Biotech Consortium India Limited)
Est. 1990. Promoted by Dept of Biotechnology.
Goal: Transfer of technology for commercialization of
biotechnology products
65.
5. TBSE (TechnologyBureau for Small Enterprises)
Joint initiative of SIDBI and APCTT (1995).
Goal: Platform for MSMEs to tap global technology
opportunities (China, Philippines, Germany, USA).
66.
Legal Issues &Documentation
1. Confidentiality Agreements (NDA)
Aim: Protect all information of parties before negotiations start.
Requirement: Reference to property rights and description of
the technology must be included.
2. Licensing
Definition: The legal core of TT. The Licenser (owner) gives
rights to the Licensee (user).
Rights: Licensee gets "use" rights but not ownership.
Limitations: Can be limited by Time, Geography, or Product
Market.
67.
3. Memorandum ofUnderstanding (MoU)
Typically used for collaborative research with outside
institutions before final agreements.
Defines Intellectual Property (IP) sharing, roles, and
responsibilities.
Identifies who manages the IP and how licensing income is
shared



























![Transfer technologypharmaceuticalmanufacturingtrs961annex7[1]](https://cdn.slidesharecdn.com/ss_thumbnails/transfertechnologypharmaceuticalmanufacturingtrs961annex71-131217221719-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)











![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)








