Ultrasound in
Ultrasonography
Inphysics, the term "ultrasound" applies to
all acoustic energy (longitudinal,
mechanical wave) with a frequency
above the audible range of human
hearing. The audible range of sound is 20
hertz-20 kilohertz. Ultrasound is frequency
greater than 20 kilohertz.
3.
Ultrasound Technology
Principleof SONAR, used by bats and ships
Generation of high-frequency sound waves
through a transducer
Pulsed sound waves penetrate till structures
of different tissues densities is reached
Reflected energy to the transducer is
amplified and displayed on a screen
Detection of breathing, cardiac actions and
vessel pulsations
4.
Obstetrical Ultrasound
Introducedin the late 1950’s
ultrasonography is a safe, non-
invasive, accurate and cost-
effective means to investigate the
fetus
Computer generated system that
uses sound waves integrated
through real time scanners placed
in contact with a gel medium to
the maternal abdomen
The information from different
reflections are reconstructed to
provide a continuous picture of
the moving fetus on the monitor
screen
5.
Risks and Side-effects
Ultrasonography is generally considered a
"safe" imaging modality. However slight
detrimental effects have been occasionally
observed (see below). Diagnostic ultrasound
studies of the fetus are generally considered
to be safe during pregnancy. This diagnostic
procedure should be performed only when
there is a valid medical indication, and the
lowest possible ultrasonic exposure setting
should be used to gain the necessary
diagnostic information under the "as low as
reasonably achievable" or ALARA principle.
6.
World HealthOrganizations technical report
series 875(1998).supports that ultrasound is
harmless: "Diagnostic ultrasound is
recognized as a safe, effective, and highly
flexible imaging modality capable of
providing clinically relevant information
about most parts of the body in a rapid and
cost-effective fashion". Although there is no
evidence ultrasound could be harmful for
the fetus, US Food and Drug Administration
views promotion, selling, or leasing of
ultrasound equipment for making
"keepsake fetal videos" to be an
unapproved use of a medical device.
7.
Studies onthe safety of ultrasound
A study at the Yale School of Medicine
found a correlation between prolonged
and frequent use of ultrasound and
abnormal neuronal migration in mice. A
meta-analysis of several ultrasonography
studies found no statistically significant
harmful effects from ultrasonography but
mentioned that there was a lack of data
on long-term substantive outcomes such
as neurodevelopment.
8.
Types of Ultrasonography
TransAbdominal
Ultrasonography
(TAS)
Trans Vaginal
Ultrasonography
(TVS)
Doppler Ultrasound Tissue Harmonic
Imaging (THI)
Three-dimensional
Ultrasound (3-D
USG
9.
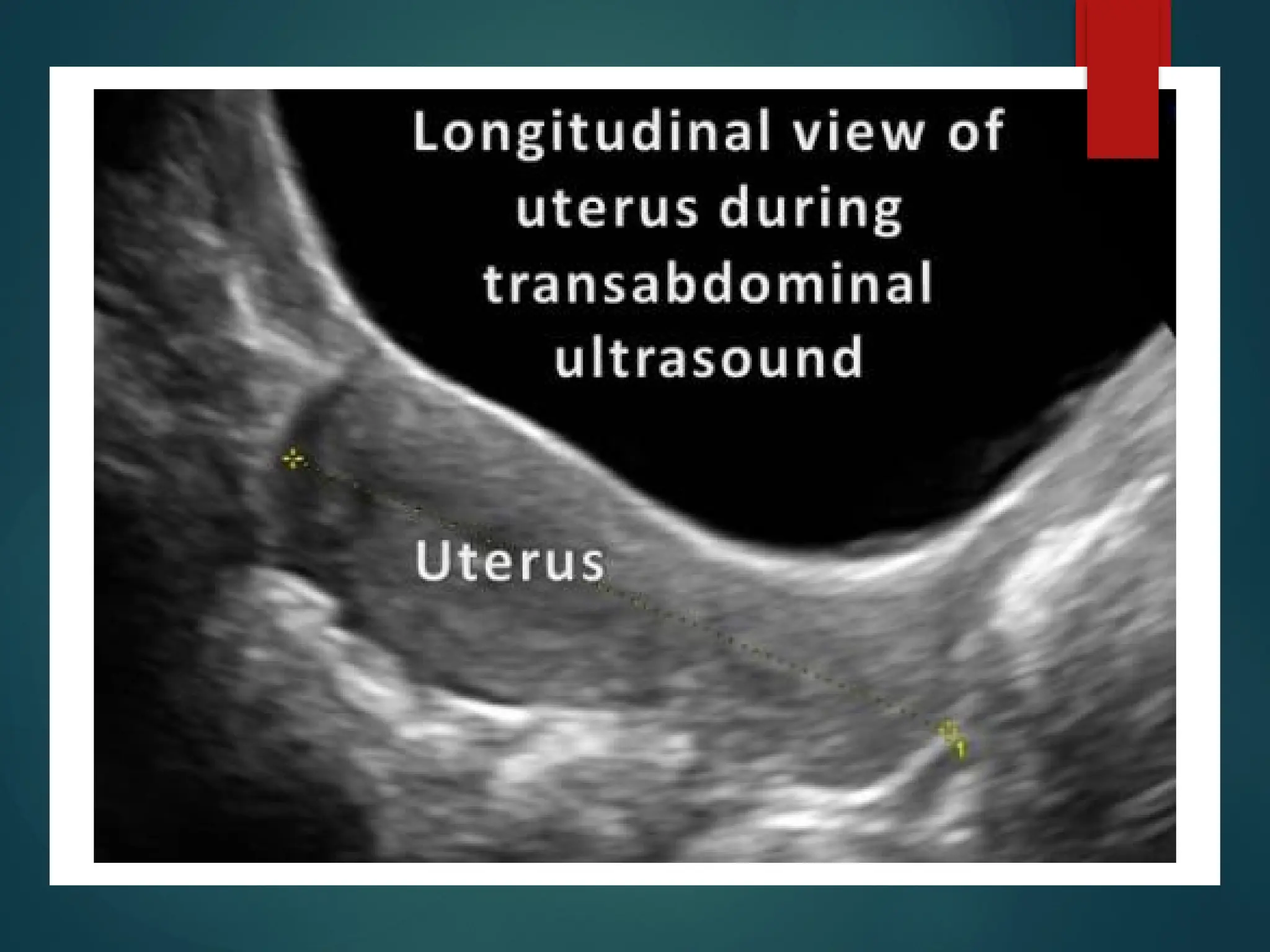
Trans Abdominal Ultrasound
(TAS)
•Major technique for imaging in 2nd
and 3rd
trimester
• Patient to have full bladder because
– Pushes the uterus out of the pelvis
– Provides an acoustic window
– Displaces pelvic bowel loop superiorly
• Real-time ultrasound equipment includes:
– Sector transducers, when access is limited
– Linear curved array transducers, for less distortion and
greater field of view
11.
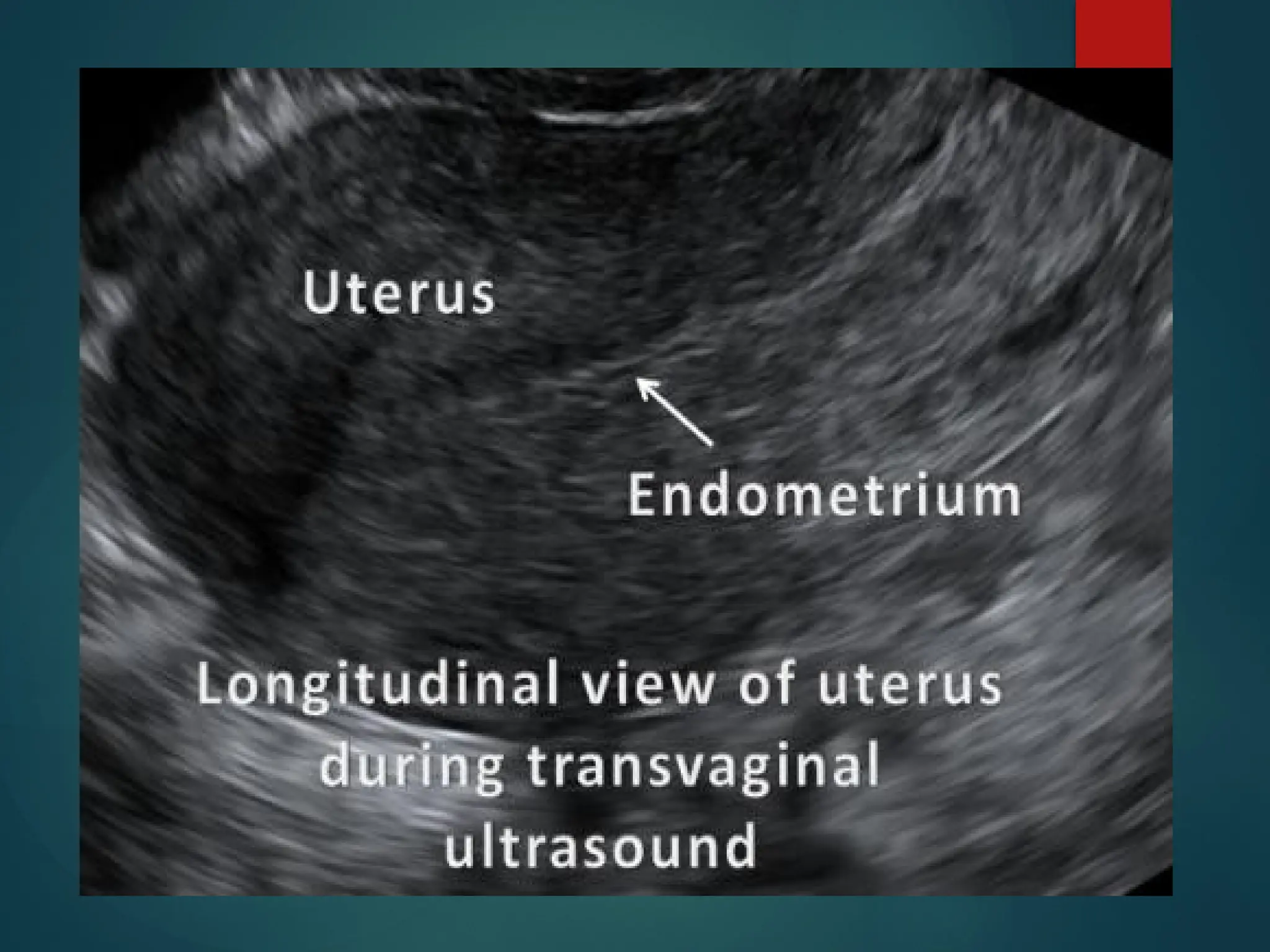
Trans Vaginal Ultrasound
(TVS)
Method of choice for
Monitoring infertility disorders
Diagnosis of ectopic pregnancy
Differentiation of normal and abnormal 1st
trimester pregnancy
Diagnosis of congenital anomalies in 2nd
trimester
Patient to have empty bladder because
Uterus will be pushed posteriorly out of the field
of view of the transducer
12.
Trans Vaginal Ultrasound(TVS)
cont
• Specially designed high frequency transducers
• Higher resolution images
• Favorable for obese patients or in early stage of
pregnancy
• Limitations include
– Reduced beam penetration
– More invasive nature of the technique
14.
Doppler Ultrasonography
• Mostwidely employed for detection of:
– Fetal cardiac pulsation
– Pulsation in various fetal blood vessels
• Doppler waveform for useful information about
intra-uterine growth retardation
• Use remains controversial due to increased power
16.
Tissue Harmonic Imaging
(THI)
Processing of lower amplitude, higher frequency
waveforms accompanying fundamental frequency
Lesser clutter and scatter
Better visualization of fetal structure
17.
Three-dimensional USG (3-
D)
3-Dimensional “cleaner” image of the scanning
Transducer captures series of images
3-D processing done by Computer
Significant improvement in identifying
Cleft lips
Spina bifida
Polydactyl
A) The followingqualified persons may
perform USG as far the provisions of the
Schedule i/ii/iii of IMC Act 1956 and
PCPNDT Act 1994
I. Radiologist with MD, DNB and DMRD
qualifications
II. Obstetric & Gynaecology
Specialist(MS/DNB/DGO) with 4 week of training
and 6months of experiences
III. Medical Officer(MBBS) with 6 months of training
in obstetric USG as mandate by PCPNDT Act 1994
21.
PC-PNDT
Act 1994
Pre-Conceptionand Pre-Natal Diagnostic Techniques
(Prohibition of Sex Selection) Act, 1994 an Act of the
Parliament of India enacted to stop female foeticides and
arrest the declining sex ratio in India. The act banned
prenatal sex determination.
Main provisions in the act are:-
1. The Act provides for the prohibition of sex selection, before or
after conception.
2. It regulates the use of pre-natal diagnostic techniques, like
ultrasound machine by allowing them their use only to
detect :- genetic abnormalities, metabolic disorders,
chromosomal abnormalities, certain congenital
malformations, haemoglobinopathies, Sex linked disorders.
3. No laboratory or centre or clinic will conduct any test including
ultrasonography for the purpose of determining the sex of
the foetus.
4. No person, including the one who is conducting the procedure
as per the law, will communicate the sex of the foetus to the
pregnant woman or her relatives by words, signs or any
other method.
5. Any person who puts an advertisement for pre-natal and pre-
conception sex determination facilities in the form of a notice,
circular, label, wrapper or any document, or advertises through
interior or other media in electronic or print form or engages in
any visible representation made by means of hoarding, wall
painting, signal, light, sound, can be imprisoned for up to three
years and fined Rs. 10,000.
Indications for
Ultrasonography
in ThirdTrimester
Fetal growth monitoring
Estimation of fetal weight
Evaluation of fetal wellbeing
Biophysical Profile
Placenta position
Amniotic fluid index
Presentation and lie
Follow up of anomalities in second
trimester
Post dated(placental aging, fluid
and fetal status)
26.
Post Partum
Indication of
Ultrasonography
PPH& Retained products of conception
Uterine rupture or dehiscene
Endometritis
Pelvic abscess
Bladder Injury
Ovarian vein thrombosis
Lochia abnormalities
CS scar evaluation
First Trimester USG
•0-4.3 weeks: no ultrasound findings
• 4.3-5.0 weeks:
• possible small gestational sac
• possible double decidual sac sign (DDSS)
• possible intradecidual sac sign (IDSS)
• 5.1-5.5 weeks:
•
gestational sac should be visible by this time
• 5.5-6.0 weeks
• yolk sac should be visible by this time
• gestational sac should be ~6 mm in diameter
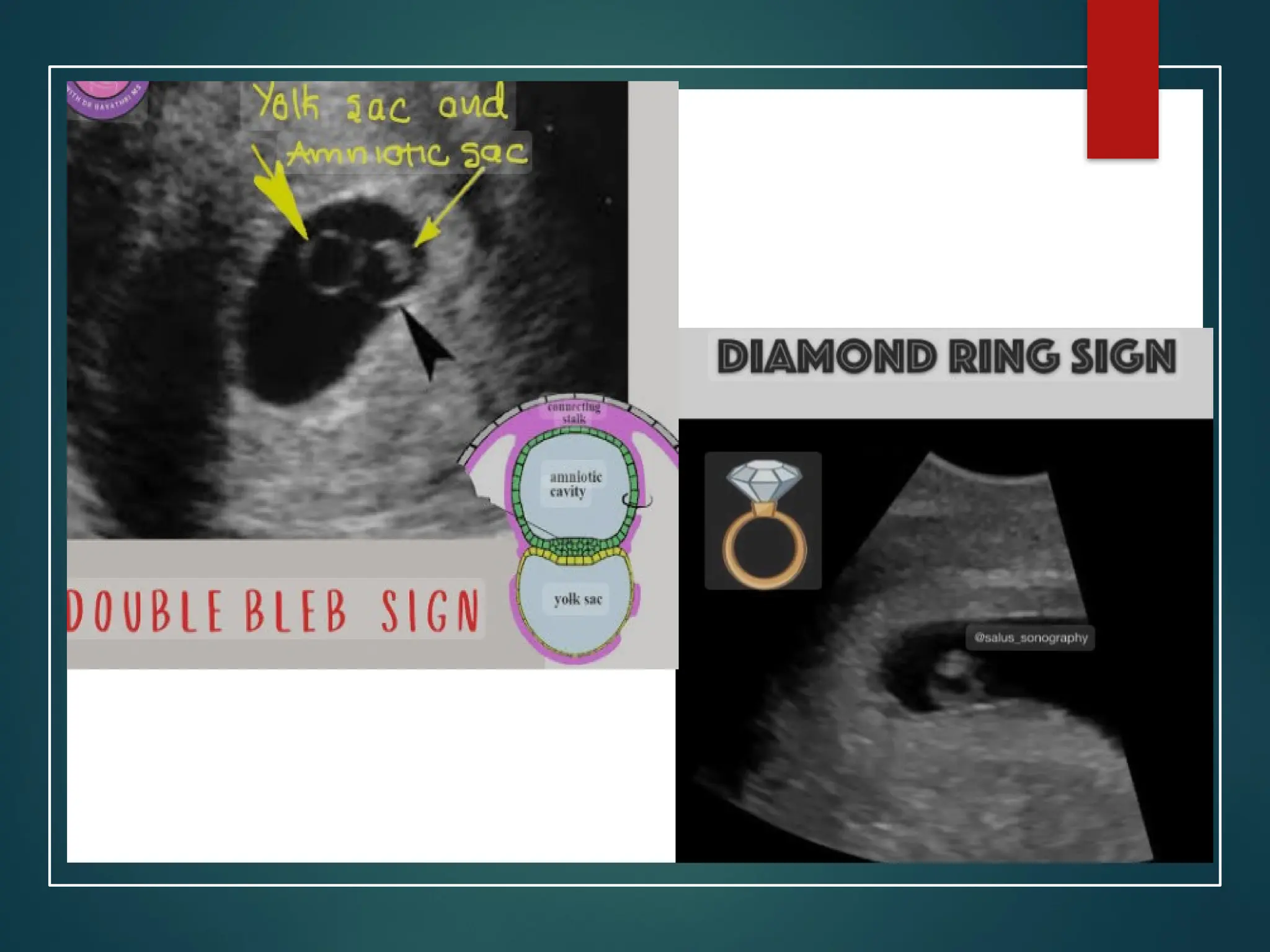
• Double bleb sign
• Diamond ring sign(6weeks)
29.
• >6.0 weeks
•fetal pole may be identifiable on endovaginal
ultrasound (1-2 mm)
• fetal heart rate (FHR) should be ~100-115 bpm
• gestational sac should be ~10 mm in diameter
• 6.5 weeks
• crown rump length (CRL) should be ~5 mm
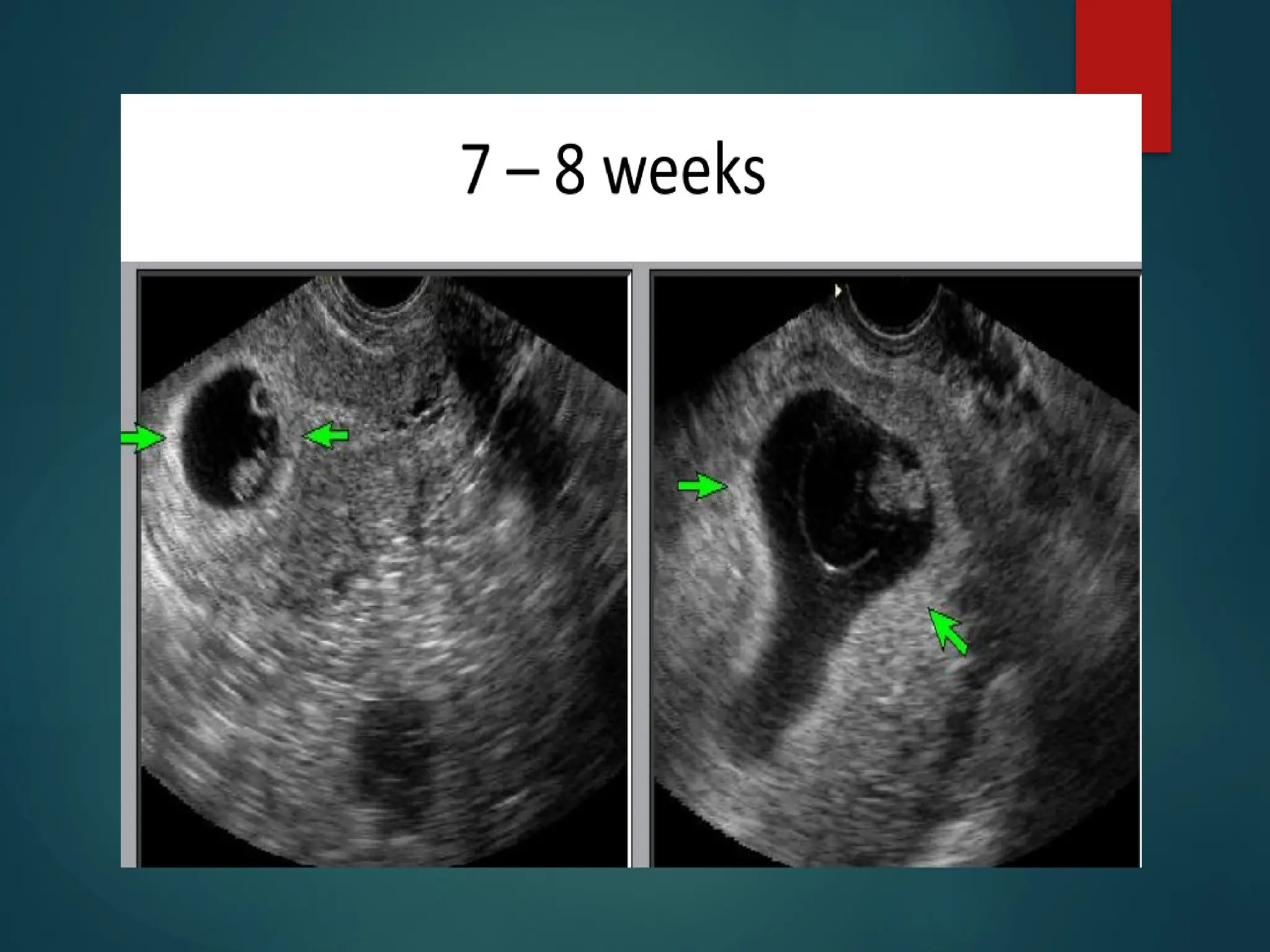
• 7-8 weeks
• CRL is between 11-16 mm
• cephalad and caudal poles can be identified
30.
• 8-9 weeks
•CRL is between 17-23 mm
• limb buds appear
• head can be seen as separate from the body
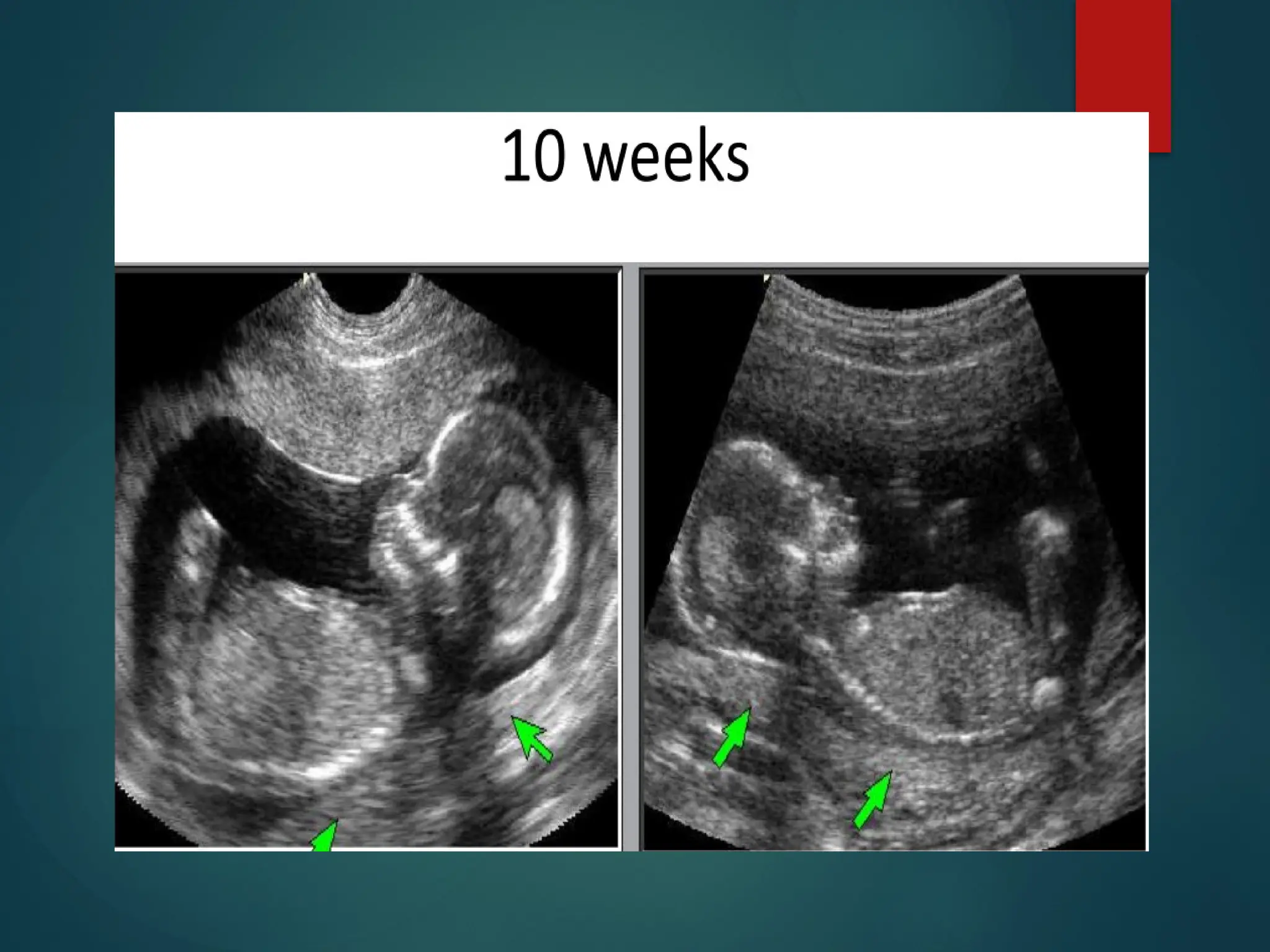
• 9-10 weeks
• CRL is between 23-32 mm
• fetal heart rate 170-180 bpm
• fetal movement can be seen
• a round hypoechoic structure in the fetal brain
represents a developing
embryonic/fetal rhombencephalon
11 weeks:
nuchal translucency may begin to be seen
31.
Gestational Sac
USG
• Roundor oval with
regular margin
• Eccentric toward one
side of endometrium
• May show yolksac or
embryo inside
• Wall is thick with
echogenic rim
• Intrauterine pregnancy
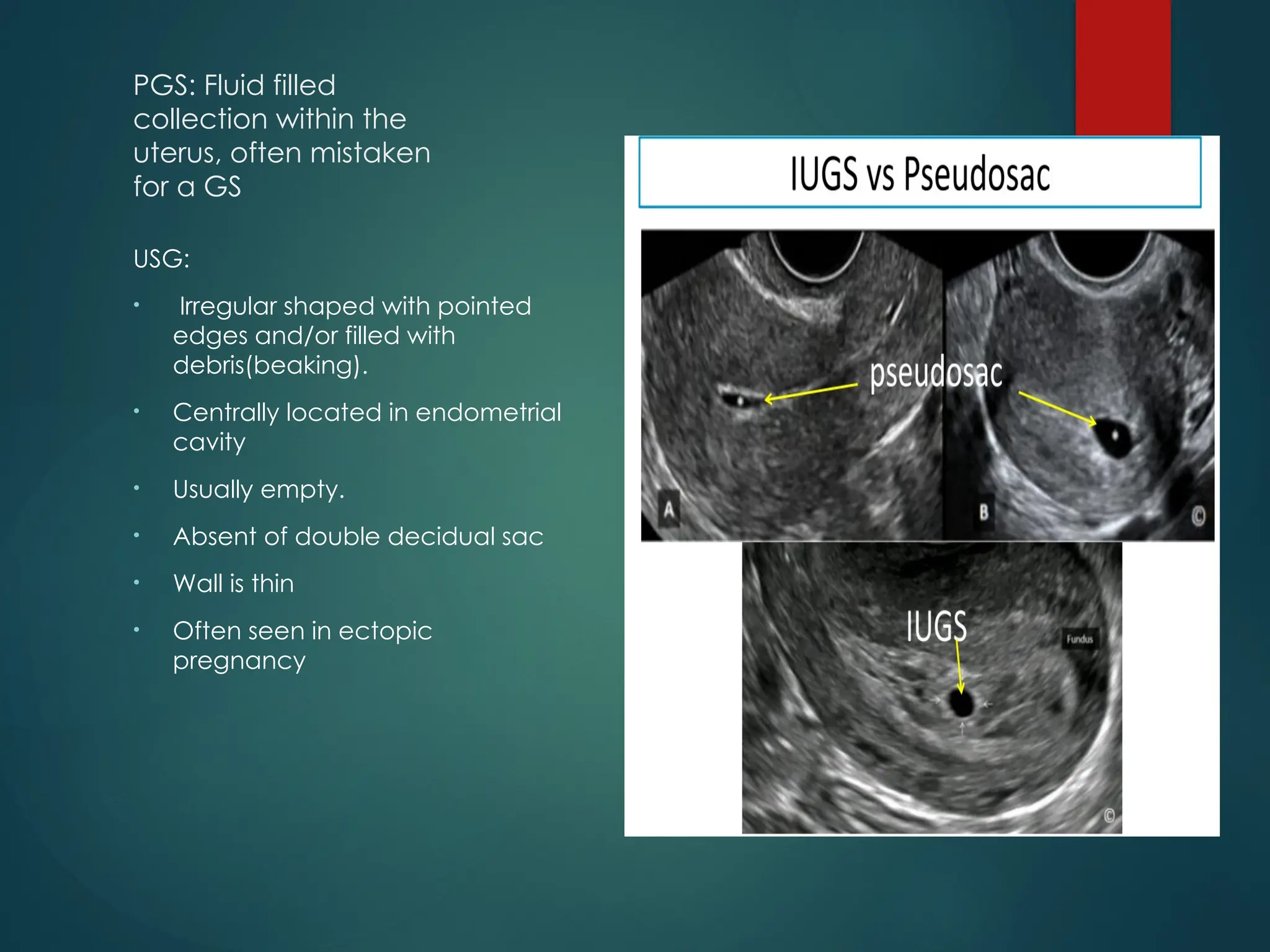
PGS: Fluid filled
collectionwithin the
uterus, often mistaken
for a GS
USG:
• Irregular shaped with pointed
edges and/or filled with
debris(beaking).
• Centrally located in endometrial
cavity
• Usually empty.
• Absent of double decidual sac
• Wall is thin
• Often seen in ectopic
pregnancy
35.
Fetal Heart Rateon USG
Visible heart activity: 43 days (6.1w)
Normal heart rate at 6 weeks: 90-110 bpm
At 8-9 weeks if nl heartbeat: 140-170bpm
At 9 weeks:140-195 bpm(average=170)
At 5-8 weeks a FHR <90 bpm is associated with a
high risk of miscarriage
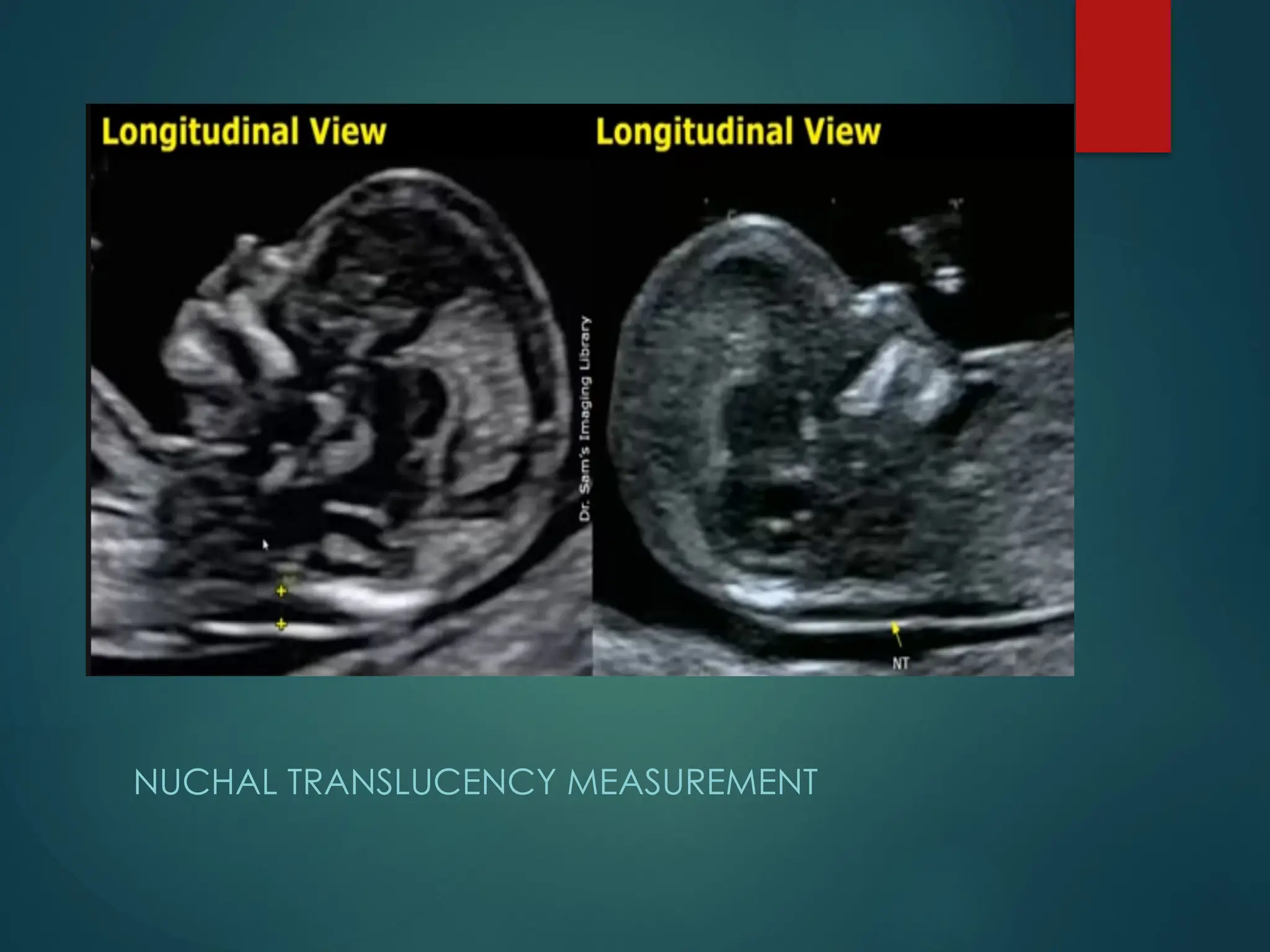
NUCHAL TRANSLUCENCY
Fluidfilled space in the back of the foetal neck.
Its measurement is used in the screening of the
chromosomal abnormalities in the first trimester
Ideal time for measuring NT is between 11 weeks
to 13weeks 6days of gestation (CRL between 45
to 84mm)
Can be scan using TAS & TVS
Fluid filled anechoic space at the back of the
foetal neck
Normal NT measurement <2mm
Ectopic Pregnancy:
Implantationof fertilised
ovum outside of the
uterine cavity
Risk of 1-2% of all the
pregnancy. The risk as
high as 18% first trimester
pregnancies with
bleeding
Locations:
Tubal ectopic: 93-97%
(ampulla 65%, Isthmus
11%, fimbria 10%,
interstitial 3%)
Ovarian ectopic: 0.5-1%
Cervical ectopic: <1%
Abdominal ectopic:
1.4%
Scar(CS):Rare
54.
USG of EctopicPregnancy
Empty uterine cavity or no evidence of
intrauterine pregnancy(exception: heterotopic
pregnancy)
Pseudogestational sac/decidual sac may be
seen in 10-20% of EP
Thick echogenic endometrium
Tube and ovary: simple adnexal cyst, complex
extraadnexal cyst/mass, solid hyperechoic
mass(not specific), tubal ring sign, ring of fire sign
Peritoneal cavity: Free pelvic
fluid/hemoperitoneum in pouch of Douglas, free
fluid in hepatorenal recess/Morison’s pouch
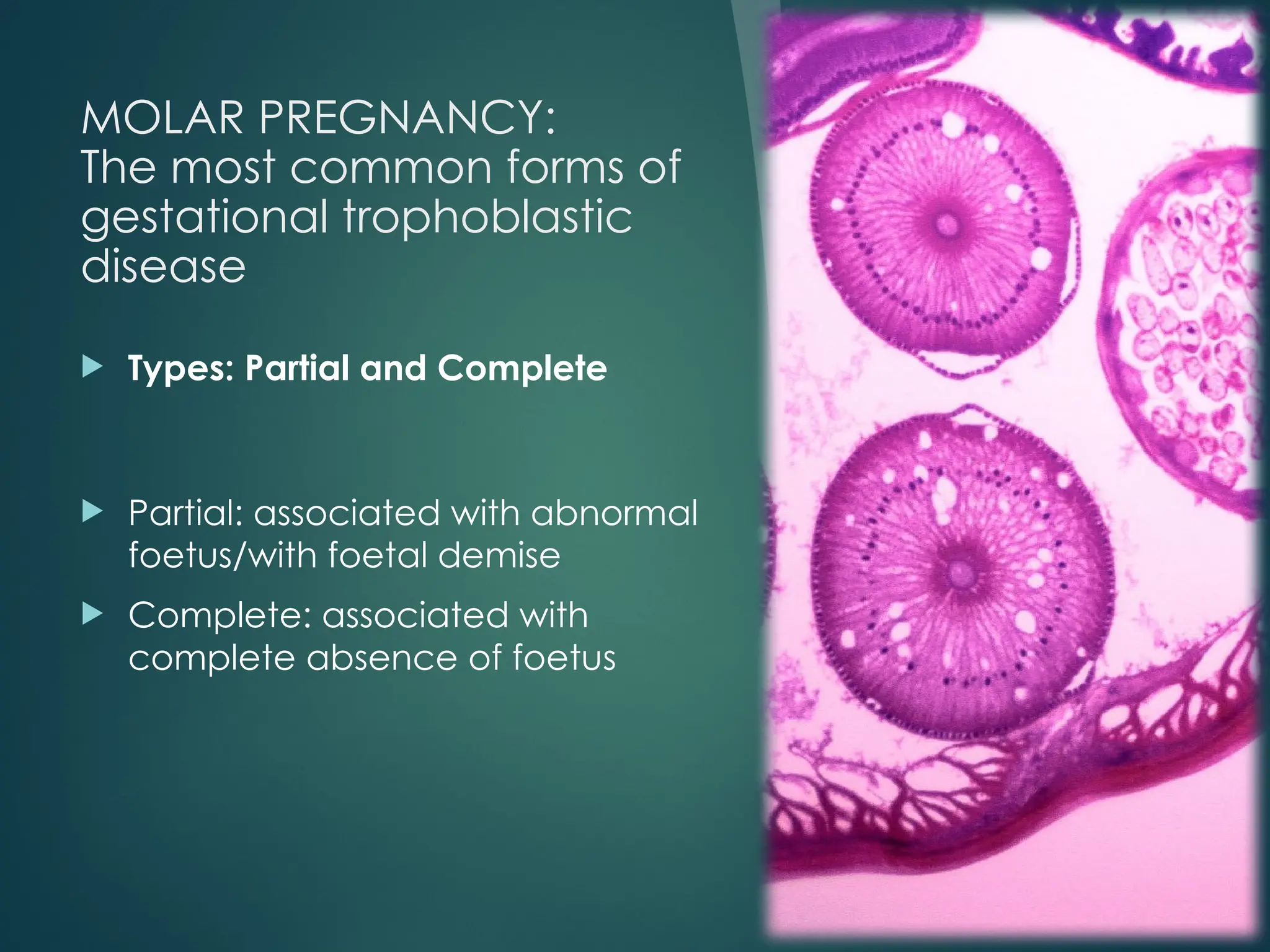
MOLAR PREGNANCY:
The mostcommon forms of
gestational trophoblastic
disease
Types: Partial and Complete
Partial: associated with abnormal
foetus/with foetal demise
Complete: associated with
complete absence of foetus
59.
Partial
Molar
Pregnancy
Greatly enlarged
placenta relative
tothe size of the
uterine cavity
Cystic spaces
within the
placenta
Amniotic cavity
either empty or
contains
amorphous small
foetal echoes
which may be
surrounded by
thick rim of
pacental echoes
Colour doppler
may show high
velocity and low
impedance flow
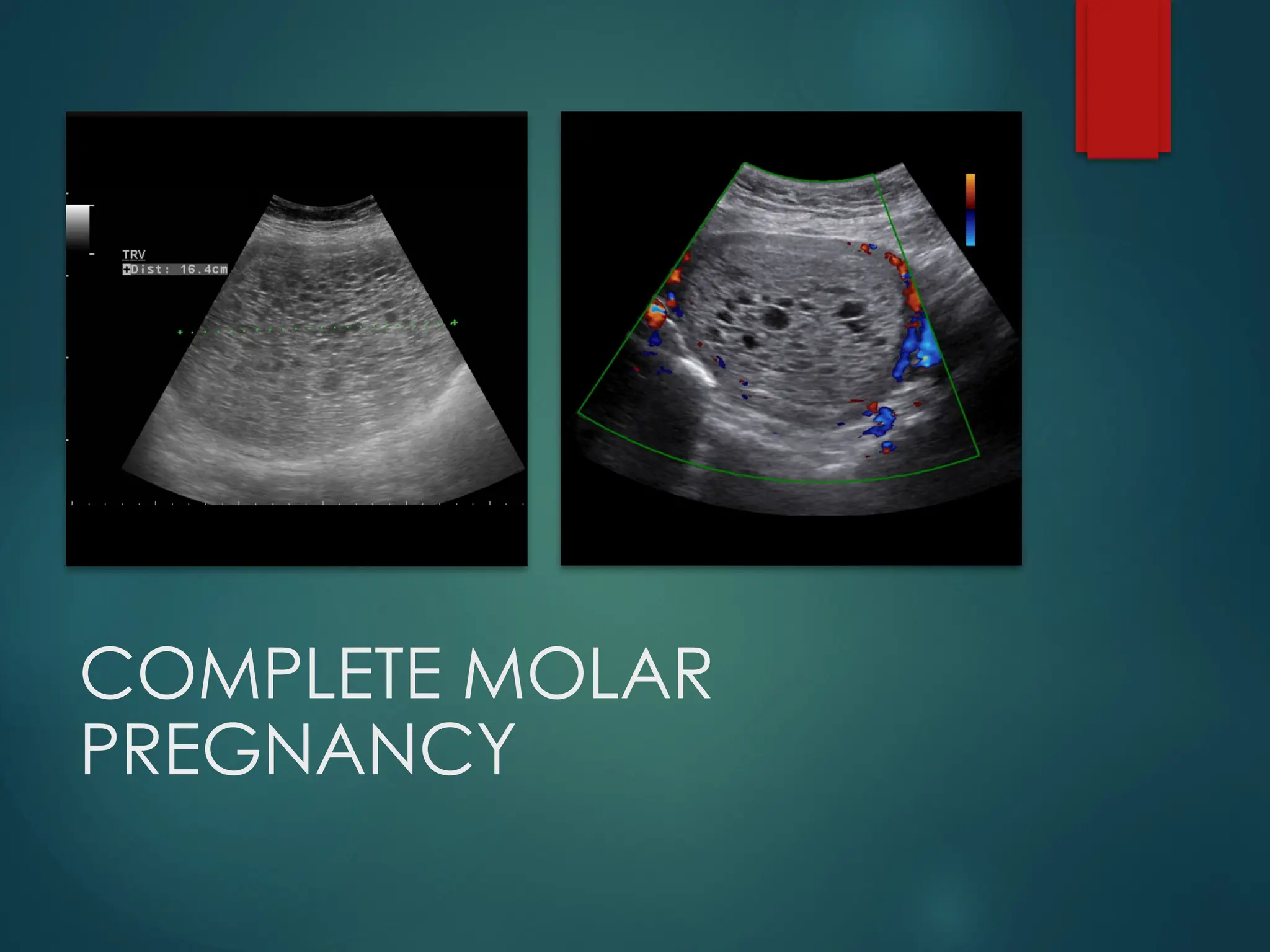
Complete
Molar
Pregnancy
Enlarged uterus
Intrauterine mass with multiple
cystic spaces without any
associated of foetal part or foetal
echoes often refer to as
“snowstorm” or “bunch of
grapes” appearance
Colour doppler shows high
velocity with low impedance flow
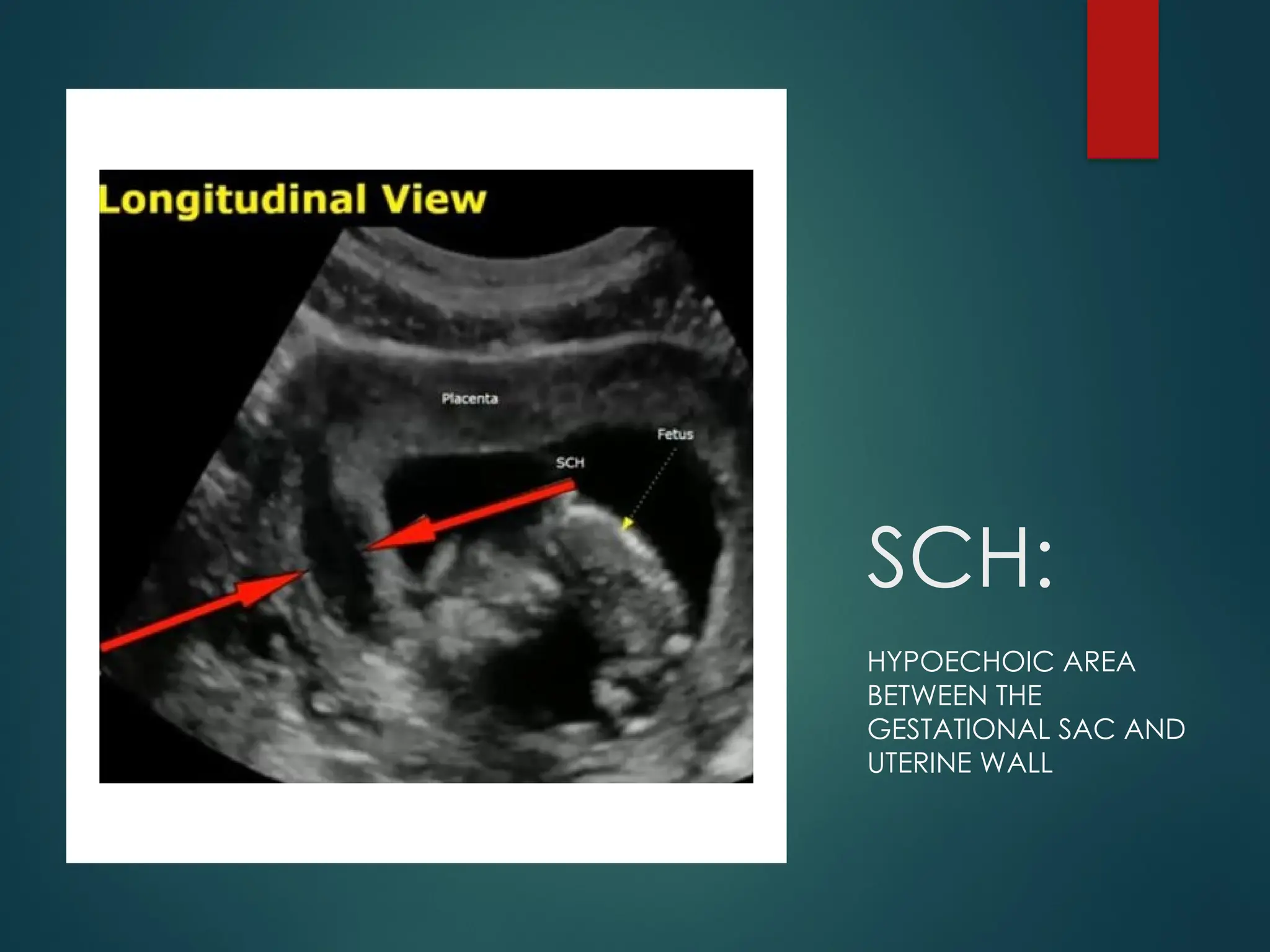
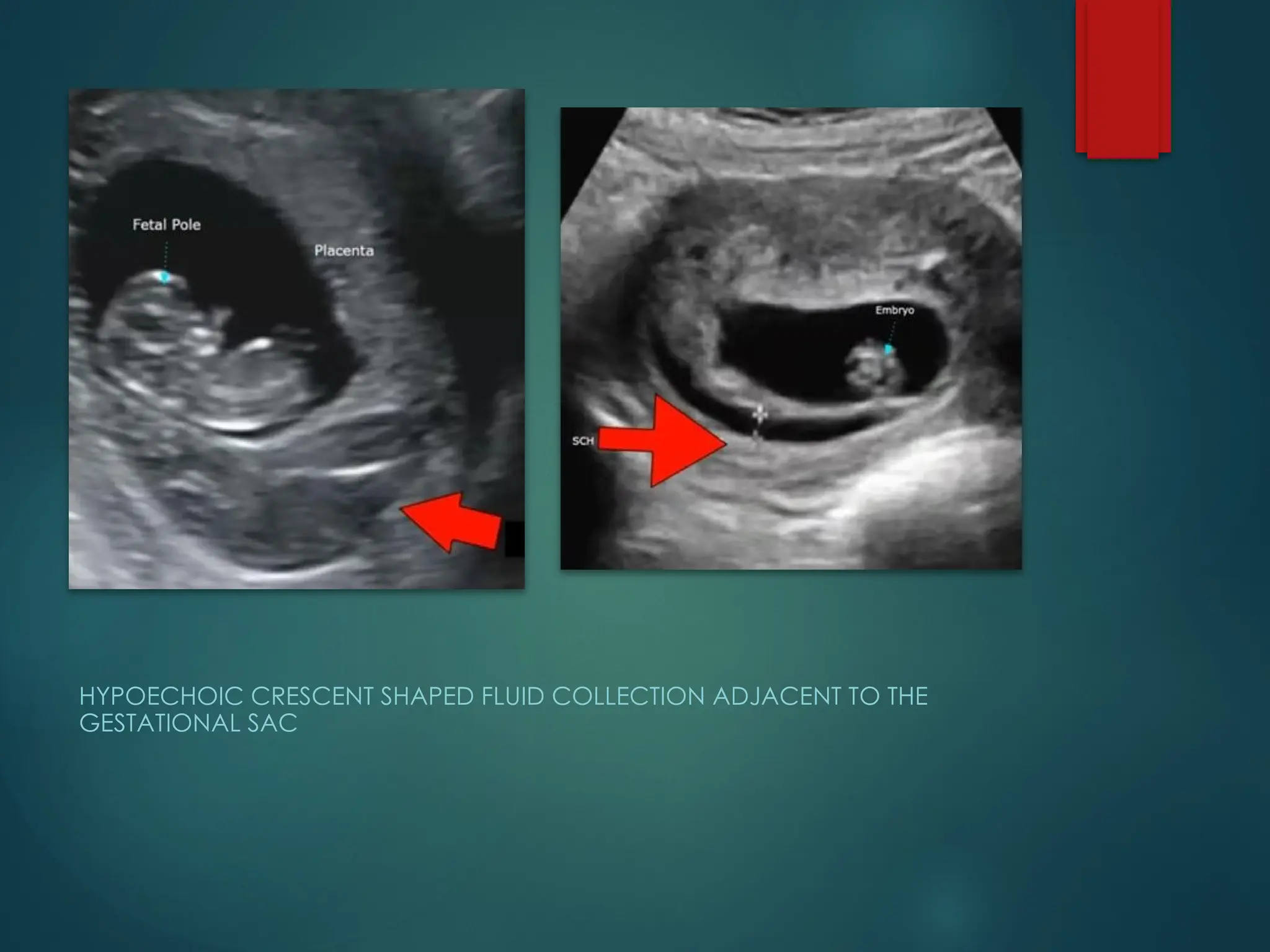
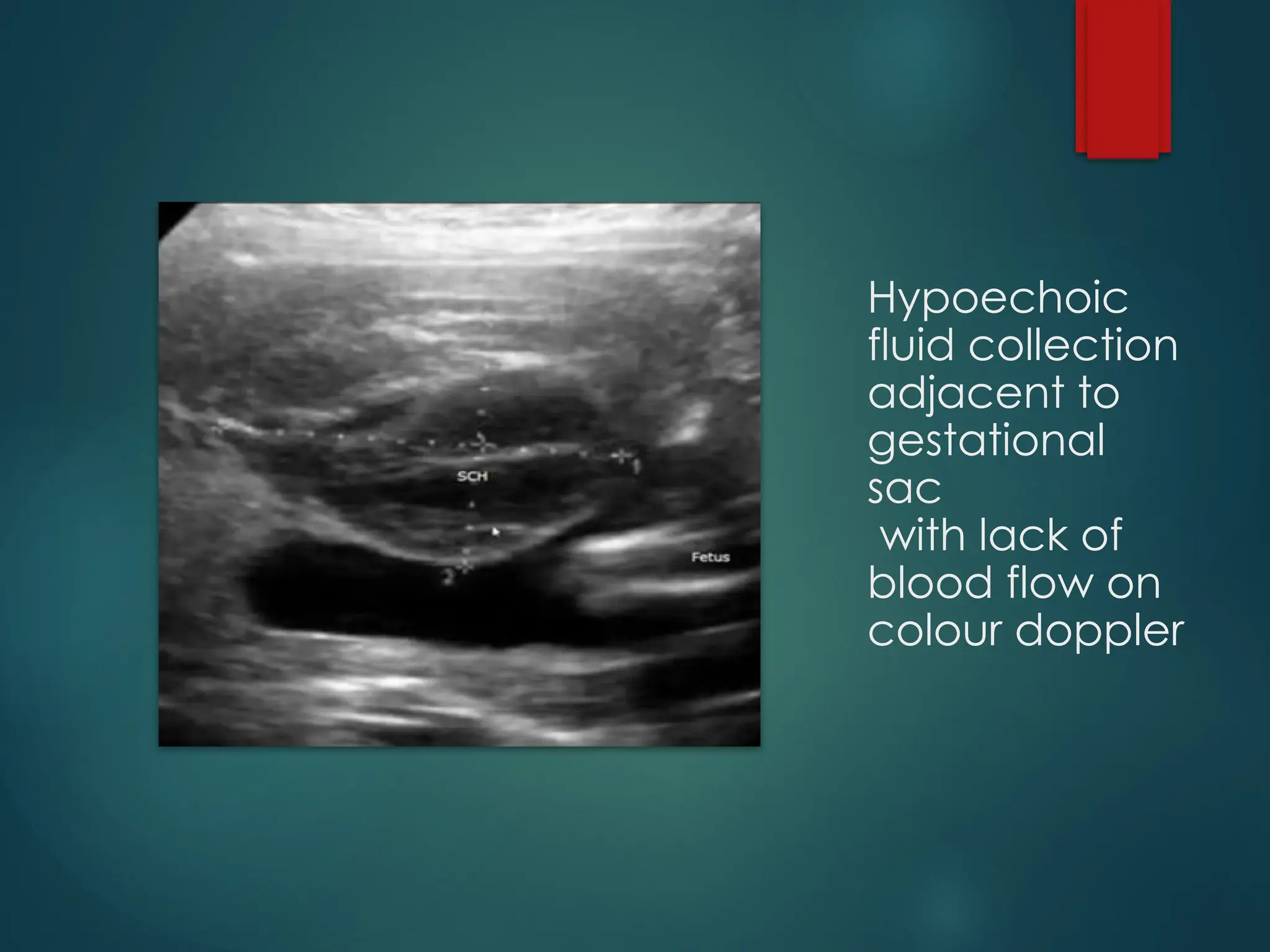
SUBCHORIONIC HAEMORRHAGE
Perigestationalhaemorrhage and blood
collection outsidre the gestational sac that
accumulates between the uterine wall and the
chorionic membrane in pregnancy
Frequent cause of bleeding in first trimester and
second trimester
Causes: Trauma, maternal conditions(clotting
disorders, hypertension, hormonal changes,
infections/inflamations, previous H/O SCH
Grading of
Subchorionic
Haemorrhaage:
SMALL: <20%of the size of
gestational sac
Medium: 20-50% of the size of
gestational sac
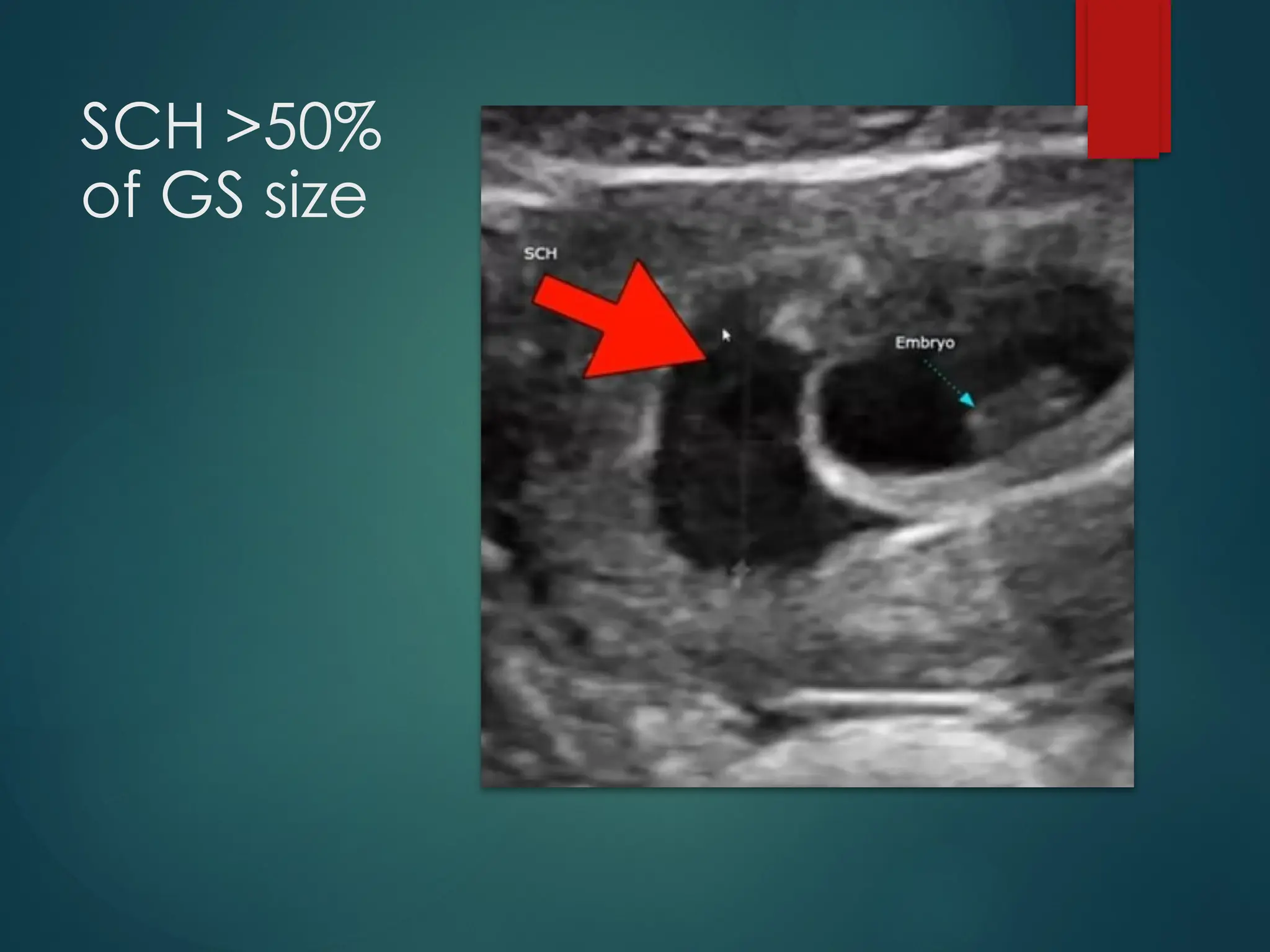
Large: >50% of the size of
gestational sac (higher risk of
complications such as
miscarriage)
MULTIFETAL PREGNANCY
Pregnancieswith more than one fetus have
become an increasingly common
Most multifetal pregnancies are twins
The rate of twins occurring naturally is 1 in 80 births
Multifetal pregnancies have higher rates of periatal
morbidity and mortality than singletons
• Chorionicity is the major determining feature for
the inherent unique complications faced by multiple
gestations
Fetal growth differences and congenital
malformations are increased in all types of multiple
gestations
72.
In monochorionictwins with a single demise, there
is a high risk of severe cerebral and other injuries in
the survivor
Sonography permits the diagnosis of syndromes
unique to monochorionic twins, including twin-
twin transfusion syndrome, twin anemia
polycythemia sequence, twin reversed arterial
perfusion sequence, and conjoined twin
73.
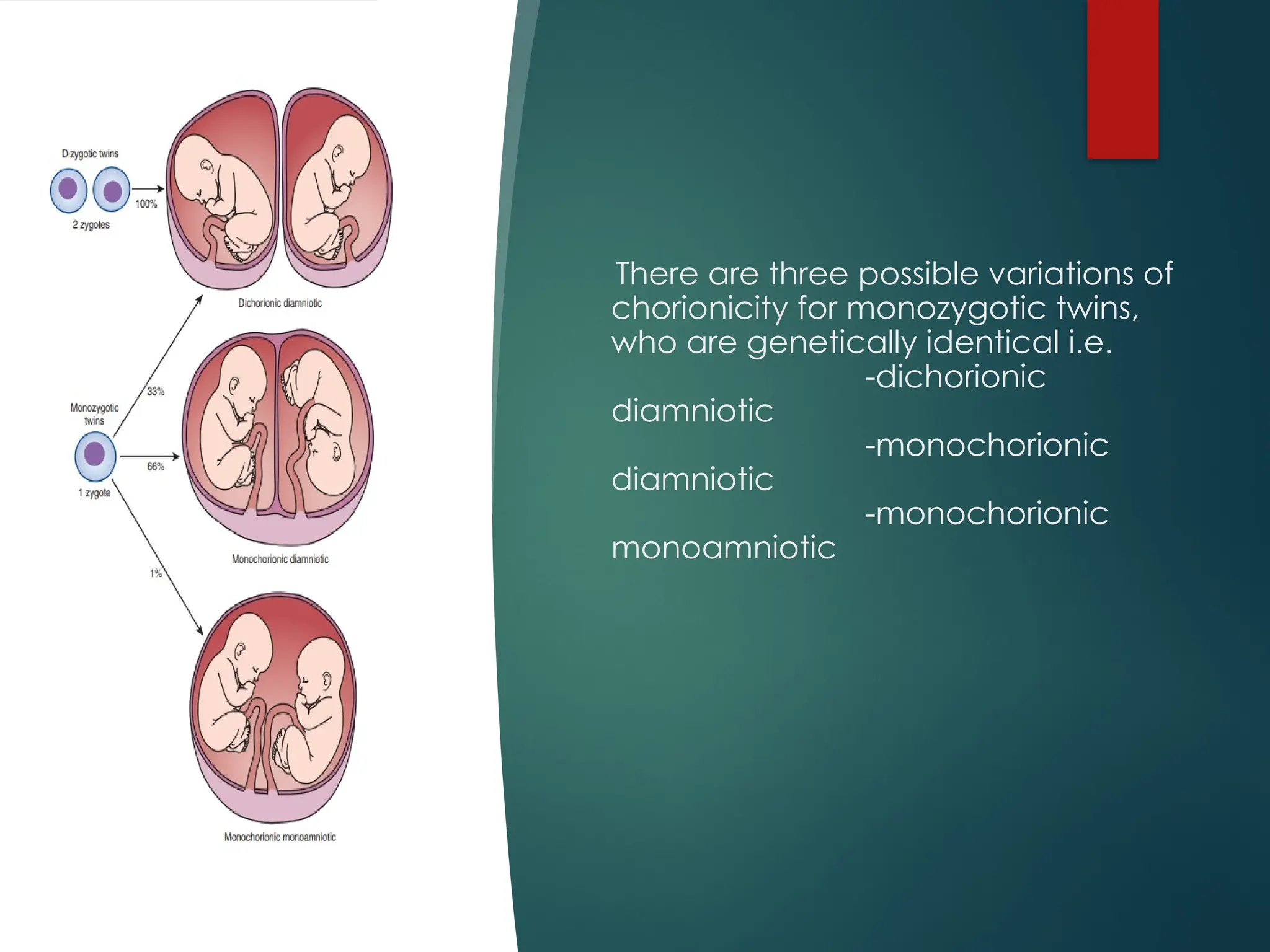
ZYGOSITY/CHORIONICITY
Twins areeither dizygotic or
monozygotic
Approximately two-thirds are
dizygotic and one-third are
monozygotic
Dizygotic twins occur when two
separate ova are fertilized by two
separate sperm
Monozygotic twins occur when a
single ovum is fertilized by a single
sperm
Dizygotic twins are always
dichorionic diamniotic, meaning
that each twin has its own
placenta (chorion), amnion and
amniotic fluid
74.
There are threepossible variations of
chorionicity for monozygotic twins,
who are genetically identical i.e.
-dichorionic
diamniotic
-monochorionic
diamniotic
-monochorionic
monoamniotic
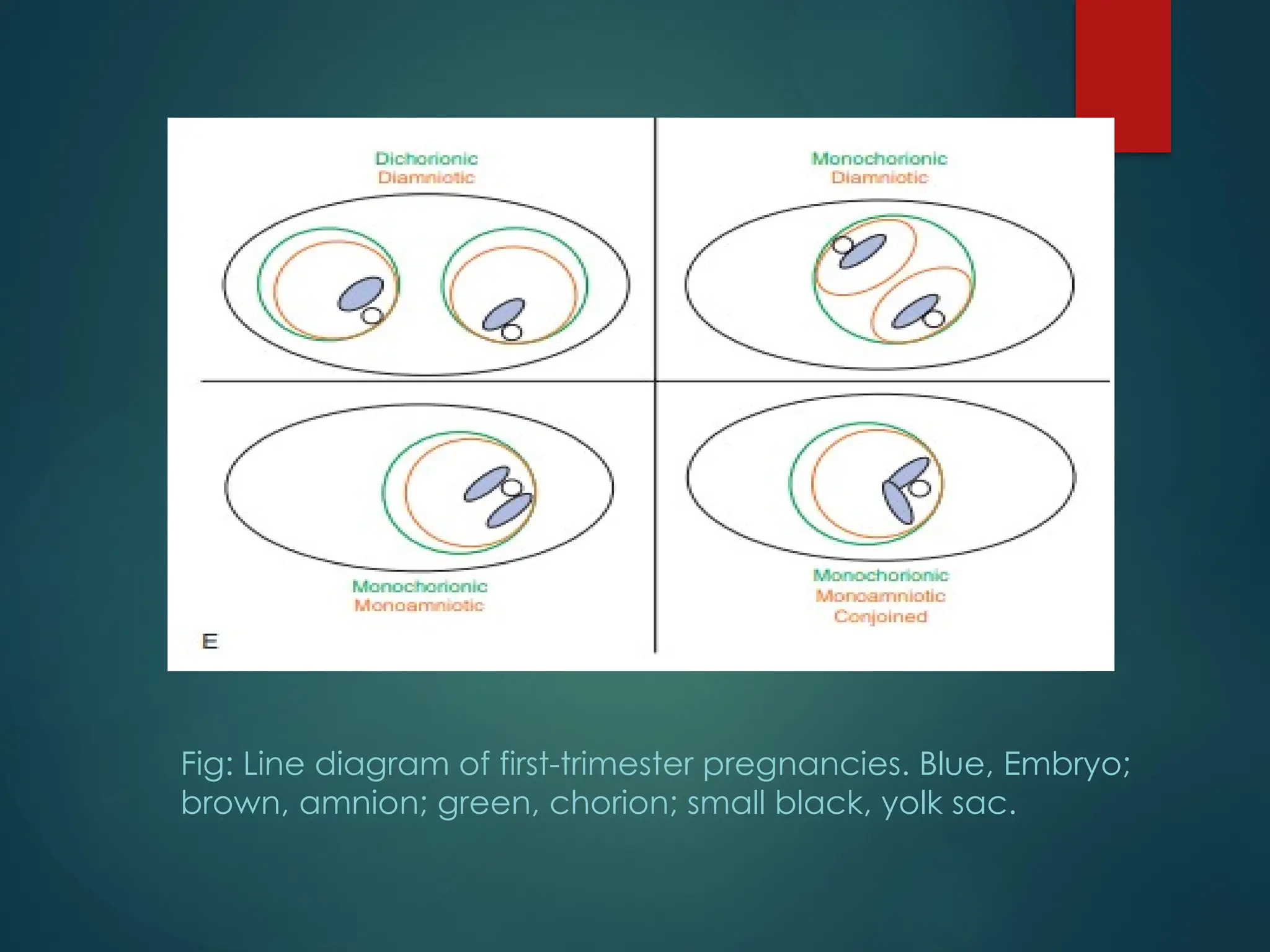
Fig: Line diagramof first-trimester pregnancies. Blue, Embryo;
brown, amnion; green, chorion; small black, yolk sac.
77.
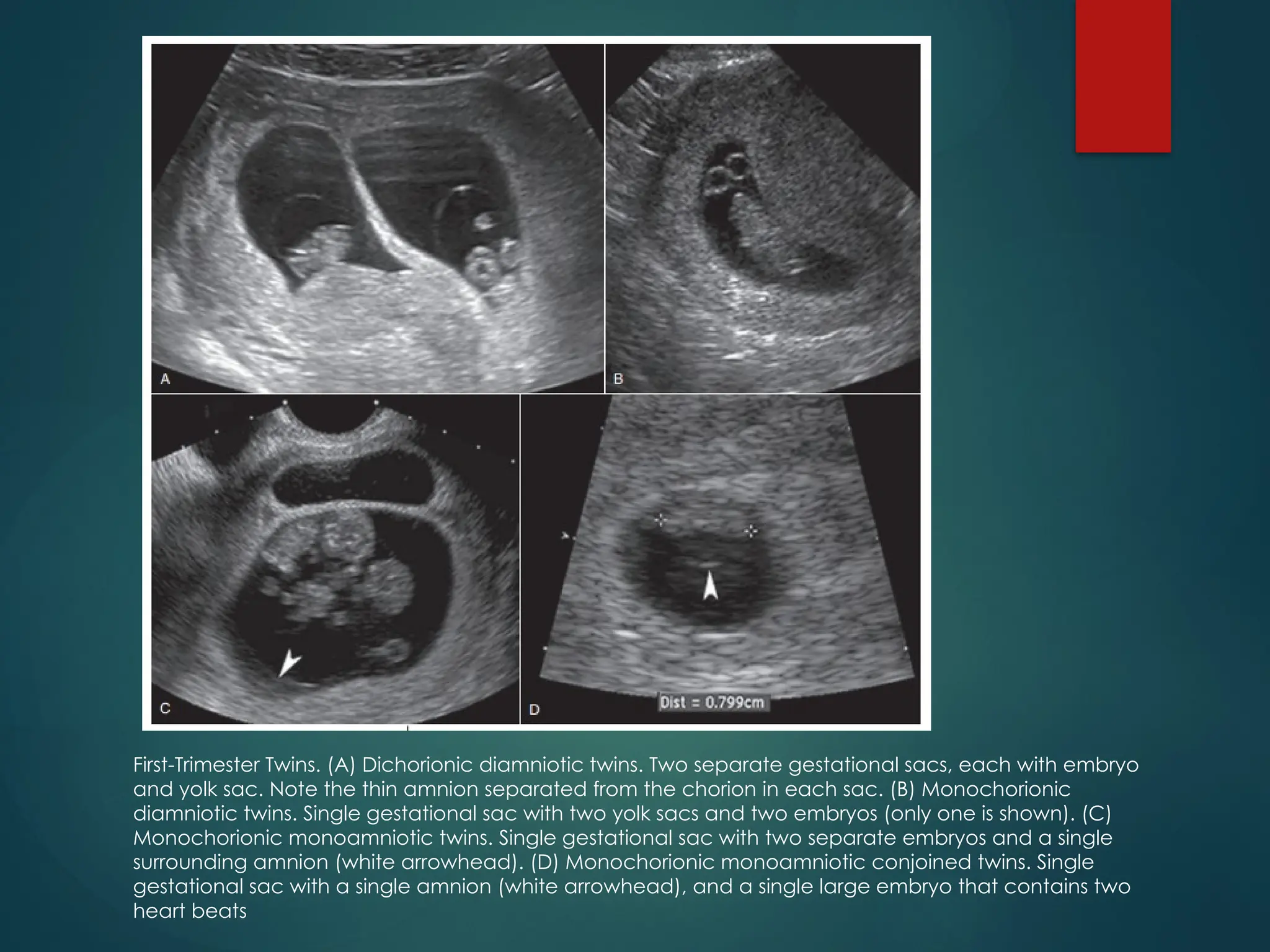
First-Trimester Twins. (A)Dichorionic diamniotic twins. Two separate gestational sacs, each with embryo
and yolk sac. Note the thin amnion separated from the chorion in each sac. (B) Monochorionic
diamniotic twins. Single gestational sac with two yolk sacs and two embryos (only one is shown). (C)
Monochorionic monoamniotic twins. Single gestational sac with two separate embryos and a single
surrounding amnion (white arrowhead). (D) Monochorionic monoamniotic conjoined twins. Single
gestational sac with a single amnion (white arrowhead), and a single large embryo that contains two
heart beats
78.
COMPLICATIONS OF MULTIFETAL
PREGNANCYIN FIRST TRIMESTER
Vanishing twin syndrome
Twin-twin transfusion syndrome
Conjoined twin
Discordant growth
Miscarriage(higher risk than singleton)
SCH
Chromosomal Anomalies(higher risk than
singleton)
79.
CONJOINED TWIN
Occurswhen monozygotic twin embryo fails to
fully separate after the day 14 post fertilization
Later the split, more fused the bodies will be
Conjoined twins can be diagnosed in the late first
trimester; however, a detailed survey will be
required by 18 to 20 weeks gestation for the most
accurate evaluation of the degree of visceral
and vascular sharing
REFERENCES
1. Diagnostic ultrasound5th
edition by
Carol Rumack Chapter 28 & 30
2. Textbook of ultrasound in obstetric
and gynaecology: practical
approach 1edition by Alfred
Abuhamad,MD Chapter 4
3. http://radiopaedia/articles/
4. http://nhmmeghalaya.nic.in/pcpndt
5. www.youtube.com/drsamimaginglibr
ary