Definition
• Tympanoplasty isa surgical procedure performed to eradicate disease from
the middle ear and reconstruct the hearing mechanism, with or without
repair of the tympanic membrane.
3.
• Aim ofTympanoplasty
• To eliminate middle ear disease
• To close tympanic membrane perforation
• To restore hearing
• To create a safe, dry ear
4.
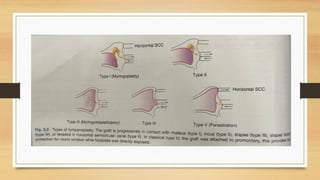
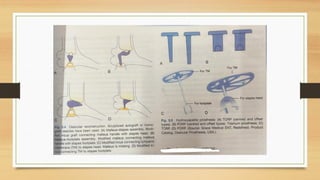
Types of tympanoplasty
TypeI – Myringoplasty
Only tympanic membrane perforation
• Ossicular chain intact
• Graft placed on TM
• Also called Myringoplasty
Type -II
• TM perforation + erosion of malleus
• Incus or malleus remnant
present
•Graft placed on incus or malleus remnant
5.
Type III –Myringostapediopexy
• Malleus and incus absent
• Stapes head present
• Graft placed directly on stapes head
• Also called Columella tympanoplasty.
Type IV
• Only stapes footplate present
• Graft placed between oval & round window
• Creates small middle ear cavity (cavum minor)
• Round window protected.
6.
Type V –Fenestration Operation
• Stapes footplate fixed
• Round window functioning
• New window created in lateral semicircular canal
• Covered with graft
• Now obsolete
8.
Several modifications haveappeared in above classification and they mainly
pertain to the types of ossicular reconstruction
• Ossicular Reconstruction
Importance
• • Ossicles transmit sound from tympanic membrane →
labyrinth
• Reconstruction restores conductive hearing
9.
Materials Used
• Autograftossicles – sculptured to bridge gap (preferred)
• Homograft ossicles – preserved ossicles ± TM
⚠ Risk of disease transmission, difficult to procure.
Prerequisites for Ossicular Reconstruction
• Healthy middle ear
• No mucosal disease or cholesteatoma
• Good Eustachian tube function
• Atelectatic middle ear → poor prognosis
10.
Timing of Reconstruction
•Delayed (≈ 6 months) after canal wall-up
mastoidectomy(to ensure ear is disease-free)
Primary Ossicular Reconstruction Done In
• Traumatic ossicular disruption
• Ossicular fixation
• Canal wall-down surgery without active disease
Advantages:
1. restoring thehearing loss and in some cases the tinnitus;
2. checking repeated infection from external auditory canal and eustachian tube
(nasopharyngeal infection ascends more easily via eustachian tube through
perforation )
3. checking aeroallergens reaching the exposed middle ear mucosa, leading to
persistent ear discharge.
16.
CONTRAINDICATIONS-
1.Active discharge fromthe middle ear.
2. Nasal allergy. It should be brought under control be-fore surgery
3. Otitis externa.
4. Ingrowth of squamous epithelium into the middle ear.
In such cases, excision of squamous epithelium from the middle ear
or a tympanomastoidectomy may be required.
17.
5. When theother ear is dead or not suitable for hearing aid rehabilitation.
6. Children below 3 years.
ANAESTHESIA
Local or general, the former is preferred
18.
Position -Supine withface turned to one side; the ear to be operated is up.
Graft materials used are:
1. Temporalis fascia (most common)
2. Areolar fascia overlying the temporal fascia
3. Perichondrium from the tragus
19.
4. Cartilage
5. Vein
6.Periosteum
Incision for exposure of tympanic membrane depends on the size of
the ear canal, it may be endomeatal , endaural or postaural.
20.
POSTOPERATIVE CARE
● Toensure the long-term success of the surgery, postoperative
care focuses on three primarary objectives:
● Graft Integration: Providing the stable environment necessary
for the graft to revascularize and
● Infection Control: Maintaining sterility to prevent middle ear
infections that could liquefy the graft.
21.
● Vigilant Monitoring:Early identification of complications
such as graft displacement or middle ear fluid buildup.
Postoperative Timeline & Protocol.
● Suture Management: External skin stitches are removed
between days 5 and 6.
● Internal Debridement: The ear canal pack (used for
stabilization) is carefully removed on day 5 to avoid mechanical
displacement of the graft.
22.
● Follow-up Schedule:1Week: Assessment of the surgical site
and canal healing.
● 6 Weeks: Evaluation of graft stability and initial hearing
improvement.
● Healing Maturity: Complete epithelialization (the growth of
skin over the graft) typically requires 6–8 weeks.
23.
COMPLICATIONS
● Complications aretechnically driven and differ significantly
based on the surgical approach:
■ Underlay Technique: Graft is placed medial to the tympanic
membrane remnant and the malleus handle.
■ Overlay Technique: Graft is placed lateral to the fibrous layer of
the remnant.
24.
UNDERLAY TECHNIQUE
● UnderlayTechnique Complications
●Medialization: The graft sits too deep in the middle ear,
reducing the air-filled space and potentially impacting sound
resonance.
● Promontory Adherence: The graft may adhere to the medial
wall (promontory), tethering the ossicular chain and causing
conductive hearing loss.
25.
● Anterior Failure:The most common failure point; the graft loses
contact at the anterior margin, leading to a residual anterior
perforation.
26.
OVERLAY TECHNIQUE
●Overlay TechniqueComplications
●Anterior Blunting: Thickening of tissue at the anterior sulcus,
which obscures the drum and hampers sound conduction.
●Anterior Blunting: Thickening of tissue at the anterior sulcus,
which obscures the drum and hampers sound conduction
● Epithelial Pearls: Squamous skin cells trapped under the graft
can form iatrogenic cholesteatomas (pearls)
27.
● Lateralization: Thegraft pulls away from the malleus handle.
This creates a gap that prevents sound vibrations from reaching
the inner ear.
● Prevention: Securely tucking the graft under the malleus
handle is critical.
28.
OTHER PROCEDURES FORCLOSURE OF
TYMPANIC MEMBRANE PERFORATION
Alternative methods are used for small perforations or
cases where major reconstructive surgery is not
immediately indicated.
29.
Selection Criteria:
● Perforationsize is small.
● Surgery is not immediately required or appropriate.
● Applicable for both fresh traumatic and long-standing chronic
perforations.
Primary Techniques:
● Splintage
●Cautery Patching
● Fat-Graft Myringoplasty
30.
1. SPLINTAGE
● Indications:Primarily used for fresh traumatic tympanic
membrane perforations.
● Procedure:
● Torn edges of the perforation are carefully everted (turned
outward) using a microscope.
● Absorbable gelfoam is placed into the middle ear through the tear
for support.
31.
●Outer Surface Splinting:For smaller tears, the outer surface is
splinted with:
●Cigarette paper
●Gelfilm
● Silicone sheet
32.
2. CAUTERY PATCHING
Indications:
●Small, long-standing central perforations.
●Chronic cases where margins have become epithelialized (skin
has grown over the edges, preventing natural closure).
33.
Procedure Steps:
● Freshening:Margins are cauterized with 50% trichloroacetic acid
to remove epithelialized edges, or freshened with a fine pick.
● Support: Perforation is supported with cigarette paper moistened
with 1% phenol in glycerine Follow-up: The procedure can be
repeated at 2 week intervals. Alternative Materials: Steristrip,
Gelfilm, or silicone sheets.
● Follow-up: the procedure can be repeated at 2 week intervals.
34.
3.FAT-GRAFT MYRINGOPLASTY
Indications: Small,long-standing central perforations.
Chronic cases where margins have become epithelialized (skin
has grown over the edges, preventing natural closure).
35.
TECHNIQUE:
● Performed underlocal anesthesia. Edges of the perforation
are freshened using a 1 mm stapes hook. The inside of the
perforation is also scraped to promote healing
36.
The Graft:
A smallpiece of fat is harvested from the ear lobule. The fat is
plugged into the perforation like an hour-glass.
Outcome: Over time, the fat graft adheres and successfully
close the perforation










![Untitled (6) [Autosaved] ear.pptx ear surgeries](https://cdn.slidesharecdn.com/ss_thumbnails/untitled6autosavedear-251128030434-d7ae6d96-thumbnail.jpg?width=640&height=640&fit=bounds)






































