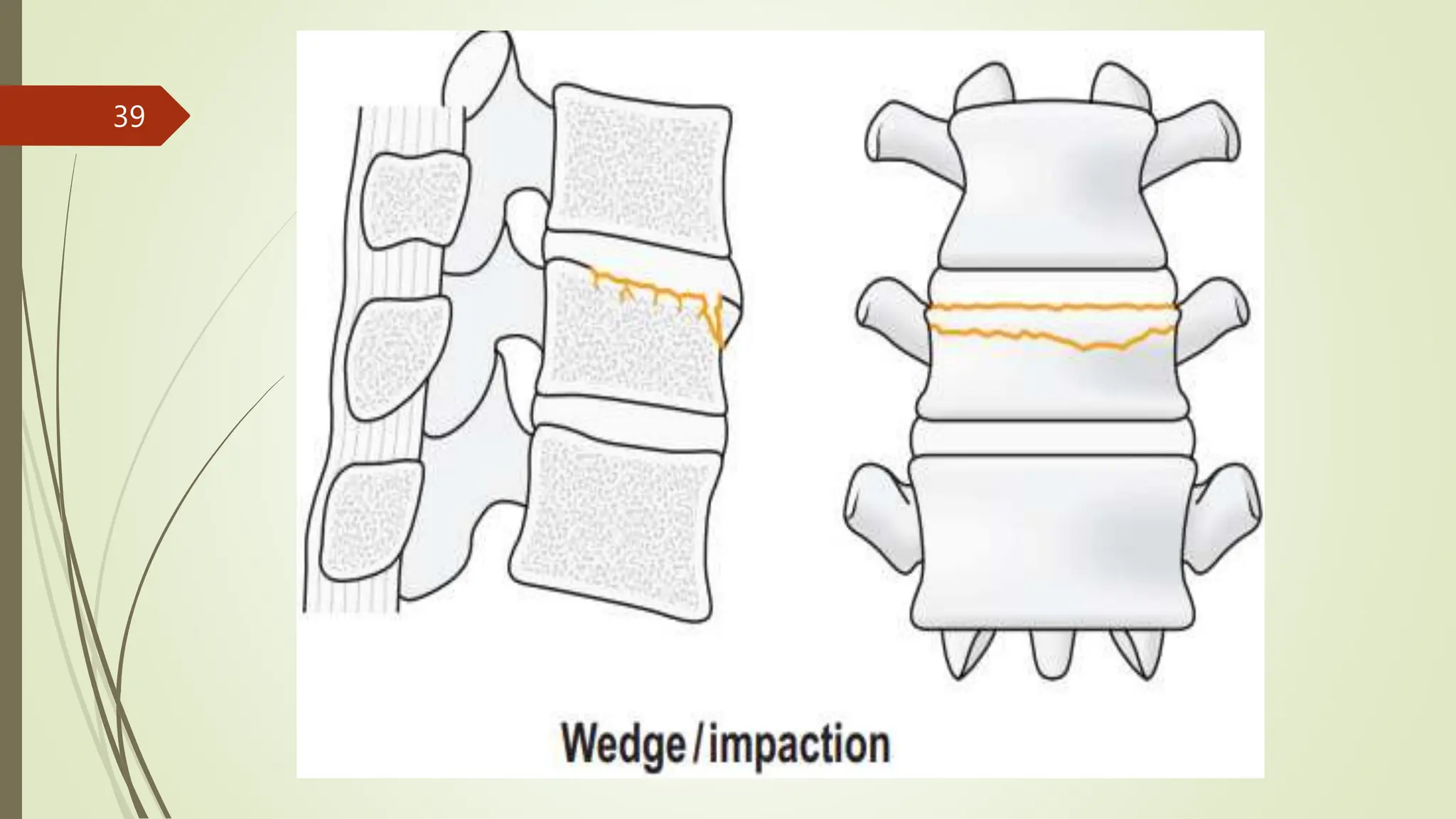
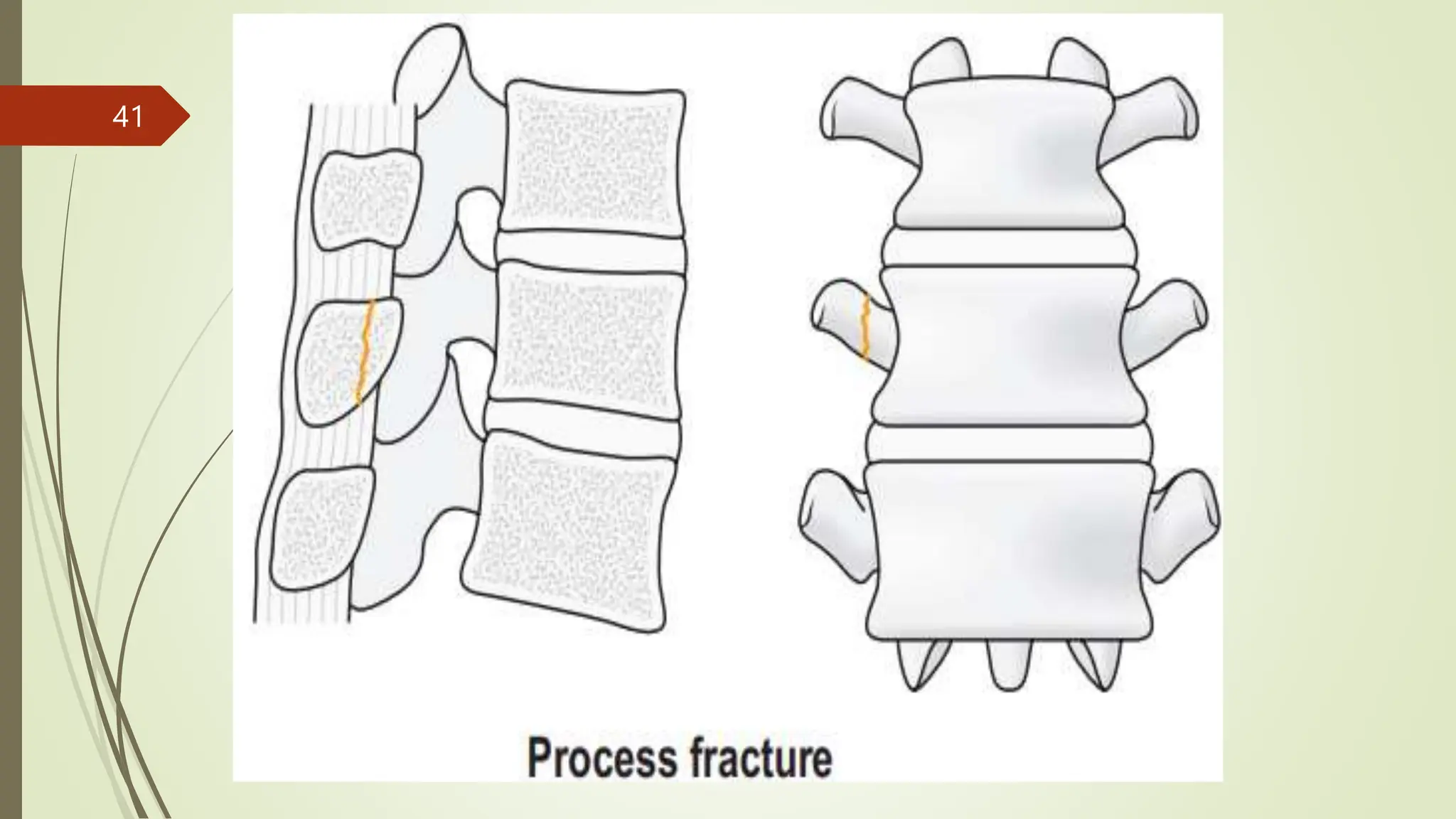
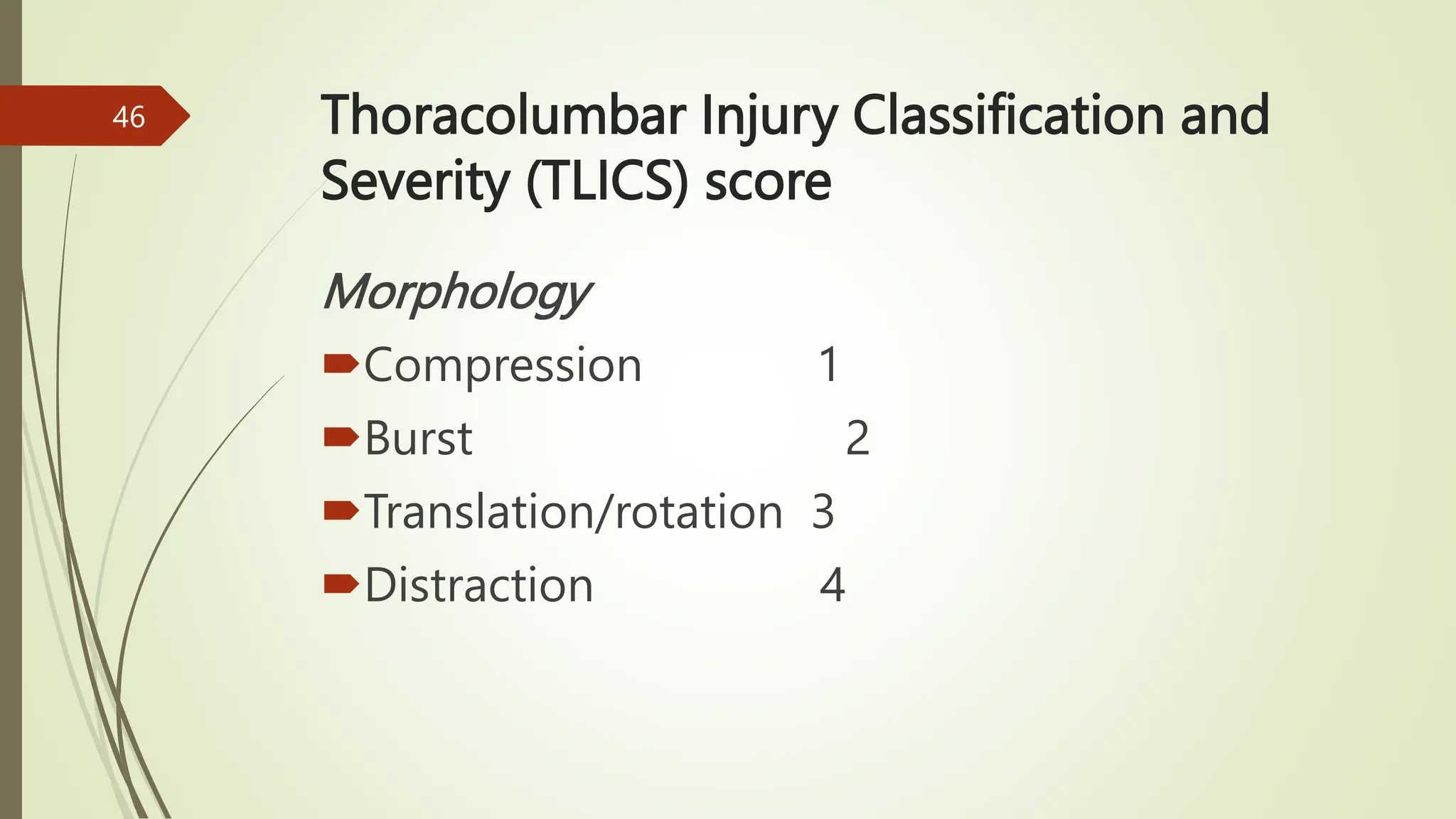
The document outlines a course on traumatology, focusing on the anatomy and common injuries of the thoracolumbar region, particularly whiplash injuries and fractures. It details clinical features, investigations, classifications, management strategies, and the importance of addressing neurological status in treatment. Key topics include non-operative and operative management of thoracolumbar injuries, along with references for further reading.