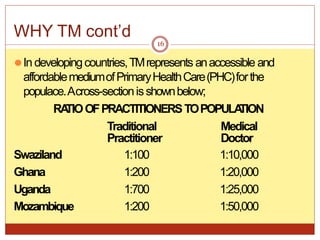
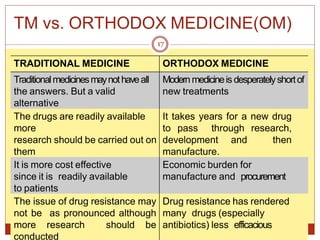
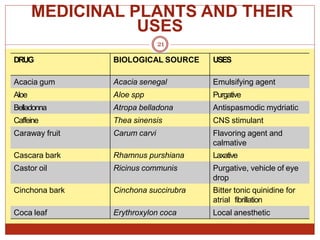
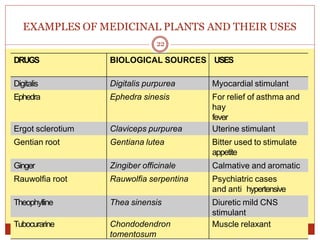
This document discusses traditional medicines, providing definitions, a brief history, descriptions of traditional medicine practices from various regions, profiles of traditional healers, comparisons to orthodox medicines, arguments for and against traditional medicines, examples of medicinal plants and their uses, and conclusions. The key information presented includes that traditional medicines have been used for millennia, rely on plant and animal-based remedies, and are still widely used today, especially in developing countries where access and cost are significant factors. However, issues regarding safety, efficacy, and quality need further research and regulation.