The document discusses the anatomy and clinical applications of the tracheobronchial tree and upper airway, including detailed descriptions of the nasal cavity, pharynx, larynx, trachea, and bronchial structures. It outlines blood supply, nerve innervation, and important clinical implications for procedures such as tracheostomy and endotracheal intubation, particularly in infants and children. It emphasizes the significance of understanding the anatomical relationships and respiratory functions in medical practice.
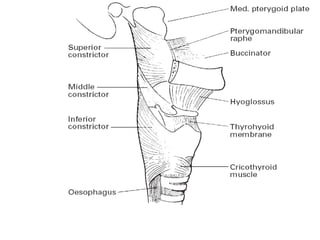
![PHARYNX
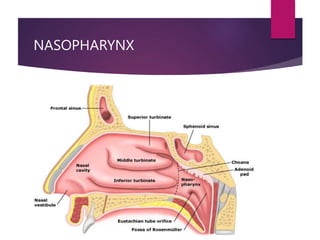
NASOPHARYNX
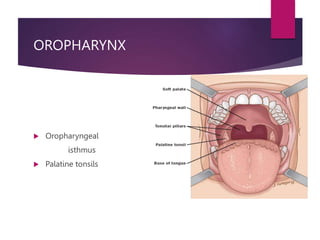
OROPHARYNX
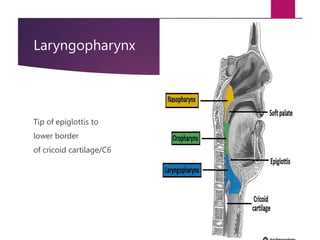
LARYNGOPHARYNX
Extends from basilar part of occipital bone
of skull to origin of the esophagus
(lower part of cricoid cartilage/ C6 vertebra)
12-15cm long
Widest-hyoid bone[5cm]
Narrowest-pharyngo-oesophageal jn[1.5cm]
DEVELOPMENT-cranial most part of foregut](https://image.slidesharecdn.com/topictracheobronchialtreeupperairway-240615153134-83d3357b/85/topic-tracheobronchial-tree-upper-airway-pptx-15-320.jpg)
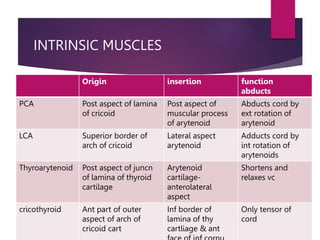
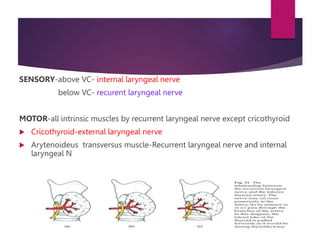
![Abductors of cords- PCA
Adductors of the cords- LCA, Interarytenoides
Tensor of VC-Cricothyroid
only intrinsic muscle lies outside
cartilagenous framework
Regulators of cord tension
cricothyroid(tensor)
thyroarytenoid(relaxor)
vocalis(fine adjustment[relax])](https://image.slidesharecdn.com/topictracheobronchialtreeupperairway-240615153134-83d3357b/85/topic-tracheobronchial-tree-upper-airway-pptx-44-320.jpg)
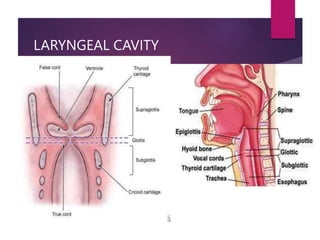
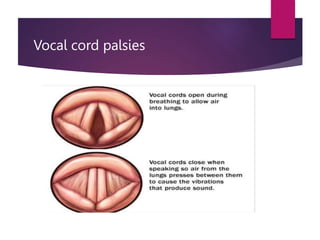
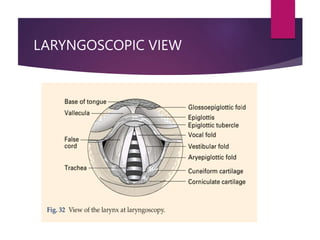
![Vocal cord
Pearly white folds of mucous membrane
Angle of thyroid cartilage to vocal process of arytenoid
Narrowest part of laryngeal cavity
Stratified squamous epithelium[larynx-ciliated columnar
epithelium]
No submucosa with blood vessels
No mucous glands](https://image.slidesharecdn.com/topictracheobronchialtreeupperairway-240615153134-83d3357b/85/topic-tracheobronchial-tree-upper-airway-pptx-52-320.jpg)