Background:-
• Evaluation ofdemographic, etiological, and clinical
properties of neuro-ophthalmological diseases in
childhood.
• Treatment modalities of neuro-ophthalmological
diseases in childhood.
• Limited information regarding the neuro-
ophthalmological diseases in young ages.
• Genetic & socioeconomic conditions and limited
access to medical centers may result in variability to
diagnose neuro-ophthalmological cases.
3.
Aim of Thisstudy
• Evaluation of causes.
• Finding the clinical characteristics.
• And tracing out the natural courses of neuro-
ophthalmological diseases among children.
4.
• Detailed history,
demographicand clinical
data were recorded.
• Systemic diseases
evaluated and treatment
protocols were set.
• Neuro-ophthalmological
examinations were
performed.
• Diagnosis and follow up
visits were recorded.
Materials and methods
• Retrospective study.
• Study Place:- Ulucanlar
Eye Hospital, Turkey.
• Study period - From
2004 to 2019.
• Patients age was
considered.
• Study protocol was
approved by ethics
committee.
5.
Inclusion criteria
• Agebelow 18 years.
• Changes of visual acuity.
• Abnormalities in pupillary light reaction.
• Abnormalities in slit-lamp examination.
• Abnormalities in fundus examination.
• History of Strabismus.
• Abnormal color vision test.
• Associated systemic diseases.
6.
Exclusion criteria
• Patientwith age more than 18 years.
• Referred patients with other than neuro-
ophthalmological abonrmalities.
7.
Data collection
• Ophthalmological
examination
Visualacuity test
Color vision test
Pupil examination
Slit-lamp examination
Ocular motility test
Fundoscopy
IOP measurement
Visual Field testing
• Systemic examination
Pulse, BP check in suitable
patient
Blood sugar level
Lipid profile test in selected cases
Other immuno biochemistry in
selected cases
Infection & immune marker tests
in selected cases
Neurological and imaging study
CSF study
8.
Neuro-ophthalmological Data
collection
• Best-correctedvisual acuity (BCVA) with Snellen chart.
• Number of visits during the follow-up period.
• Color vision testing with Ishihara’s pseudoisochromatic color
vision chart.
• Pupillary light reflexes evaluation.
• Evaluation of RAPD/APD.
• Pupillary diameters were measured with the pupil gauge
chart in both dim and bright light
9.
Neuro-ophthalmological data
collection
• Extraoculareye movements were recorded in nine
cardinal positions.
• Detailed Anterior segment examination.
• Dillated fundus examination with a 90-diopter lens
or indirect ophthalmoscopic examination with a 20-
diopter lens were performed.
10.
Neuro-ophthalmological data
collection
• Humphrey30-2 or 24-2 visual field test were
performed by automatic perimetry.
• Where Humphrey couldn't performed due to
patient age and cooperation problems, VF was
assessed by a confrontation test.
• VEP was performed in patients suspected of optic
nerve and visual pathway damage.
• MRI & MRV were done.
• LP done by paediatric neurologist for CSF Ex
11.
Data compilation
• Allstatistical analyses were carried out using the
SPSS 21.0 statistical analysis program.
• SPSS is a widely-used software for advanced
statistical analysis, data management, and data
visualization developed by IBM.
• The descriptive statistics mean or median values,
and percentages were obtained in the analysis.
12.
Result
• Among 1,910number of
patients 128 (6.7%) were
younger than 18 years old.
• Mean age of onset was 11.9
± 3.5 years.
• Race :- Turkish Caucasians.
• 71(57.5%) girls and
57(44.5%) boys.
13.
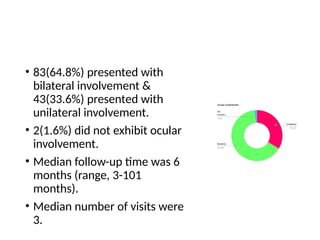
• 83(64.8%) presentedwith
bilateral involvement &
43(33.6%) presented with
unilateral involvement.
• 2(1.6%) did not exhibit ocular
involvement.
• Median follow-up time was 6
months (range, 3-101
months).
• Median number of visits were
3.
14.
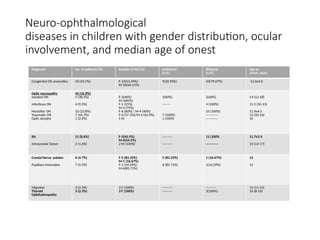
Neuro-ophthalmological
diseases in childrenwith gender distribution, ocular
involvement, and median age of onest
Diagnosis No. of patients (%) Gender (F/M) (%) Unilateral
(n,%)
Bilateral
(n,%)
Age at
onset, years
Congenital OD anomalies 43 (33.5%) F-23(53.49%)
M-20(46.51%)
9(20.93%) 34(79.07%) 12.0±3.0
Optic neuropathy
Isolated ON
Infectious ON
Herediter ON
Traumatic ON
Optic atrophy
42 (32.8%)
5 (38.5%)
4 (9.5%)
10 (23.8%)
7 (16.7%)
1 (2.4%)
F-2(40%)
M-3(60%)
F-1 (25%)
M-3 (75%)
F-6 (60%) / M-4 (40%)
F-4 (57.1%)/M-3 (42.9%)
1 M
3(60%)
-------
7 (100%)
1 (100%
2(40%)
4 (100%)
10 (100%)
-----------
-----------
14 (12-18)
11.5 (10-13)
11.9±4.5
12 (10-16)
10
IIH
Intracranial Tumor
11 (8.6%)
2 (1.6%)
F-5(45.5%)
M-6(54.5%)
2 M (100%)
---------
---------
11 (100%
-----------
11.7±3.9
15 (13-17)
Cranial Nerve palaies
Pupillary Anomalies
6 (4.7%)
7 (5.5%)
F-5 (83.33%)
M-1 (16.67%)
F-1 (14.29%)
M-6(85.71%)
5 (83.33%)
6 (85.71%)
1 (16.67%)
1(14.29%)
12
12
Migraine
Thyroid
Ophthalmopathy
3 (2.3%)
3 (2.3%)
3 F (100%)
3 F (100%)
---------
---------
---------
3(100%)
15 (11-15)
16 (8-16)
15.
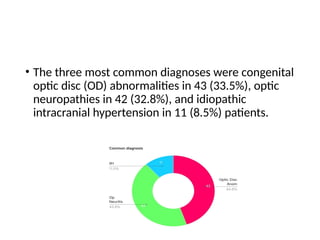
• The threemost common diagnoses were congenital
optic disc (OD) abnormalities in 43 (33.5%), optic
neuropathies in 42 (32.8%), and idiopathic
intracranial hypertension in 11 (8.5%) patients.
16.
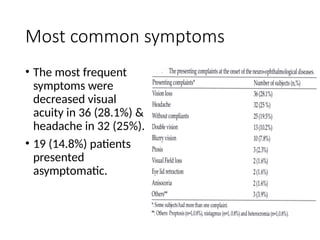
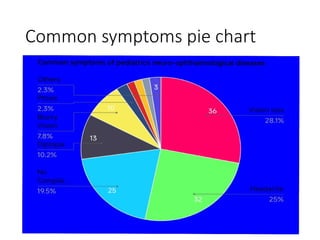
Most common symptoms
•The most frequent
symptoms were
decreased visual
acuity in 36 (28.1%) &
headache in 32 (25%).
• 19 (14.8%) patients
presented
asymptomatic.
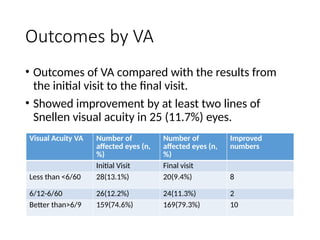
Outcomes by VA
•Outcomes of VA compared with the results from
the initial visit to the final visit.
• Showed improvement by at least two lines of
Snellen visual acuity in 25 (11.7%) eyes.
Visual Acuity VA Number of
affected eyes (n,
%)
Number of
affected eyes (n,
%)
Improved
numbers
Initial Visit Final visit
Less than <6/60 28(13.1%) 20(9.4%) 8
6/12-6/60 26(12.2%) 24(11.3%) 2
Better than>6/9 159(74.6%) 169(79.3%) 10
• All paralyticcranial nerve cases completely
recovered during follow-up period.
• All patients with traumatic optic neuropathy were
caused by blunt trauma.
• The VA decreased in 16 (7.5%) and remained
unchanged in the other 172 (80.7%) eyes.
21.
Study observation
• Neuro-ophthalmologicdiseases vary from life-
threatening intracranial or systemic diseases to
congenital disc anomalies.
• Having a long-term effect on the visual system.
• Having an impact over development of a child.
• Loss of vision at an early stage of life, has a negative
impact on neuro-behavioral development.
22.
Study observation
• Earlydiagnosis of neuro-ophthalmological diseases
is significant.
• Mostly disorders are treatable and preventable.
• Rate of prevalence of treatable diseases is 25.7% in
school-aged children.
• More than half of optic nerve disease cases could
be treatable at an early stage.
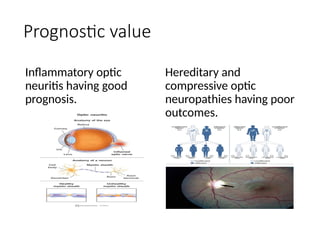
23.
Preventable neurological diseases
•Secondary optic atrophies.
• Traumatic cortical blindness.
• Traumatic Retinal detachment.
• Cataract secondary to intrauterine infections.
• Optic nerve disease treatable at an early stage, i.e.
Inflammatory optic neuritis, Glaucomatous optic
neuropathies, IIH, nutritional & Toxic optic
neuropathies.