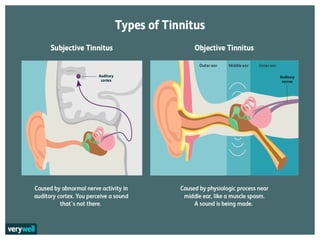
Tinnitus is described as a ringing or noise in the ear. It can be subjective, only heard by the patient, or objective, audible to an examiner. Causes include ear issues, neurological conditions, cardiovascular problems, and medications. Treatments include addressing underlying causes, sound therapy like hearing aids, and tinnitus retraining therapy which aims to reduce negative reactions to tinnitus through counselling and sound exposure.