














![POSTERIOR BORDER
Separates medial surface
from posterolateral surface
Related to:
Anastomosis of sup. & inf.
thyroid arteries
Parathyroid glands (superior
& inferior)
[Sup. parathyroid at the level
of C6 (cricoid)
Inf. parathyroid at lower pole
of gland]
On left side thoracic duct
(lower part)
© Dr.N.Mugunthan](https://image.slidesharecdn.com/thyroidgland-prof-250526085648-abd19fbd/75/THYROID-GLAND-Prof-Dr-N-Mugunthan-KMMC-Muttom-32-2048.jpg)





















![Parafollicular C cells
O Polyhedral cells with oval
nucleus
O Paler & larger than thyroid
follicular cells
O Present between basement
membrane and the
follicular cell
O Secretes - Thyrocalcitonin
[lowers the blood calcium
level]
© Dr.N.Mugunthan](https://image.slidesharecdn.com/thyroidgland-prof-250526085648-abd19fbd/75/THYROID-GLAND-Prof-Dr-N-Mugunthan-KMMC-Muttom-55-2048.jpg)








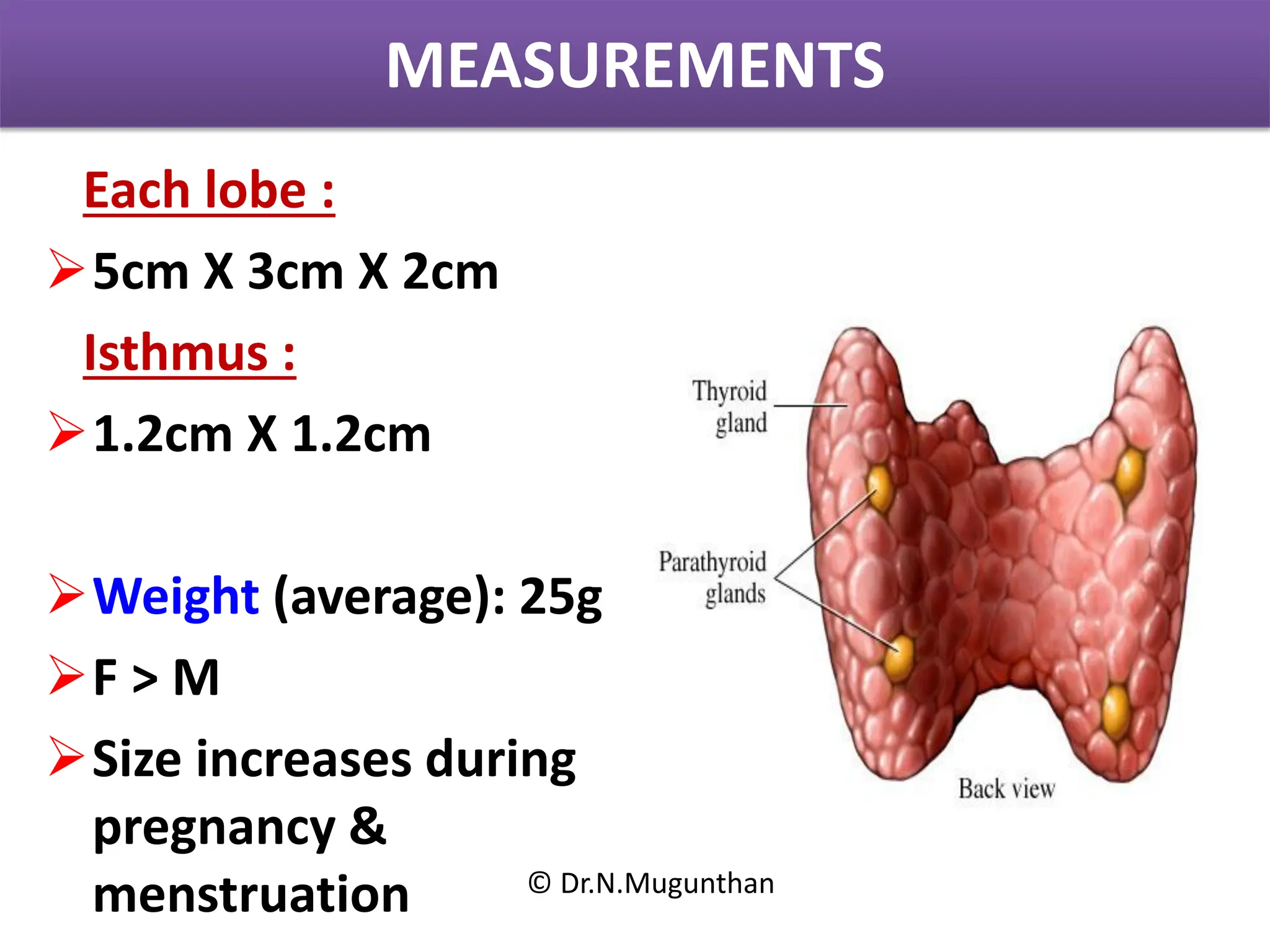
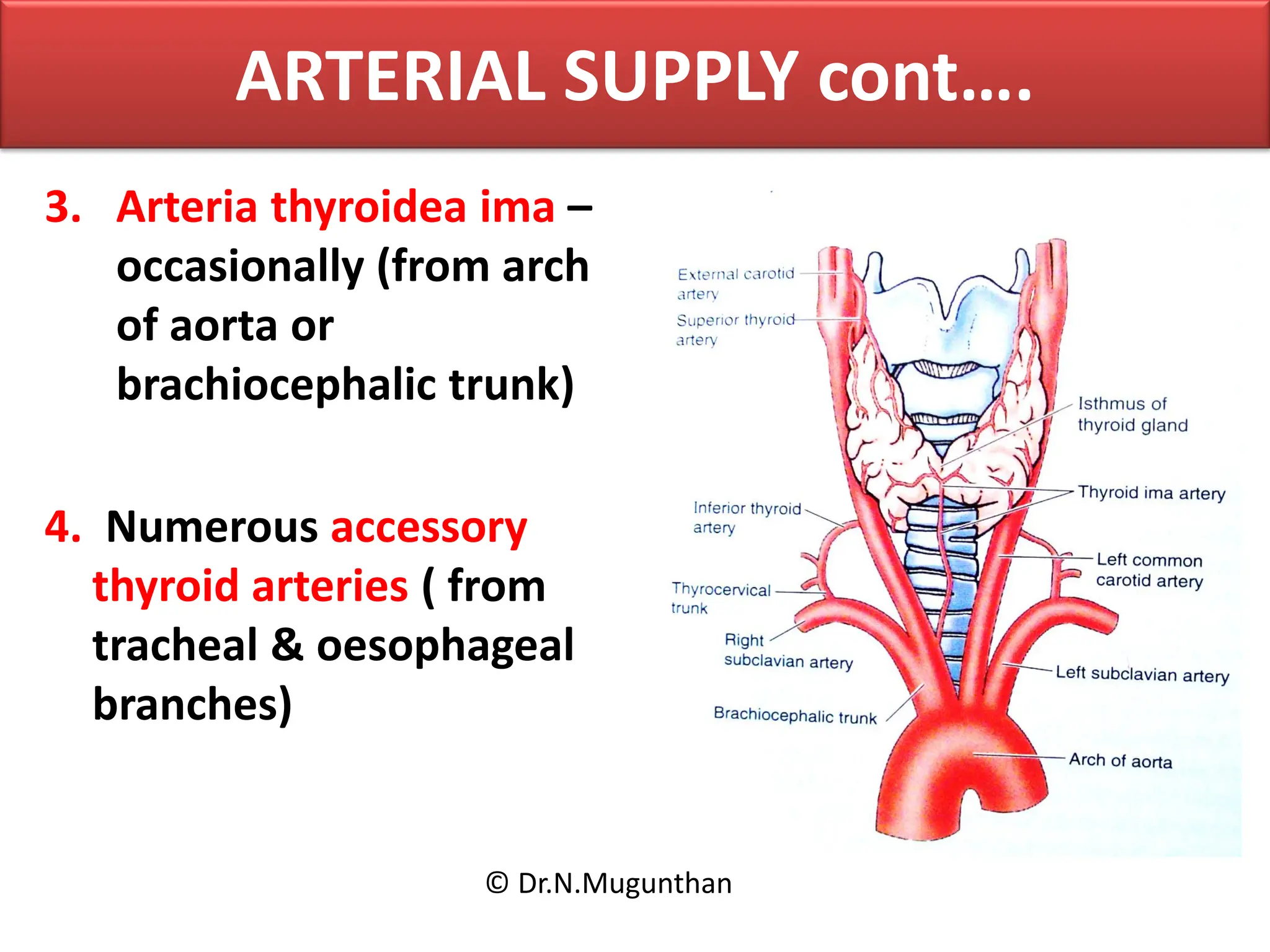
*Thyroid Gland – Anatomy** **Location* * Located in the **anterior neck**, below the **larynx**. * Lies over the **trachea**, from the level of **C5 to T1 vertebrae**. *Structure** Bilobed gland**: Right and left lobes connected by a thin bridge called the **isthmus**. * Sometimes a pyramidal lobe is present (remnant of thyroglossal duct). **Size & Weight** * ~4-6 cm in length. * Weighs about **15–25 grams** in adults. **Capsules** * **True capsule**: Thin fibrous capsule. * **False capsule**: Formed by the pretracheal fascia. *Blood Supply** *Arterial supply**: * **Superior thyroid artery** (from external carotid) * **Inferior thyroid artery** (from thyrocervical trunk) * Occasionally: **Thyroid ima artery** (from brachiocephalic trunk or aorta) * **Venous drainage**: * **Superior**, **middle**, and **inferior thyroid veins** → drain into internal jugular and brachiocephalic veins. **Lymphatic Drainage** * Prelaryngeal, pretracheal, and paratracheal lymph nodes → deep cervical nodes. Nerve Supply** Sympathetic**: Cervical sympathetic ganglia (vasomotor). Parasympathetic**: From the vagus nerve** (via recurrent laryngeal and external laryngeal nerves). * Recurrent laryngeal nerve runs close to the thyroid — important surgically. **Development** * Develops from a **midline endodermal outgrowth** of the **floor of the pharynx** (foramen cecum). * Migrates downward via the **thyroglossal duct** (normally obliterated).