Objectives
1. Understand thecase management process for support
of survivors of GBV
2. Understand how case management services can be
tailored to survivors of different ages and to address
different forms of GBV
3. Understand the responsibilities of a GBV Programme
Manager regarding case management supervision
4. Consider ways to improve service coordination and to
effectively advocate for appropriate response to GBV
3.
What is GBVCase Management?
A structured method for providing help to a survivor. It involves
one organization, usually a psychosocial support or social
services actor, taking responsibility for making sure that
survivors are informed of all the options available to them and
that issues and problems facing a survivor and her/his family are
identified and followed up in a coordinated way, and providing
the survivor with emotional support throughout the process.
4.
Principles of CaseManagement
The survivor is the primary actor
The case management process should empower
the survivor and ensure s/he leads
Plans must reflect a survivor’s wishes and choices
This requires…
Individualized service delivery based on an
Assessment of needs that is used to
Develop a case plan that ensures
Good coordination of service delivery
1. Introduction &Engagement
Have you put the survivor at ease, introduced yourself and the
services you offer?
Greet and comfort the survivor.
Establish rapport and obtain informed consent to proceed with
CM services.
7.
Informed consent
The voluntaryagreement of an individual who has the
legal capacity to give consent.
The survivor must:
• Have the capacity and maturity to know about and
• Understand the services being offered, and
• Be legally able to give her consent
8.
When do weobtain informed
consent?
Before case management services begin= before listening to
a story or gathering information
Throughout the case management process
When making referrals
Before sharing any information on a case or meeting with
other service providers
9.
Confidentiality
“Informed” consent includesinformation on confidentiality
practices
Limitations on confidentiality must be disclosed during Step 1.
Limitations might include:
Mandatory reporting laws
SEA policy
Fear of imminent security risks
Fear of self harm or harm to others
Information sharing among GBV team
10.
2. Assessment
Why isthe individual seeking assistance?
Collect information using a survivor-centred approach
What problems is she facing? How does she see her situation?
What supports does she have? What assistance does she
want?
Listen. And help a survivor identify her problems and needs.
11.
3. Case ActionPlanning
What does the survivor want to happen next?
Develop a case plan based on the assessment
Ask questions about what a survivor wants
This may include personal goals related to return to normal
activities, seeking support from friends, etc.
Provide information on service options
Provide information on processes, and likely outcomes, of different
available services
Obtain consent for referrals and documentation
12.
4. Implementing theplan
How can we help a survivor achieve her goals?
Provide services within scope of work (PSS support)
Refer to other services, as requested
Advocate for services, support
Lead case coordination
13.
5. Case FollowUp
Is the survivor reaching her goals? Is she recovering?
Monitor outcomes with survivor
Identify any barriers to achieving goals
Adapt plan as needed
14.
6. Case Closure
Howdo we know when the work is finished?
Assess with survivor if her goals are met
Assess with survivor if her own (normal or new normal) support
systems are functioning
Ensure any ongoing services are in place
Ensure survivor has means of contact for any future needs
15.
Service Evaluation atCase Closure
What was the quality of the service?
Determine if the client feel satisfied with the service
Reflect on the service provided and any challenges that arose
Assess whether best practices were followed
Benefits of GBVCase Management
Approach
Holistic
Survivor-centered
Restores some measure of
control to the person
affected
Attentive to specific needs,
risks related to GBV
Skills not credentials:
caseworker profile can vary, is
adaptable
18.
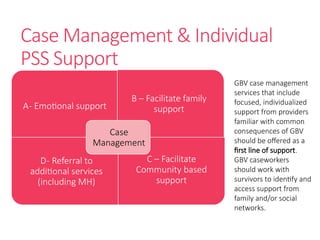
Case Management &Individual
PSS Support
A- Emotional support
B – Facilitate family
support
D- Referral to
additional services
(including MH)
C – Facilitate
Community based
support
Case
Management
GBV case management
services that include
focused, individualized
support from providers
familiar with common
consequences of GBV
should be offered as a
first line of support.
GBV caseworkers
should work with
survivors to identify and
access support from
family and/or social
networks.
Definitions
Intimate Partner Violence(IPV) is an abuse perpetrated by a
current or former partner or spouse. The term domestic
violence is often used interchangeably.
May include:
physical
sexual
psychological violence
as well as the denial of resources, opportunities or services
IPV: Types &Severity
In much of the world, some levels of/ forms of IPV is
considered “normative.” Husbands may be expected to
“discipline” their wives.
IPV survivors who seek GBV case management services
usually describe incidents/ patterns of abuse that would not
be socially sanctioned.
Implications for service provision:
• Community leaders/ family/ others may support interventions
• Security and health risks may be great
Through the casemanagement
process, a survivor of IPV can…
Receive validation and support
Acknowledge patterns of abuse in relationship
Determine limits and explore options
Identify available services
Enlist help of community leaders, others
Link to support networks
Develop safety plan
29.
Safety Plan
Safety planis a specialised type of case plan aimed at reducing
an individual’s risk of future incidents of GBV. An IPV safety plan
is developed with a survivor to help keep her (and her children)
safe from an abusive partner.
30.
Through a SafetyPlan a survivor
of IPV can…
Identify behaviors that precede a partner’s violent episodes
Identify safest spaces in home
Identify a person to tell, way to seek assistance
Identify a safe space to go
31.
Mediation
Mediation is avoluntary process in which two
or more parties involved in a dispute work with
an impartial party, the mediator, to generate
their own solutions in settling their conflict.
Unlike a judge or an arbitrator whose decisions
subject one party to win and the other party to
lose, mediation is about finding a solution that
works for both parties.
32.
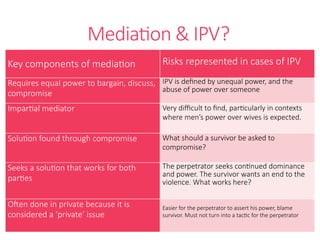
Mediation & IPV?
Keycomponents of mediation Risks represented in cases of IPV
Requires equal power to bargain, discuss,
compromise
IPV is defined by unequal power, and the
abuse of power over someone
Impartial mediator Very difficult to find, particularly in contexts
where men’s power over wives is expected.
Solution found through compromise What should a survivor be asked to
compromise?
Seeks a solution that works for both
parties
The perpetrator seeks continued dominance
and power. The survivor wants an end to the
violence. What works here?
Often done in private because it is
considered a ‘private’ issue
Easier for the perpetrator to assert his power, blame
survivor. Must not turn into a tactic for the perpetrator
33.
Why mediation isnot
recommended for IPV
Violence is ongoing but cyclical. Perpetrators may stop for long
periods of time, where mediators will consider the issue “solved.”
Safety risks heightened during/after process- for survivor and
caseworker
Process often blames the survivor for “causing” episodes. Survivor
might be asked to adapt her behavious as condition to stop violence.
Caseworkers involved risk losing trust of survivors, being perceived
as siding with perpetrators.
Involvement of GBV programmes can validate mediation as an
appropriate intervention for IPV.
34.
What if asurvivor asks for
mediation?
Caseworkers should never mediate themselves.
Caseworkers can act as advocates and support survivors
before, during and after the mediation (depending on survivors’
interests, Caseworker’s comfort, safety, and organizational
policies)
Programmes can seek to influence mediators or mediation
mechanisms, to improve process for survivors
Child Survivors ofSexual Violence
Children experience different consequences to
sexual violence than adults
Children often express suffering differently than
adults
Reactions may be influenced by:
Type of violence
Duration
Relationship to perpetrator
Stage of development
Support received
38.
Definitions
Child sexual abuse(CSA) is any form of sexual activity with
a child by an adult or other child who has power over the
child. Child sexual abuses often, but not always, involves
bodily contact.
Early/forced marriage (EFM) is a form of GBV that is linked
to CSA (marital rape).
Female genital cutting (FGC) is another form of GBV (and
sexual violence) that is mainly perpetrated against children.
39.
Child Sexual Abuse:Key Points
Children face particular risks to GBV, due to their dependence,
limited power, and vulnerability to exploitation, tricks, and
coercion.
Most CSA is perpetrated by people close to children
Globally, girls are up to three times more likely to be victims of
CSA
Incidents involving survivors under 18 constitute roughly half
the caseload of GBV programmes in humanitarian settings
40.
Guiding Principles forWorking with Child
Survivors
Promote the Child’s Best Interest
Ensure the Safety of the Child
Comfort the Child
Ensure Appropriate Confidentiality
Involve the Child in Decision- Making
Treat Every Child Fairly and Equally
Strengthen Children’s Resiliencies
41.
Support for YoungChildren
Is best provided by parents/ caregivers
Requires special training
The child’s wishes should be known
Caseworkers can support parents/caregivers and offer
tips on supporting children
In cases of suspected abuse or neglect, the best interest
of the child must be determined
42.
Support for Adolescents
Thoseworking with adolescents should also be specially
trained.
Adolescents should be able to request and receive
services.
Adolescents should always be asked if they want a
parent/ guardian present during any services.
Adolescents should also be asked before disclosing any
discussions to parents
43.
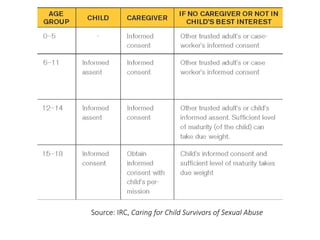
Informed Consent &Informed Assent
A child’s ability to provide consent on the use of the
information and the credibility of the information
will depend on their age, maturity and ability to
express themselves freely.
Informed assent is the expressed willingness to
participate in services. This is sought when a
child is too young to provide informed consent.
If a decision is taken on behalf of the child, the best
interests of the child shall be the overriding guide
and the appropriate procedures should be followed.
The BEST INTERESTSOFTHE
CHILD shall be a primary
consideration in all actions affecting
children.This means that when a course
of action affecting a child is taken, that
course of action should reflect what is
best for that child.
– Convention on the Rights of the Child
46.
Legal Considerations
Understandmandatory reporting requirements
• Does your country have mandatory reporting laws for child abuse
cases?
• What information needs to be shared?
• How is confidentiality protected?
• What are the legal implications of not reporting?
• When is the obligation to report triggered?
Be sure limits to confidentiality are disclosed during the first
step of the case management process.
Definitions
Early marriage isa formal or informal union where one or
both parties is under the age of 18.
Forced marriage occurs at any age when at least one
spouse does not offer full consent.
50.
Early/Forced Marriage: KeyPoints
In developing countries, one out of every three girls is
married before age 18.
Health risks of EFM (and early pregnancy) are severe.
- Increased maternal mortality
- Increased child mortality
- Increased fistula
- Increased HIV and STIs
Relationships initiated through EFM are more likely to involve
IPV.
51.
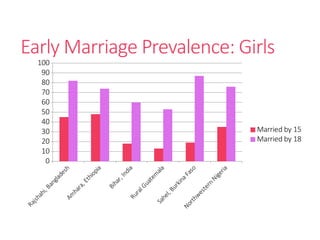
Early Marriage Prevalence:Girls
Rajshahi, Bangladesh
Am
hara, Ethiopia
Bihar, India
Rural Guatem
ala
Sahel, Burkina Faso
Northwestern
Nigeria
0
10
20
30
40
50
60
70
80
90
100
Married by 15
Married by 18
52.
Challenges: Case Management& EFM
The practice is socially promoted and sometimes legally
sanctioned
Limited services, options
Limited guidance for Caseworkers
53.
Case Management: Imminentrisk of EFM
Apply appropriate informed consent procedures
Assess
• Feelings about marriage
• Knowledge of possible consequences
• Family situation
Engage supportive caregiver, if possible
• Approach in non-judgmental manner
• Provide information
Link to other services, where relevant
54.
Case Management: EFMProceeding
Maintain relationship with survivor
Engage survivor to assess potential risks
Develop safety plan
Share SRH information, referrals
Help to identify supportive person
Help to develop coping strategies
Help to maintain routines, connections– school, family,
etc.
55.
Case Management: EFMHas Occurred
Assess situation and specific risks
Develop safety plan
Share information on consequences of early marriage,
including SRH information and referrals
Help survivor identify supportive person
Help survivor develop coping strategies
Link survivor to services, including group PSS activities
56.
EFM: Additional programmeoptions
Target likely survivors of EFM through group activities
Address risks of EFM through community prevention work
Engage community leaders as allies
Partner with SRH (ASRHR) programmes for prevention &
response
Partner with legal/advocacy actors to address
laws/procedures
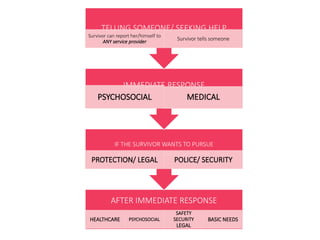
AFTER IMMEDIATE RESPONSE
HEALTHCAREPSYCHOSOCIAL
SAFETY
SECURITY
LEGAL
BASIC NEEDS
IF THE SURVIVOR WANTS TO PURSUE
Accompaniment should be offered
PROTECTION/ LEGAL POLICE/ SECURITY
IMMEDIATE RESPONSE
PSYCHOSOCIAL MEDICAL
TELLING SOMEONE/ SEEKING HELP
Survivor can report her/himself to
ANY service provider
Survivor tells someone
59.
Establishing Referral Systems
Map and collect information on services
Identify lead service providers per sector
Establish focal points
Establish agreements, SOPs
Train and inform
Collect feedback, review, and update systems
60.
Service Referrals
Caseworkersmust understand the services available from
other providers
Programmes can ask other providers (focal points) to share
brief points on services to relay to survivors
Caseworkers must offer all options to survivors and help
them weigh benefits and drawbacks, then respect their
choices
Caseworkers can coordinate with chosen service providers
to support a client’s action plan, also according to a survivor’s
wishes
61.
Spaces for Coordination
Protection Cluster/WG
GBV Sub-Cluster/WG
Referral pathway working groups (focal points)
Case management meetings (ad hoc)
Bilateral meetings between service providers
62.
The GOAL ofGBV Coordination
To provide accessible, prompt, confidential and
appropriate services to survivors according to a
basic set of guiding principles and put in place
mechanisms to prevent GBV.
– GBV AoR Coordination Handbook
To whom areGBV Programme
Managers accountable?
To whom are GBV Caseworkers
accountable?
68.
The core ofGBV case management
supervision is ensuring the physical and
emotional safety of survivors, as well as
caseworkers.
69.
GBV Case WorkSupervision
Requires:
Building case management systems that are safe,
accessible and adapted to the environment
Building and supporting case management teams
with appropriate profile, skills and attitudes
70.
Case Management: Strong
Systems
Entry points
Service points
Documentation procedures
Referral and information-sharing procedures
Monitoring, quality control
Plans for close-out/handover/evacuation
71.
Case Management: StrongTeams
Recruitment
Initial Training
Continued learning and coaching
Dedicated supervision
Monitoring, quality control
Team support and self-care
Objectives
1. Understand thecase management process for support
of survivors of GBV
2. Understand how case management services can be
tailored to survivors of different ages and to address
different forms of GBV
3. Understand the responsibilities of a GBV Programme
Manager regarding case management supervision
4. Consider ways to improve service coordination and to
effectively advocate for appropriate response to GBV
Editor's Notes
#1 Q: How many of you work in an environment where someone is offering case management services?
Q: How many of you work with programmes offering case management services?
Q: Of those offering case management services, how do you define case management?
#3 UNICEF (2014). Communities Care Programme: Transforming Lives and Preventing Violence. UNICEF, New York. This definition is applied in the Interagency GBV Case Management Guidelines (2017).
#7 Informed consent is defined as the voluntary agreement of an individual who has the legal capacity to give consent. The survivor must have the capacity and maturity to know about and understand the services being offered and must legally able to give her consent.
When I say ’legal capacity to give consent’, what does that mean to you?
*Prompting questions, if needed:
How old must someone be to give their consent?
What about individuals with disabilities? Can they give their consent?
What happens if someone is putting pressure on a survivor – is the consent valid?
#8 Refer participants to pate 54 in the Case Management Guidelines. It is imperative that we obtain informed consent BEFORE case management services begin, which includes before listening to a survivor’s story or gathering any information. We should obtain informed consent as a part of regular, ongoing case management and whenever we make a referral to services. In simple terms, informed consent is an ongoing process of making sure the survivor is fully in agreement with, and in control of, the full process of case management – and that we are not making any assumptions about his/her agreement without asking explicitly.
Informed consent is a way of establishing a survivor’s control over the case management process. Experiencing violence is disempowering for a survivor, and our role is to give him/her back his/her power in every way that we can.
When we skip or complete informed consent improperly, it undermines the guiding principles of a survivor-centered approach and jeopardizes our relationship with the survivor. By obtaining informed consent, we demonstrate our respect for the survivor, show her we intend to be collaborative and empowering and show her that we understand the need to be accountable to her in the case management process.
#9 Discuss the principle of confidentiality. Confidentiality is often discussed as “keeping secrets,” but of course survivors can share information with whomever they choose, and those working with survivors sometimes need to share information. It is better to always remember that survivors own information, and survivors’ information should always be treated with the upmost care and respect.
Refer participants to page 52 in the Case Management Guidelines. Ask participants to read through the sample script and discuss.
Refer participants to page 55 in the Case Management Guidelines– checklist for completing Step 1.
#10 Refer participants to page 67 in the Case Management Guidelines, from “Identify protective factors and strengths.” Discuss the often-neglected need to conduct an assessment related to psychosocial support needs.
Refer participants to page 75 in the Case Management Guidelines. Review the checklist for Step 2.
#11 Refer participants to page 79 in the Case Management Guidelines: Discuss and set personal goals with the survivor.
Case planning should not focus exclusively on service needs and referrals. Especially where options are limited for survivors, helping a survivor to set personal goals is an important service that can have a great impact on wellbeing.
*Remember that survivors require good information to offer consent. Caseworkers should have good information on what survivors can expect from services in order to share this with survivors. Programmes must coordinate well with other service providers to have this information. Suggestions: Conduct walk-throughs at clinics to understand what a survivor might experience at each step; Link to legal counsellors who can provide more information on legal service options for survivors considering pursuing justice.
#12 Where programmes face obligations of mandatory reporting, reporting occurs during this step.
#13 Expectations for follow up (including who, when and how often) should be established during case planning.
Caseworkers should check in with survivors on the six points reviewed in the psychosocial session– safety, services, social, family, health, feelings. Follow up is not only related to services received; follow up allows caseworkers to monitor survivors’ progress along their own plans for recovery and improved wellbeing. Over time, survivors who are not improving or show signs of deterioration may require more specialised support.
#14 Cases are not “solved” when they are closed. Caseworkers should re-frame this common thinking, from “solved” to improved safety and wellbeing, as well as satisfaction with services received, and confidence in where to seek additional help if needed.
#15 What tools might a programme use?
Client satisfaction surveys
Outcome assessments
#18 Focused, GBV case management services are recommended for holistic support of survivors. Trained staff familiar with forms of violence and their consequences are best-placed to provide appropriate service referrals and to support survivors through a process of recovery.
GBV case management is a psychosocial support service and also a process by which survivors can link to additional services, including additional psychosocial support. GBV caseworkers should be trained to provide basic emotional support to a survivor throughout the case management process. The social, emotional and psychological consequences of GBV are often the most significant consequences a survivor faces, and many survivors will report problems such as sleeplessness, anxiety and fear long after their medical and basic security needs have been addressed.
#19 Participants pair up and practice steps of case management with partner. First case study: Fatima.
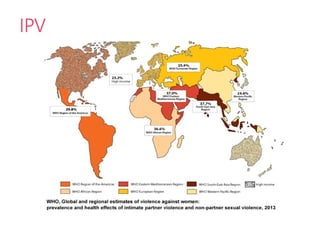
#23 Intimate partner violence is one of the most common violence women and subjected to.
#24 Death and injury - The study found that globally, 38% of all women who were murdered were murdered by their intimate partners, and 42% of women who have experienced physical or sexual violence at the hands of a partner had experienced injuries as a result.
Depression - Partner violence is a major contributor to women’s mental health problems, with women who have experienced partner violence being almost twice as likely to experience depression compared to women who have not experienced any violence.
Alcohol use problems – Women experiencing intimate partner violence are almost twice as likely as other women to have alcohol-use problems.
Sexually transmitted infections – Women who experience physical and/or sexual partner violence are 1.5 times more likely to acquire syphilis infection, chlamydia, or gonorrhoea. In some regions (including sub-Saharan Africa), they are 1.5 times more likely to acquire HIV.
Unwanted pregnancy and abortion – Both partner violence and non-partner sexual violence are associated with unwanted pregnancy; the report found that women experiencing physical and/or sexual partner violence are twice as likely to have an abortion than women who do not experience this violence.
Low birth-weight babies – Women who experience partner violence have a 16% greater chance of having a low birth-weight baby; Studies have found children born to women experiencing IPV are 40% more likely to suffer from stunting.
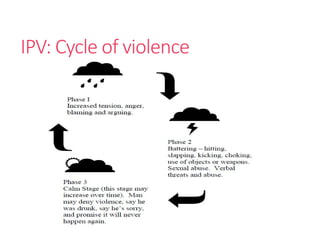
#25 The cycle of violence theory was developed at the very end of the 70s in the US.
It explains how and why the behavior of a person who commits domestic and family violence may change so dramatically over time.
The cycle of violence theory also provides an understanding to why the person affected by domestic and family violence continues to face a violent situation.
The physical violence often happens in cycles (i.e. crisis, a period of calm, and then the violence flares up again).
This pattern is circular (i.e. keeps repeating itself). The cycle goes through a number of stages, that might be more or less depending on case.
The build-up phase (Phase 1)
This phase may begin with normal relations between the people in the relationship, but involves escalating tension marked by increased verbal,
emotional or financial abuse. In non-violent relationships these issues can normally be resolved between the people in the relationship.
Explosion (phase 2)
The explosion stage marks the peak of violence in the relationship. It is the height of abuse by the person who uses violence to control and have power over others.
In the phase 3, perpetrator goes from remorse for what he did, to apologizing and promising it will never happen again to what is sometimes called the “honeymoon phase”
In the more violent phase survivor might want to escape fro the relationship and the abuses, but when the situation gets calmer (phase 3), she might change her mind, thinking (hoping) that it was just a sporadic episode that he was sorry and promised that will never happen again. In phase 3 both people in the relationship may be in denial as to how bad the abuse and violence was. Both may wish to ignore the possibility that the violence could occur again.
Until the tension increases again.
#26 SBC interventions focused on preventing and reducing IPV have proven to be very effective. However, GBV programme managers should understand that different patterns of abuse exist within all communities. In all societies, even where IPV is not considered “normative,” women experience violence. Partners who demonstrate patterns of abuse outside social norms– and those who demonstrate patterns of severe and escalating abuse– are unlikely to easily shift these behaviors.
IPV should not be tolerated in any form, but where some levels of IPV are considered normal/ expected within the social norms framework, women are unlikely to seek help in response to more typical forms of abuse. Survivors reporting to GBV case management services often explain that the abuse is severe, unprompted, escalating, or not proportionate to perceived infractions.
Even where some levels of IPV are expected, community leaders and structures will have remedies for addressing abuse that is considered disproportionate or too severe. For this reason, leaders will often approve of GBV programs supporting survivors of some forms of IPV, and they may be willing to provide support themselves (though their acceptance of some levels of violence will remain problematic). Survivors seeking GBV case management services, though, are often living with significant and ongoing risks. No one involved with GBV case management should expect that the partners of clients will easily change their behaviors after interventions by community leaders/ others.
#27 Discuss the interest in finding “solutions.”
The job of a caseworker isn’t to solve a survivor’s problems. This framework needs to shift, to thinking about improved safety and improved wellbeing. And helping survivors to think though what they would do if they had to leave temporarily or permanently
#29 Safety planning: how does she address her safety while in the same house as her husband, how does she leave the harm without further endangering her lives or the lives of her kids
Safety of children: are the children at risk of being harmed?
Legal issues
Police reporting
Power and Control and Cycle of Violence: she may come to you during the increase of the fighting, but when things return to calm, she may desert the counseling
Future goals (remain in violent situation?)
Important to remain contact with survivors.
#31 Mediation may be requested by survivors, with few options available in many contexts (allows easy access to some sort of justice for those who cannot access the formal justice system, ppl trust more community leaders than police, could be the only option where there are no services to help survivor etc)
That’s why it is important for us, as GBV staff be aware of mediation processes and the risks involved for the survivor in IPV cases. Remember we work and support the survivor; we are not impartial.
#32 Unequal power imbalance. Mediation assumes that both parties are equal, yet an abuser holds tremendous power over a victim. The imbalance of power between the parties cannot be remedied despite the skills of the mediator, even when a victim advocate or attorney is present. During mediation, the abuser can easily control the victim through the use of signals known only to the couple. Additionally, if there is a long history of domestic violence, the victim is often afraid and reluctant to voice her concerns. Because survivors often depend on the perpetrator for income, for community acceptance, have little rights in terms of inheritance or child support/custody, survivors start off with a limited base for negotiation, strengthening further the power imbalances that exist between the survivor and the perpetrator.
Impartial mediation: It will be very difficult in the contexts in which we work to find an ‘impartial party’ to run mediation given the cultural and social prejudices against survivors and in favor of perpetrators. If the mediator is not impartial, then the survivor’s rights will not be respected.
Solution=compromise: the purpose of mediation is finding a solution that works for both people - yet the solution for the perpetrator is maintaining his domination of the survivor, whereas the survivor wants the violence to stop. No compromise can be made on violence- the only solution that is acceptable is a stop to the violence, yet perpetrators are the only ones who can stop it.
Mediation focuses on future behavior, and many mediators do not allow the victim to address past issues of violence. This furthers the victim's sense of personal responsibility for the abuse, and undermines the accountability of the abuser.
#33 Mediating on cycle: DV is also characterized by a cycle of violence that is ongoing and typically combines several different types of abuse (physical and emotional) to achieve control over survivors. It is rarely a one-time event, but a continuum of incidents tied together. This cycle and ongoing violence make it very difficult to mediate on because although survivors can point to individual incidents, that cannot truly represent the totality of the violence they face.
Security concerns: unlikely that the mediation will break the cycle of violence. On the opposite, the mediation might accelerate the cycle and during the increasing tension phase, the perpetrator might easily blame the survivor for shared publicly their private issues through the mediation.
Survivor blaming: There is a high risk of survivor blaming within the mediation process. The perpetrator, who is used to blaming the survivor, will have a platform to articulate his position, and given the cultural and social norms in place, and the fact the survivor may feel intimidated or scared to answer back, he may sound convincing. The survivor may be asked to change her behavior or adapt as condition for violence reduction. This is unacceptable - only the perpetrator can stop the violence. We know that a survivor’s behavior is not at the root of the violence nor is there anything a survivor can do to stop the violence.
#34 In context where mediation is widely used and requested by survivors, we can engage active community leaders or other respected persons within the community, working with them (providing trainings, awareness, involving them in awareness activities etc) and involve them in conducting mediation in IPV cases. We should not be doing mediation directly.
A caseworker can: Discuss with survivor how mediation works, risks, rights and other options available
Work with mediator in advance to ensure survivor’s needs and wishes are considered, including pre-mediation meetings
Be aware of local laws and procedures about mediation
Work with mediators to make sure they do understand the complexity of IPV
Be present to the mediation and advocate for the survivors
Work with community leaders to make sure they also understand the complexity of IPV
* IMC’s Community Leaders Toolkit (2021) includes guidance for engaging with community leaders around mediation and justice proceedings in the Response chapter.
Refer to IMC’s Community Leaders Toolkit for guidance on supporting survivors involved with mediation and advocacy with community leaders.
#35 Participants work in the same pairs, switching roles. Case study is focused on IPV.
#37 Ask participants to offer examples of possible consequences of sexual violence for children.
Health consequences.
Physical consequences can be more complicated
Physical examination is conducted differently for young children. Dosages for post-rape drugs differ for young children.
Social consequences.
As with adults, these will differ in different environments.
How might sexual abuse affect a child’s schooling?
How might sexual violence impact a child’s marriageability?
* Remember that child sex abuse affects both boys and girls. Participants may want to discuss whether CSA is technically a form of GBV– this issue is not, of course, relevant to how we should respond to individual cases.
Immediate reactions of children, as well as possible long-term consequences, may depend on factors listed.
The significance of a perpetrator’s identity is related to his/her closeness to a child
A child’s developmental stage will influence his/her ability to understand what happened.
#41 GBV support workers responding to cases of child sexual abuse require specialized training and consistent supervision and support.
Even where child specialists are available, it is better, when possible, for trusted guardians to provide primary emotional support.
GBV support workers can talk with parents about expecting some abnormal behaviors (some examples can be provided, without leading to specific expectations).
Parents should assure the child the violence was not his/her fault and that he/she is still loved by the family. The child should feel free, but not forced, to talk about the experience. It is important for parents/guardians to continue to treat children normally (meals with the family, normal routines, etc), while allowing time for the child to fully participate in all normal activities. Extra attentiveness and affection are important supports for children.
In cases where parents/caregivers are responsible or negligent, the best interest of the child must be determined. This should ideally be determined through a process, involving child specialists. Where no specialist agency or individual is present, meetings should be held between those involved with the case. Involvement from appropriate ministries/ other concerned parties should be considered.
#42 This slide uses the term “adolescents” for older children, from the approximate ages of 12/13 to 18.
If a parent first approaches a Volunteer about an adolescent who has been raped:
Ask the parent’s permission to talk alone with the adolescent
Then ask the adolescent if she wants her parent with her when you talk
Proceed to discuss service options with the adolescent
Ask the adolescent’s permission to talk to her parent about what you discussed
If consent is granted by both parties, continue to follow up with both parent and adolescent.
If an adolescent first approaches a Volunteer and discloses rape:
Stabilize situation/ provide calm, quiet place as normal
Ask who the adolescent wants with her during services
Ask if you can let one of her parents know what has happened, and talk to them about this in a good way
If she does not consent, proceed to offer medical treatment as normal
#47 Consider a new exercise for this round of practice– small group or large group discussion is often preferred. Case study is focused on a child survivor.
#49 As children under 18 cannot give consent to marriage all early marriage should be considered forced marriage.
#50 A multi-country study found that maternal mortality doubled for mothers aged 15-19, compared to mothers aged 20-34. For mothers under 15, the rate doubled again.
#51 Source of graph: Population Council 2011
Early marriage prevalence varies considerably by country.
Globally, 21% (more than 1/5) of girls are married before they reach 18. (UNICEF)
In least developed countries, 36% of girls are married before age 18, and 10% of girls are married before age 15. (UNFPA)
Globally, 4.5% of boys are married. (UNICEF)
#58 Refer to SOP Guides, page22 (IASC 2008). Establishing Gender‐Based Violence Standard Operating Procedures (SOPs) for multi-sectoral and inter‐organisations prevention and response to gender‐based violence in humanitarian settings
Discuss briefly how and why SOP Guide was established.
GBV programs can and should support community work vis-à-vis referral pathways. If these are not yet established in and with communities, this can be an important contribution of GBV programmes. The process of developing a referral pathway with community and partner input is time consuming- don’t underestimate the investment of time.
#61 What information should be shared during coordination meetings?
When should a case management meeting be established?
Who should attend?
#62 Ask: What is the GOAL of GBV Coordination.
While this is the goal, the challenge is accomplishing this goal through enabling humanitarian actors within and between sectors to do this
We must always remember why we care about GBV coordination—why this is a good thing. Too often we get bogged down by meetings that seem to go nowhere and forget that the whole process started because we wanted to make people’s lives better. In considering our own participation in a GBV coordination structure, it is important to remember that all of our actions in this context are about creating a safer and more supportive environment for women, girls, men and boys to survive and thrive.
#63 How does first response work when many are already involved, already present?
Often, the work of a GBV PM is to help turn the volume down. This may include:
Stabilizing and calming an environment
Ensuring a survivor is not pulled to services, but provided a quiet and safe space to rest and make decisions
Ensuring a survivor is only in the company of her choice
Arranging services
Advocating restraint to actors a survivor has not chosen to meet.
(as discussed during PSS individual support session)
#64 How can a GBV Program Manager advocate for survivor-centred response when many actors and agencies are expressing interest?
Discuss different actors’ presence and their place in first response.
Refer again to SOP Guide. Established SOPs are useful for clarifying roles of different actors.
#65 Participants work in the same pairs, switching roles. Case study is focused on service coordination.
#67 Open discussion for different layers of accountability– supervisors, HQ, donors, cluster leads, host government, population, staff, survivors. How should we think about our multiple– and at times competing– sources of accountability?
For GBV programmes that offer case management services– to whom are Caseworkers accountable? Do they face similar pressures related to multiple responsibilities?
#69 This will not provide instruction on all a Manager requires to provide appropriate supervision for CM services, but is rather intended to provide an overview of what the work involves. GBV CM Toolkit offers particular guidance on case management supervision, including monitoring tools.
Please also refer to GBV Core Competencies Framework– further discussed during the HR module.



























![A.L.I.V.E.[1]](https://cdn.slidesharecdn.com/ss_thumbnails/alive1-124242587805-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)































