Learning Objectives
1.Define tuberculosis and describe its causative agent
and transmission.
2. Describe the global and national epidemiology of TB.
3. Identify key risk factors and vulnerable populations.
4. Explain methods of diagnosis, including the Mantoux
test.
5. Discuss TB control strategies: DOTS, BCG,
chemoprophylaxis.
6. Describe WHO treatment categories and the National
TB Control Program (NTP).
4.
Introduction to
Tuberculosis
• Chronicinfectious disease caused by Mycobacterium tuberculosis
• Primarily affects lungs but may involve other organs
• Pulmonary TB is the most common and infectious form
5.
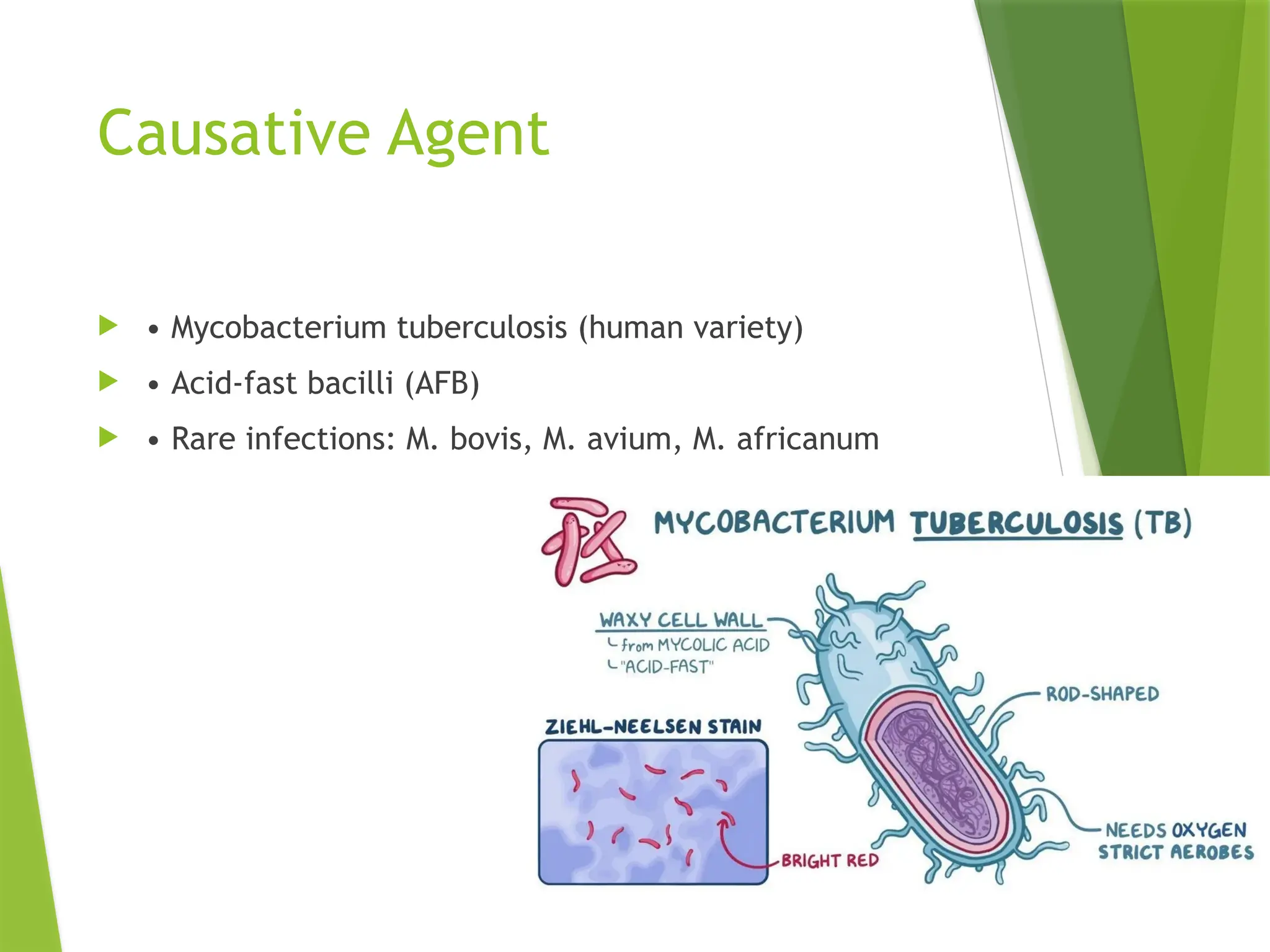
Causative Agent
•Mycobacterium tuberculosis (human variety)
• Acid-fast bacilli (AFB)
• Rare infections: M. bovis, M. avium, M. africanum
6.
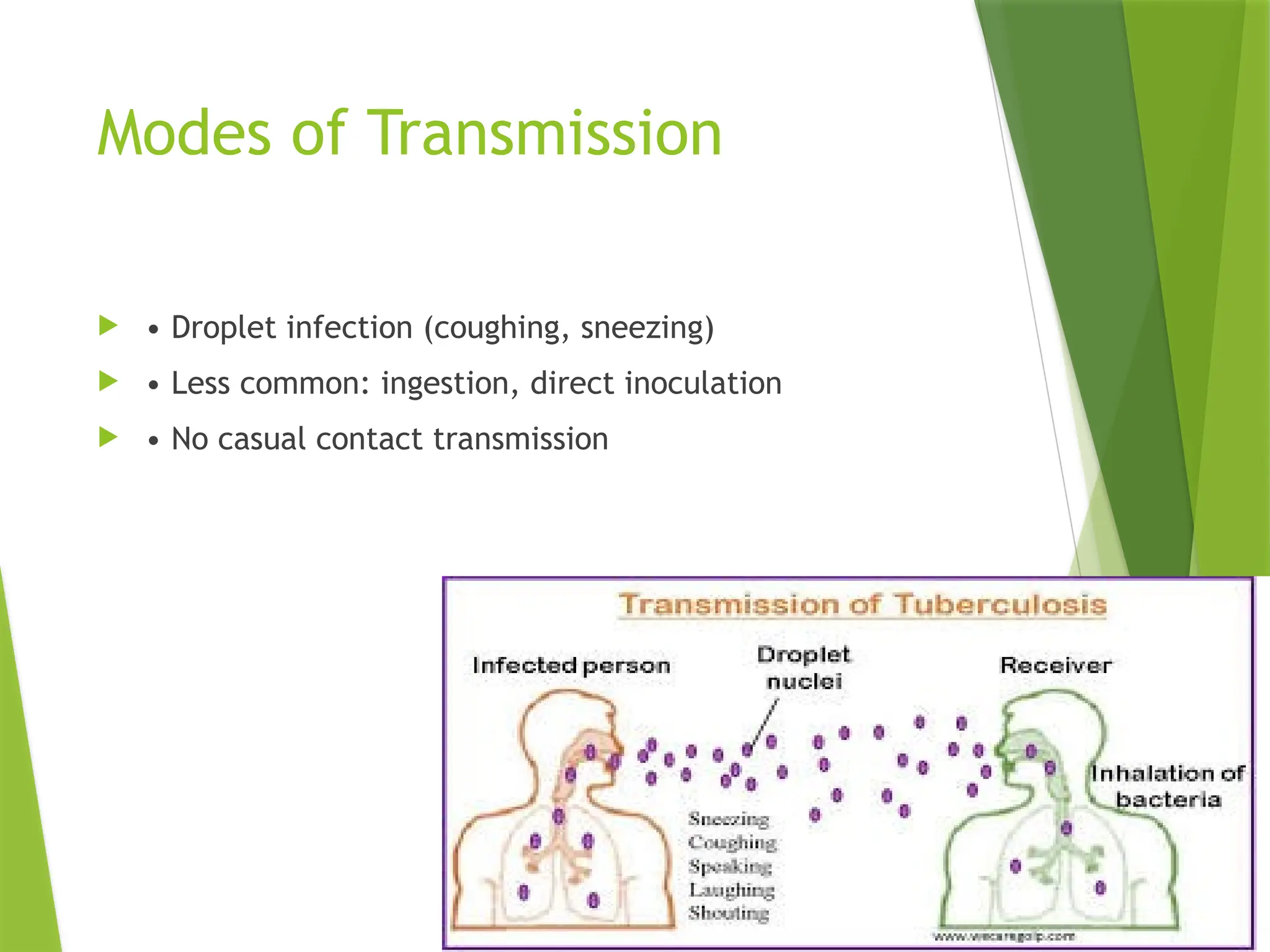
Modes of Transmission
• Droplet infection (coughing, sneezing)
• Less common: ingestion, direct inoculation
• No casual contact transmission
7.
Global Epidemiology
•WHO: 10.6 million cases annually
• 1/3rd of population has latent TB
• High burden: South-East Asia, Africa, Western Pacific
8.
TB in Pakistan
• 5th highest TB burden globally
• Incidence: 263/100,000
• Most common in 15–45 age group
• Contributing factors: poverty, overcrowding
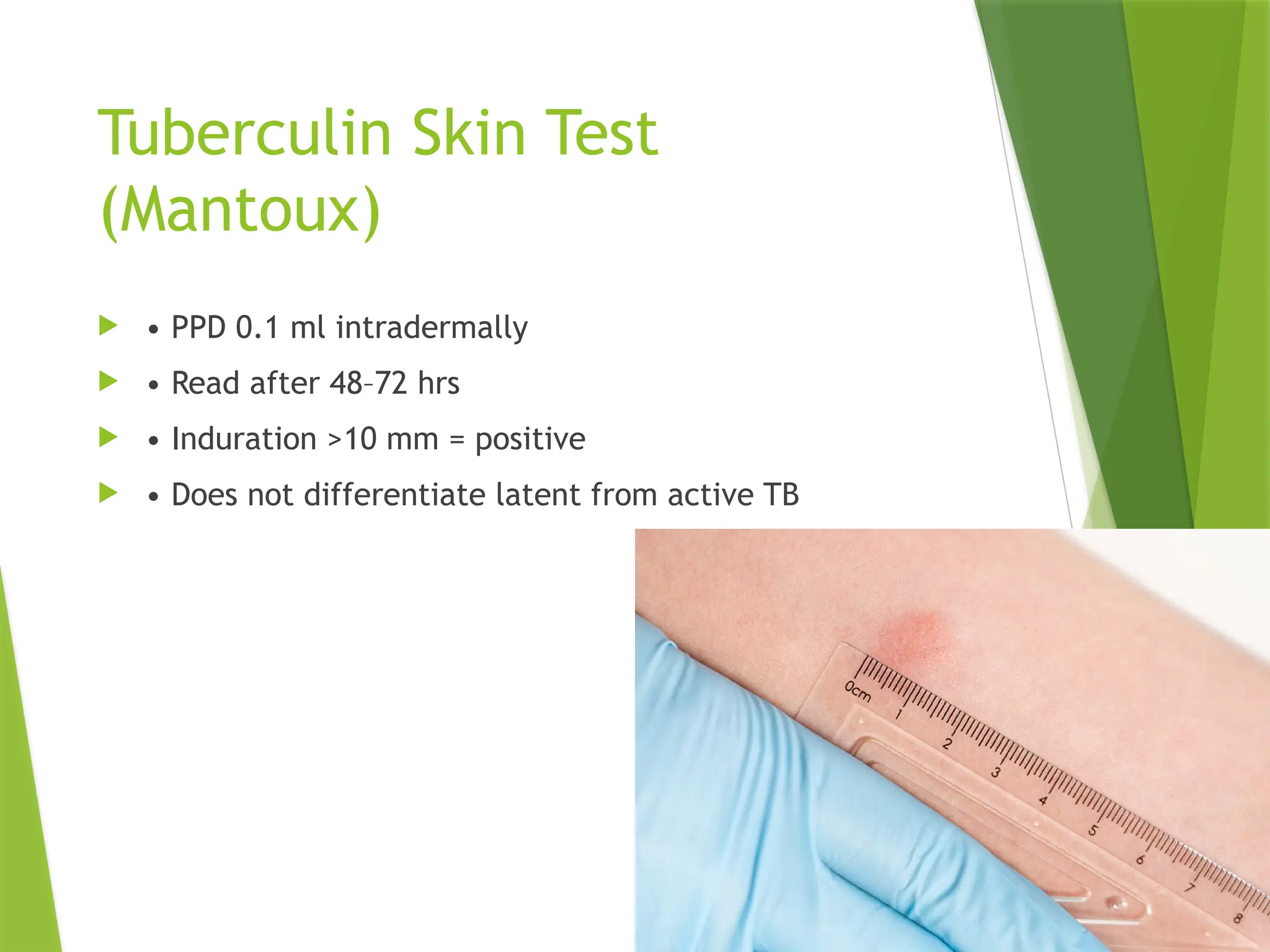
Tuberculin Skin Test
(Mantoux)
• PPD 0.1 ml intradermally
• Read after 48–72 hrs
• Induration >10 mm = positive
• Does not differentiate latent from active TB
12.
TB Case Definitions(WHO)
• New case: no or <1 month of treatment
• Relapse: previously cured, now positive
• Smear-positive: AFB visible
• Smear-negative: clinical + radiological signs
13.
TB Control Strategies
• Early detection and treatment
• DOTS strategy
• BCG at birth
• Health education
14.
DOTS Strategy
1.Political commitment
2. Case detection
3. Supervised treatment
4. Drug supply
5. Monitoring
BCG Vaccination
•Live attenuated M. bovis
• Given at birth (0.05 ml), >4 wks (0.1 ml)
• Prevents severe TB in children
18.
Chemoprophylaxis
• INH6–9 months for children <5, HIV+ with latent TB
• BCG is preferred for general population
19.
Summary
• TBis a major public health issue
• DOTS and BCG are cornerstones
• Community awareness is key
20.
MCQs for Self-Assessment
1. Most common TB transmission mode?
2. Specific test for active TB?
3. DOTS full form?
4. NTP diagnostic approach?
5. BCG efficacy?

![Tuberculosis
Dr. Mahnoor | Department of Community Medicine
Date: [Insert Date]](https://image.slidesharecdn.com/tblecturewithnotes-250806193529-41ee802d/75/TB_Prevention-of-Tuberculosis-and-BCG-vaccine-2-2048.jpg)