Russian Escort Service in Delhi 11k Hotel Foreigner Russian Call Girls in Delhi
sympatheticoverdriveinhypertension ppt.pptx
1. contents
1. Egan BM, Basile J, Chilton RJ et al. Cardioprotection: the role of β-blocker therapy. J Clin Hypertens. 2005;7(7):409–16.
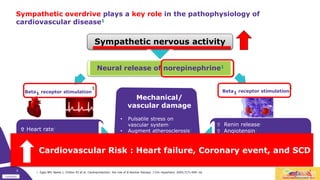
Sympathetic nervous activity
Heart rate1
Heart rate variability1
Contractility1
Renin release1
Angiotensin1
Blood pressure1
Left ventricular hypertrophy1
Heart failure1
Beta1 receptor stimulation
1
Beta1 receptor stimulation
1
Sympathetic overdrive plays a key role in the pathophysiology of
cardiovascular disease1
Mechanical/
vascular damage
• Pulsatile stress on
vascular system1
• Augment atherosclerosis1
• Plaque rupture1
• Risk of cardiac ischemia1
Neural release of norepinephrine1
Graph according to reference 1
0
Cardiovascular Risk : Heart failure, Coronary event, and SCD
2. contents
1. Cruickshank JM. The Modern Role of Beta-blockers in Cardiovascular Medicine. Shelton, CT: People's Medical Publishing House-USA;2011; Fig. 3-8
2. Cruickshank JM. Beta-blockers and diabetes: the bad guys come good. Cardiovasc Drugs Ther. 2002;16(5):457–70.
3. Poitras VJ, Pyke KE. The impact of acute stress on vascular endothelial function: Evidence, mechanisms and importance. Int J Psychophysiol. 2013;88(2):124–35
4. Cruickshank JM. The Modern Role of Beta-blockers in Cardiovascular Medicine. Shelton, CT: People's Medical Publishing House-USA;2011
5. Klein LW, Pichard AD, Holt J et al. Effects of chronic tobacco smoking on the coronary circulation. J Am Coll Cardiol. 1983;1(2 Pt 2):421–26
6. Huggett RJ, Scott EM, Gilbey SG et al. Circulation. 2003;108:3097–101.
1
What can trigger for sympathetic overdrive?
Diabetes1,2
Mental stress3
Obesity4 insulin resistance, endothelial dysfunction and increased NE
Smoking5 increased 2 to 3 fold increased NE
Hypertension6
3. contents
Underlying causes of hypertension differ between
The Young VS Old – Framingham Heart Study1
Blood pressure (BP); Diastolic BP (DBP); Systolic BP (SBP); Diastolic hypertension (DH); Systolic/diastolic hypertension (SDH); Isolated systolic hypertension (ISH); Pulse pressure (P-P)
1. Franklin SS, Pio JR, Wong ND et al. Predictors of new-onset diastolic and systolic hypertension. Circulation. 2005;111:1121–7.
2. Cruickshank JM. Are we misunderstanding beta-blockers? Int J Cardiol. 2007;120:10–27.
3. Grassi G. Assessment of sympathetic cardiovascular drive in human hypertension: achievements and perspectives. Hypertension. 2009;54(4):690–97.
Sympathetic overdrive is the main cause of hypertension in young or middle-aged patients2,3
Predictors of diastolic hypertension
(± systolic hypertension)
= DBP ≥90 mmHg ( SBP ≥140 mmHg)
1 Young age
2 Male sex
3 High BMI at baseline
4 Increasing BMI during follow-up
Main mechanism of DH and SDH
is raised peripheral resistance
Predictors of isolated systolic hypertension
= SBP ≥140 mmHg + DBP <90 mmHg (wide P-P)
1 Older age
2 Female sex
3
Increasing BMI during follow-up
(but weaker than in young)
4
ISH arises more commonly from normal
and high normal BP
5
Only 18% with new-onset ISH
had a previous DBP ≥ 95 mmHg
Main mechanism of ISH is
increased arterial stiffness = aging of arteries
2
4. contents
Increased heart rate is a long-term predictor of cardiovascular events in
patients with hypertension1
Increased cardiovascular mortality rate, suddden cardiac death
53 %
difference in
incidence of
endpoints1
The incidence of primary
endpoints in the highest in-
trial HR group compared to
the pooled 4 lower quintiles
was 53% greater in patients
with well-controlled blood
pressure (p<0.001)1
1. Julius S, Palatini P, Kjeldsen SE et al. Usefulness of heart rate to predict future cardiac events in treated patients with high-risk systemic hypertension.
Am J Cardiol. 2012;109:685–92.
14 %
12 %
10 %
8 %
6 %
4 %
2 %
0 %
250 750 1250 1500
1000
500
Days since year 1 and patients at risk
Cumulative
primary
event
rate
High HR, BP uncontrolled
High HR, BP controlled
Low HR, BP uncontrolled
Low HR, BP controlled
Graph adapted from reference 1
3
5. contents
Pharmacotherapy options for elevated heart rate:1-5
Beta blockers
(without ISA)3
HR control via
actions on
Sympathetic
overdrive3
If channel inhibitor
(ivabradine)
Specific action on
the If channel that
controls in sinoatrial
node
Non-
dihydropyridine CCBs
(verapamil, diltiazem)1
Action is not related to
Sympathetic overdrive
Elevated heart rate
Calcium channel blockers(CCBs) Sympathetic overdrive(SO) Intrinsic sympathomimetic activity(ISA) Coronary heart disease(CHD)
1. Palatini P, Benetos A, Julius S. Impact of increased heart rate on clinical outcomes in hypertension: implications for antihypertensive drug therapy. Drugs. 2006;66(2):133–44.
2. Gupta D. A review on calcium channel & its blockers. Int J Pharm Pharm Sci. 2012;4:3842.
3. Egan BM, Basile J, Chilton RJ et al. Cardioprotection: the role of beta-blocker therapy. J Clin Hypertens. 2005;7(7):409–16.
4. DiFrancesco D, Camm JA. Heart rate lowering by specific and selective I(f) current inhibition with ivabradine. Drugs. 2004;64:1757–65.
5. Sulfi S, Timmis AD. Ivabradine: the first selective sinus node I(f) channel inhibitor in the treatment of stable angina. Int J Clin Pract. 2006;60:222–28.
6. Procoralan (ivabradine) Summary of Product Characteristics, revision dated 7 June 2016.
7. Montalescot G, Sechtem U, Achenbach S et al. 2013 ESC guidelines on the management of stable coronary artery disease. Eur Heart J. 2013;34:2949-3003.
4,5
4
6. contents
Modulation of sympathetic activation is an important goal of
antihypertensive treatment: effect of different drug classes1
Drug class Effects on peripheral SNS Effects on cardiac SNS
Central sympatholytics Marked reduction Reduction
Alpha-blockers Marked reduction No change
Thiazide diuretics Marked increase No change
Anti-aldosterone agents Reduction No change
Beta-blockers Reduction Marked reduction
Short-acting CA Marked increase Marked increase
Long-acting CA Reduction or no change No change or increase
ACE inhibitors Reduction or no change No change
Angiotensin II receptor blockers* Reduction or no change No change
*Although laboratory studies suggest that angiotensin II receptor blockers may inhibit the SNS, they have been shown to increase sympathetic activity in young
men with normal or slightly high blood pressure2
1. Grassi G. Sympathetic overdrive in hypertension: clinical and therapeutic relevance. J Cardiol Pract. 2015;13(24):24 November 2015.
2. Heusser K, Vitkovsky J, Raasch W et al. Elevation of sympathetic activity by eprosartan in young male subjects. Am J Hypertens. 2003;16(8):658–64.
Angiotensin-converting enzyme (ACE) CA: Calcium antagonists(CA) Sympathetic nervous system(SNS)
5
7. contents
Myocardial
infarction
Neurohormonal
activation
Arrhythmias
and loss of muscle
Remodelling
Ventricular
enlargement
CHF
Death
Risk factors
• Hyperlipidemia
• Hypertension
• Diabetes
• Smoking
Atherosclerosis
LVH
CHD
Myocardial
ischemia
Coronary
thrombosis
Left ventricular hypertrophy (LVH)
Coronary heart disease (CHD)
Chronic heart failure (CHF)
Beta-blockers can intervene at many points in the
cardiovascular continuum1
1. Adapted from Willenheimer R, Erdmann E. Beta-blockade across the cardiovascular continuum – when and where to use? Eur Heart J Suppls. 2009;11(Suppl A):A1–2.
Sudden
death
Beta-
blockers
Graph adapted from reference 1
6
8. contents
Why beta1-selectivity is important in the treatment of hypertension
associated with sympathetic overdrive1,2
Beta1 receptors Beta2 receptors
Myocardium
Contractility and heart rate1
Myocardial necrosis/apoptosis1
Bronchial smooth muscle Bronchodilation1
Blood vessel smooth
muscle
Vasodilation1
Kidney Renin release1
Primary distribution of beta-receptors and effects of stimulation1
Highly selective beta1-blockers inhibit sympathetic activity in the heart and kidney
reduce the risk of adverse effects mediated by blockade of beta2 receptors in the lungs
and peripheral tissues2
1. Cruickshank JM. The Modern Role of Beta-blockers in Cardiovascular Medicine. Shelton, CT: People's Medical Publishing House-USA;2011
2. Egan BM, Basile J, Chilton RJ et al. Cardioprotection: the role of beta-blocker therapy. J Clin Hypertens. 2005;7(7):409–16.
7
9. contents
Beta-blockers offer additional protection to BP reductions in preventing
recurrent events in patients with a history of CHD1
1. Law MR, Morris JK, Wald NJ. Use of blood pressure lowering drugs in the prevention of cardiovascular disease: meta-analysis of 147 randomised trials in
the context of expectations from prospective epidemiological studies. BMJ. 2009;338:b1665. doi:10.1136/bmj.b1665.
Trials of beta-blockers
People with history of CHD
Entry after acute myocardial infarction
Entry after long term coronary heart disease
People with no history of CHD
Trials other than beta-blocker
People with history of CHD
People with no history of CHD
All trials except ones of beta-blockers in people
with history of CHD
37
27
11
6
37
24
64
2524
2155
369
851
5834
3217
9417
0.71 (0.66 to 0.78)
0.69 (0.62 to 0.76)
0.87 (0.71 to 1.06)
0.89 (0.78 to 1.02)
0.85 (0.79 to 0.91)
0.84 (0.79 to 0.90)
0.85 (0.81 to 0.89)
No of
trials
No of
events
Relative risk
(95% CI)
Relative risk
(95% CI)
p<0.001
Treatment better Placebo better
0.5 0.7 1 1.4 2
Blood pressure(BP) Coronary heart disease(CHD)
Graph adapted from reference 1
8
10. contents
Classification of beta-blockers according to their beta1-
selectivity1,2
Relative beta1-selectivity Non-selective Beta1-selective
• Bupranolol
• Propanolol
• Timolol
• Labetalol
• Carvedilol
• Atenolol
• Metoprolol
• Bisoprolol
• Betaxolol
• Esmolol
Intrinsic sympathomimetic
activity (ISA)
• Alprenolol
• Pindolol
• Oxprenolol
• Carteolol
• Bucindolol
• Acebutolol
• Celiprolol
• Nebivolol*
Hydrophilia
• Nadolol
• Sotalol
• Atenolol
• Celiprolol
1. Egan BM, Basile J, Chilton RJ et al. Cardioprotection: the role of beta-blocker therapy. J Clin Hypertens. 2005;7(7):409–16.
2. López-Sendón J, Swedberg K, McMurray J et al. for the Task Force on Beta-blockers of the European Society of Cardiology. Expert consensus document on
beta-adrenergic receptor blockers. Eur Heart J. 2004;25:1341-62.
3. Cruickshank J. Nebivolol, a third generation beta-blocker. J Symptoms Signs. 2014;3(5):380-91
*Although nebivolol is often characterized as a beta1-selective beta-blocker without ISA, the nitric oxide release induced by nebivolol leading
to vasodilatation results from agonism at beta3-receptors, which is an ISA3
9
11. contents
1. Mancia G, Fagard R, Narkiewcz K et al. 2013 ESH/ESC Guidelines for the management of arterial hypertension: the Task Force for the management of arterial
hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). Eur Heart J. 2013;34:2159–219.
European guidelines recommend beta-blockers for the initiation and
maintenance of antihypertensive treatment1
BP measurements SHOULD ALWAYS be associated with measurement of
heart rate, because resting heart rate values independently predict CV
morbid or fatal events in hypertension
Diuretics, beta-blockers, calcium antagonists, angiotensin converting
enzyme (ACE) inhibitors and angiotensin receptor blockers are all suitable
for the initiation and maintenance of antihypertensive treatment, either as
monotherapy or in some combinations
1
2
Class IA recommendations
Please refer to abbreviated product information in chapter 7 which may vary by country.
10
12. contents
Consider beta-blockers in younger people
with evidence of increased sympathetic drive
The NICE evidence review identified four studies that reported beta-blockers and
ACE inhibitors as being more effective at lowering blood pressure in younger
people than calcium channel blockers or thiazide-type-diuretics.
The guidelines do not generally recommend beta-blockers as a preferred initial
treatment option for hypertensive patients, but beta-blockers may be considered
for initial therapy of hypertension in younger people, particularly:
• those with an intolerance or contraindication to ACE inhibitors and
angiotensin II receptor antagonists or
• women of child-bearing potential or
• people with evidence of increased sympathetic drive.
1. NICE Guideline CG127. Hypertension: The clinical management of primary hypertension in adults. August 2011.
Available at: https://www.nice.org.uk/guidance/cg127/evidence/full-guideline-248588317. Last accessed March 2016.
NICE guidelines also recommend beta-blockers as initial therapy for
hypertension in younger people1
Please refer to abbreviated product information in chapter 7 which may vary by country.
11
13. contents
Bisoprolol (Concor®) indications*
Bisoprolol (Concor®) is indicated for the treatment of:
Reference to local prescribing information to be added here by speakers
Hypertension
Chronic heart failure
Coronary heart disease (angina pectoris)
12
14. contents
Overview of the pharmacokinetics of bisoprolol1-3
Bisoprolol
Absorption >90%3
Bioavailability ~90%1
Plasma protein binding 30%3
Metabolism 50% (inactive)2,3
Plasma elimination half-life 10–12 hours1
1. Leopold G, Kutz K. Bisoprolol: pharmacokinetic profile. Rev Contemp Pharmacother. 1997;8:35-43.
2. Leopold G, Pabst J, Ungethüm W, Bühring K-U. Basic pharmacokinetics of bisoprolol, a new highly beta1-selective adrenoceptor antagonist. J Clin Pharmacol. 1986;26:616-21.
3. Leopold G. Balanced pharmacokinetics and metabolism of bisoprolol. J Cardiovasc Pharmacol. 1986;8(Suppl 11):16–20.
13
15. contents
Bisoprolol has a 'balanced' clearance1,2,3
• 50% renal elimination of unchanged drug
• 50% hepatic metabolism to inactive metabolites – also renally excreted
Metabolism
• Only by oxidation – no subsequent conjugation4,5
• Primarily by CYP3A4 (~95%)4
• Only minor contribution of CYP2D64 ( metabolism not dependent
on CYP2D6 gene polymorphism, formerly debrisoquine-sparteine
polymorphism2)
NO dose adjustment necessary in mild to moderate liver or kidney impairment6
Daily dose to be limited to 10 mg in severe liver or kidney impairment6
Bisoprolol has a balanced clearance
1. Leopold G, Pabst J, Ungethüm W, Bühring K-U. Basic pharmacokinetics of bisoprolol, a new highly beta1-selective adrenoceptor antagonist. J Clin Pharmacol. 1986;26:616-21.
2. Leopold G. Balanced pharmacokinetics and metabolism of bisoprolol. J Cardiovasc Pharmacol. 1986;8(Suppl 11):16–20.
3. Leopold G, Kutz K. Bisoprolol: pharmacokinetic profile. Rev Contemp Pharmacother. 1997;8:35-43.
4. Horikiri Y, Suzuki T, Mizobe M. Stereoselective metabolism of bisoprolol enantiomers in dogs and humans. Life Sci. 1998;63(13):1097-108.
5. Horikiri Y, Suzuki T, Mizobe M. Pharmacokinetics and metabolism of bisoprolol enantiomers in humans. J Pharm Sci. 1998;87(3):289-94.
6. Concor® / Concor® COR Product information (abbreviated prescribing information), Merck KGaA, Darmstadt, Germany; July 2017.
14
16. contents
Beta1-selectivity of different beta-blockers:
bisoprolol is a highly selective beta1-blocker1-5
1. Cruickshank JM. The Modern Role of Beta-blockers in Cardiovascular Medicine. Shelton, CT: People's Medical Publishing House-USA;2011, Fig. 1-5
2. Wellstein A, Palm D, Belz G. Affinity and selectivity of the β-adrenoceptor antagonists in vitro. J Cardiovasc Pharmacol. 1986; 8 (Suppl. 11): 36–40.
3. Wellstein A, Palm D, Betz GG et al. Reduction of exercise tachycardia in man after propranolol and bisoprolol in comparison to beta-adrenoceptor occupancy.
Eur Heart J. 1987; 8 (Suppl. M): 3–8.
4. Maack C, Tyroller S, Schnabel P et al. Characterization of beta1-selectivity, adrenoceptor-Gs-protein interaction and inverse agonism of nebivolol in human myocardium.
Br J Pharmacol. 2001;132:1817–26.
5. Brixius K, Bundkirchen A, Bölck B et al. Nebivolol, bucindolol, metoprolol and carvedilol are devoid of intrinsic sympathomimetic activity in human myocardium.
Br J Pharmacol. 2001;133;1330–8.
Propranolol
Atenolol Betaxolol
Ratio of constants of inhibition (ci/β1 to ci/β2)
Metoprolol
300:1
1:35 1:35
1:75
1.8:1
1:20
ICI 118,551
Increasing beta1-selectivity
Increasing beta2-selectivity
No selectivity
Bisoprolol
Graph adapted from reference 1
Comparisons between the beta1-selectivity of bisoprolol
with that of nebivolol have reported inconsistent results.4,5
15
17. contents
Efficacy of bisoprolol compared with other antihypertensives (GENRES
Study): 24-hour ambulatory BP responses1,2
Systolic
-20
-15
-10
-5
0
5
Bisoprolol Losartan Amlodipine HCT
Systolic
BP
(mmHg)
p<0.001 p<0.01 p<0.001
-20
-15
-10
-5
0
5
Bisoprolol Losartan Amlodipine HCT
Diastolic
BP
(mmHg)
p<0.001 p<0.01 p<0.001
1. Cruickshank JM. Essential Hypertension. Shelton, CT: People's Medical Publishing House-USA;2013, Fig. 6-28
2. Hiltunen TP, Suonsyrjä T, Hannila-Handelberg T et al. Predictors of antihypertensive drug responses: initial data from a placebo-controlled, randomized,
cross-over study with four antihypertensive drugs (The GENRES Study). Am J Hypertens. 2007;20:311-8.
Prospective, randomized double-blind, cross-over, placebo-controlled study in 208 moderately hypertensive men (aged 35 to 60 years):
bisoprolol 5 mg/day, losartan 50 mg/day, amlodipine 5 mg/day, hydrochlorothiazide (HCT) 25 mg/day.
Bisoprolol showed the best antihypertensive effect.
Diastolic
Graph adapted from reference 1
16
18. contents
Sympathetic overdrive in hypertension: the role of beta-blockers with a
focus on bisoprolol
Summary 1/2
• Sympathetic overdrive is associated with the development
of multiple cardiovascular risk factors and is the main cause
of hypertension in young and middle-aged men1,2
• The adverse cardiovascular outcomes associated with
sympathetic overdrive result from the neural release of
norepinephrine and stimulation of beta1 receptors in the
heart and kidneys4
• Beta1-blockade helps to prevent the adverse effects of
sympathetic overdrive and could protect the heart at every
stage of the cardiovascular continuum5
1. Cruickshank JM. Int J Cardiol. 2007;120:10–27; 2. Grassi G. Hypertension. 2009;54(4):690–97; 3. Gillman MW, Kannel WB, Belanger A et al. Am Heart J.
1993;125(4):1148–54; 4. Egan BM, Basile J, Chilton RJ et al. J Clin Hypertens. 2005;7(7):409–16; 5. Willenheimer R, Erdmann E. Eur Heart J Suppls. 2009;11(Suppl
A):A1–2; 6. Mancia G, Fagard R, Narkiewcz K et al. Eur Heart J. 2013;34:2159–219.
17
19. contents
Sympathetic overdrive in hypertension: the role of beta-blockers with a
focus on bisoprolol
Summary 2/2
• Bisoprolol is a highly beta1-selective beta-blocker1-3 , available
as Concor®
• Bisoprolol provides effective 24-hour BP control with once-
daily dosing4
• Bisoprolol is particularly useful for the treatment of young
hypertensive patients with additional risk factors for
sympathetic overdrive:
• Cigarette smoking8
• Overweight or obese9
• Diabetes 10
• High levels of stress11
1. Wellstein A, Palm D, Belz G. J Cardiovasc Pharmacol. 1986; 8 (Suppl. 11): 36–40; 2. Wellstein A, Palm D, Betz GG et al. Eur Heart J. 1987; 8 (Suppl. M): 3–8;
3. Smith C, Teitler M. Cardiovasc Drugs Ther. 1999;13:123–6; 4. References see slide 39; 5. References see slide 48; 6. References see slides 49, 50; 7. References see
slides 53-57; 8. References see slides 49, 13, 14; 9. References see slides 29, 11, 12; 10. References see slides 29, 30, 8; 11. References see slide 10.
18
Editor's Notes
0
Type 2 diabetes is associated with a clustering of coronary risk factors including obesity, insulin resistance, glucose intolerance, hypertension, and dyslipidemia.1 Diabetes has also been associated with sympathetic overdrive, probably resulting from central stimulation by chronically elevated insulin levels.1
High levels of norepinephrine and sustained beta1-receptor activation have been shown to lower the threshold for lethal ventricular arrhythmias, to lead to myocardial myocyte necrosis, apoptosis, and arterial wall damage that predisposes to atheroma, and to local hemodynamic changes that increase the likelihood of atheromatous plaque rupture.1
Chronically high norepinephrine levels also cause high blood pressure, particularly at night (non-dipping), and stimulate renin release from the kidney, leading to angiotensin II formation.1,2 This increases intra-glomerular pressure and predisposes to nephropathy and stimulates further norepinephrine release from peripheral nerve endings, particularly within the heart, thus initiating a vicious cycle between norepinephrine release and angiotensin II activity.1,2
References
1. Cruickshank JM. Beta-blockers and diabetes: the bad guys come good. Cardiovasc Drugs Ther. 2002;16(5):457–70.
2. Cruickshank JM. The Modern Role of Beta-blockers in Cardiovascular Medicine. Shelton, CT: People's Medical Publishing House-USA;2011; Fig. 3-8.
This classic study from the Framingham Group, published in 2005, was one of the first studies to provide clear evidence that the underlying causes of hypertension differed markedly between the young and old.1 The group followed 3915 normal, untreated individuals for 10 years and they reported that, in the young – particularly in men – diastolic hypertension (with or without systolic hypertension) was closely linked to a high body mass index and an increase in weight during follow-up, and resulted from high peripheral resistance. In contrast, the development of systolic hypertension in older individuals was primarily the result of aging, non-compliant (stiff) arteries.
Since obesity is known to be associated with a high sympathetic drive, the results from this and other studies have been interpreted as providing evidence that sympathetic overdrive is the main cause of hypertension in young or middle-aged men.2,3
References
1. Franklin SS, Pio JR, Wong ND et al. Predictors of new-onset diastolic and systolic hypertension. Circulation. 2005;111:1121–7.
2. Cruickshank JM. Are we misunderstanding beta-blockers? Int J Cardiol. 2007;120:10–27.
3. Grassi G. Assessment of sympathetic cardiovascular drive in human hypertension: achievements and perspectives. Hypertension. 2009;54(4):690–97.
A high heart rate is an important marker of sympathetic overdrive and a well-known predictor of future cardiovascular events. This slide presents data from a study that confirmed that an elevated heart rate is a potent risk factor for future cardiac events in patients with hypertension.
The study was conducted to investigate the usefulness of heart rate to predict future cardiac events in patients with ‘high risk’ hypertension. The study used data from the VALUE trial, in which 15,193 patients were followed for up to 5 years. Heart rate was assessed from ECG recordings obtained annually. The primary endpoint was the interval to cardiac events.
After adjustment for confounders (e.g. baseline BP, age, gender and other risk factors), a 10 beats per minute increase in the baseline heart rate was found to be associated with a significant increase in the risk of a cardiac event, heart failure, sudden death, myocardial infarction, stroke or death from all causes. The adjusted hazard ratio for the primary endpoint in the highest heart rate quintile versus the lowest quintile was 1.53 (95% CI 1.26 to 1.85). The incidence of cardiac events in the highest heart rate group (vs. pooled data from the four lower quintiles) was 53% greater in patients whose blood pressure had been well controlled during year 1 of the study (p<0.001).
Reference
1. Julius S, Palatini P, Kjeldsen SE et al. Usefulness of heart rate to predict future cardiac events in treated patients with high-risk systemic hypertension. Am J Cardiol. 2012;109:685–92.
The beneficial effects of reducing heart rate pharmacologically have been demonstrated in patients with myocardial infarction or heart failure.1 In these clinical settings, both beta-blockers and non-dihydropyridine calcium channel blockers have proved to be beneficial in reducing mortality.1
The benefits of reducing heart rate in hypertension have not yet been fully elucidated, however, it has been suggested that drugs that reduce both blood pressure and heart rate might be especially beneficial in hypertensive patients with a high heart rate and other features of sympathetic overdrive.1,2
Current options for pharmacotherapy for elevated heart rate include the non-dihydropyridine calcium channel blockers,1 which reduce nerve conduction velocity and prolong repolarization;2 the beta-blockers without intrinsic sympathomimetic activity (ISA),3 which are associated with a reduction of heart rate by reducing sympathetic overdrive;3 and the If channel blocker, ivabradine, which reduces heart rate by inhibiting the cardiac pacemaker current (If) that controls spontaneous diastolic depolarization in the sinoatrial node.4,5 Although ivabradine reduces heart rate, it is hemodynamically neutral, and does not reduce blood pressure. Ivabradine is therefore not indicated in the treatment of hypertension, but is recommended as a second-line treatment in coronary heart disease when beta-blockers are not tolerated or additional heart rate reductions are needed after the maximum beta-blocker dose has been reached.6,7
Only the beta-blockers without ISA have been shown to reduce heart rate via a direct action on sympathetic overdrive.2, 3, 4, 5
References
1. Palatini P, Benetos A, Julius S. Impact of increased heart rate on clinical outcomes in hypertension: implications for antihypertensive drug therapy. Drugs. 2006;66(2):133–44.
2. Gupta D. A review on calcium channel & its blockers. Int J Pharm Pharm Sci. 2012;4:3842.3. Egan BM, Basile J, Chilton RJ et al. Cardioprotection: the role of β-blocker therapy. J Clin Hypertens. 2005;7(7):409–16.
4. DiFrancesco D, Camm JA. Heart rate lowering by specific and selective I(f) current inhibition with ivabradine: a new therapeutic perspective in cardiovascular disease. Drugs. 2004;64:1757–65.
5. Sulfi S, Timmis AD. Ivabradine: the first selective sinus node I(f) channel inhibitor in the treatment of stable angina. Int J Clin Pract. 2006;60:222–228.
6. Procoralan (ivabradine) Summary of Product Characteristics, revision dated 7 June 2016.
7. Montalescot G, Sechtem U, Achenbach S et al. 2013 ESC guidelines on the management of stable coronary artery disease. Eur Heart J. 2013;34:2949-3003.
Modulation of sympathetic activation is considered an important goal of treatment in cardiovascular disease.1 Sympathetic abnormalities can influence the development and progression of target organ damage, and sympathetic activation is associated with adverse outcomes in terms of morbidity and mortality in a variety of cardiovascular diseases. 1
A reduction in sympathetic cardiovascular drive may lead to favorable cardiovascular outcomes including a decrease in heart rate and myocardial oxygen demand, decreased coronary vascular resistance and increased cardiac and vascular protection.1 Conversely, sympathoexcitatory drugs would have the opposite effect.1
This slide shows the effects of different drug classes on peripheral and cardiac sympathetic drive, illustrating how some drug classes have profound sympathoinhibitory effects (e.g. beta-blockers), some have little if any effects, and some (e.g. diuretics and short-acting calcium antagonists) can increase the adrenergic cardiovascular drive.1 Studies using animal models have suggested that angiotensin II receptor blockers may inhibit the sympathetic nervous system,2 however, these agents have been found to increase sympathetic activity in young men with normal or slightly high blood pressure.2
References
1. Grassi G. Sympathetic overdrive in hypertension: clinical and therapeutic relevance. J Cardiol Pract. 2015;13(24):24 November 2015.
2. Heusser K, Vitkovsky J, Raasch W et al. Elevation of sympathetic activity by eprosartan in young male subjects. Am J Hypertens. 2003;16(8):658–64.
The cardiovascular continuum remains an important cause of premature death and disability, however, its progression is not inevitable.1 Targeted interventions are now available for almost every stage of the continuum, with beta-blockers an effective and well tolerated option at many points along the pathway.1 In this presentation, we are focusing on the use of beta-blockers in patients with hypertension associated with sympathetic overdrive – a key risk factor for the development and progression of cardiovascular disease in young and middle-aged men.
Reference
1. Willenheimer R, Erdmann E. Beta-blockade across the cardiovascular continuum – when and where to use? Eur Heart J Suppls. 2009;11(Suppl A):A1–2.
The beta1-selectivity of beta-blockers is particularly important in the treatment of hypertension associated with sympathetic overdrive. Beta1-receptors are located primarily in the myocardium and kidney, where, when stimulated by norepinephrine, they increase heart rate and renin release.1 Beta2-receptors are located primarily in the bronchial smooth muscle, where they lead to bronchodilation when stimulated,2 and in the blood vessel smooth muscle, where they contribute to vasodilatation.2
Highly beta1-selective beta-blockers therefore have a number of advantages over less selective agents in the treatment of hypertension associated with sympathetic overdrive, as they are associated with a reduction of heart rate and reduce blood pressure via beta1-blockade, they do not interfere with beta2-receptor-mediated vasodilatation, and they are less likely to cause adverse effects (e.g. bronchoconstriction) mediated by blockade of beta2 receptors in the lungs and peripheral tissues.1
References
1. Egan BM, Basile J, Chilton RJ et al. Cardioprotection: the role of beta-blocker therapy. J Clin Hypertens. 2005;7(7):409–16.
2. Cruickshank JM. The Modern Role of Beta-blockers in Cardiovascular Medicine. Shelton, CT: People's Medical Publishing House—USA;2011.
This meta-analysis of 147 randomized studies of blood pressure lowering drugs1 demonstrated that beta-blockers offer additional protection over and above that due to blood pressure reductions in preventing recurrent events in patient with a history of coronary heart disease (CHD).1 This slide shows relative risk estimates for CHD events (fatal or non-fatal myocardial infarction or sudden cardiac death) in blood pressure studies according to drug (beta-blockers or other), the presence or absence of CHD, and, for beta-blockers, according to whether the study recruited patients after an acute myocardial infarction (MI).1
In the 37 studies comparing beta-blockers with placebo (32 studies) or with an untreated control (5 studies) in people with a history of CHD, recurrent CHD events were, on average, reduced by 29% (relative risk 0.71, 95% CI 0.66 to 0.78), significantly greater (p<0.001) than the 15% reduction observed in people with a history of CHD receiving other classes of drugs (relative risk 0.85, 95% CI 0.79 to 0.91).1
The greater protective effect of beta-blockers in people with CHD was explained by a greater effect in the 27 trials that recruited participants at the time of an acute MI (within a month in 25 trials and within 4 months in the other two studies).1 The risk reduction for recurrent CHD events in these 27 trials of people with an acute MI was 31% (relative risk 0.69, 95% CI 0.62 to 0.76).1
This study confirmed that beta-blockers have a special extra effect over and above that related to blood pressure reductions in preventing recurrent CHD events, particularly when used immediately after an acute MI.1
Reference
1. Law MR, Morris JK, Wald NJ. Use of blood pressure lowering drugs in the prevention of cardiovascular disease: meta-analysis of 147 randomised trials in the context of expectations from prospective epidemiological studies. BMJ. 2009;338:b1665. doi:10.1136/bmj.b1665
Beta-blocking agents are usually classified according to their pharmacological properties.1,2 Some non-selective beta-blockers (e.g. propranolol) block both beta1 and beta2 receptors, while others (e.g. atenolol, bisoprolol, and metoprolol) block beta1 receptors preferentially. Because cardiac tissue contains predominantly beta1 receptors, beta1 blockers are considered cardioselective, and they tend to have fewer adverse effects associated with beta2 blockade in the lung and peripheral tissues. Selectivity is dose-dependent: at high doses, some beta1-selective beta-blockers can induce clinically significant antagonism of the beta2 receptors.1
A number of beta-blockers also have intrinsic sympathomimetic activity (ISA) (e.g. acebutolol and pindolol), which leads to weak stimulation of beta-adrenergic receptors while blocking the effects of catecholamines. Beta-blockers with ISA are associated with a reduction of heart rate less effectively than beta-blockers without ISA and provide reduced cardioprotection. They should generally be avoided in heart failure and in post-MI patients. 1
Hydrophilic beta-blockers (e.g. atenolol) are incompletely absorbed from the gastrointestinal tract and are excreted unchanged or as active metabolites by the kidney.2 They do not cross the blood-brain barrier effectively and their elimination half-life is increased in renal insufficiency.2
References
1. Egan BM, Basile J, Chilton RJ et al. Cardioprotection: the role of beta-blocker therapy. J Clin Hypertens. 2005;7(7):409–16.
2. López-Sendón J, Swedberg K, McMurray J et al. for the Task Force on Beta-blockers of the European Society of Cardiology. Expert consensus document on beta-adrenergic receptor blockers. Eur Heart J. 2004;25:1341-62.
3. Cruickshank J. Nebivolol, a third generation beta-blocker. J Symptoms Signs. 2014;3(5):380-91.
10
11
12
Bisoprolol is a highly beta1-selective beta-blocker that was chosen for clinical development because of its pharmacological and pharmacokinetic properties.1 The drug does not have any partial agonistic nor membrane stabilizing activity.1 Bisoprolol has an absolute oral bioavailability of >90%, with virtually no first-pass effect (<10 %).2 The drug has a terminal elimination half-life of 10-12 hours, enabling once-daily dosing, and a clearance of approximately 16 L/hour.1,3 A low plasma protein binding (30%) minimizes the risk of drug interactions and a balanced clearance via renal and hepatic routes ensures that bisoprolol is suitable for use in patients with renal or hepatic insufficiency.2
The pharmacokinetic properties of bisoprolol demonstrate low inter- and intra-patient variability.2
References
1. Leopold G, Kutz K. Bisoprolol: pharmacokinetic profile. Rev Contemp Pharmacother. 1997;8:35-43.
2. Leopold G. Balanced pharmacokinetics and metabolism of bisoprolol. J Cardiovasc Pharmacol. 1986;8(Suppl 11):16–20.
3. Leopold G, Pabst J, Ungethüm W, Bühring K-U. Basic pharmacokinetics of bisoprolol, a new highly beta1-selective adrenoceptor antagonist. J Clin Pharmacol. 1986;26:616-21.
The clearance of bisoprolol is 'balanced' between renal elimination of the unchanged drug (~50%) and hepatic metabolism (~50%) to metabolites that are also renally excreted.1, 2, 3 The total clearance of the drug is 15.6 ± 3.2 L/hour with renal clearance being 9.6 ± 1.6 L/hour.1 In a study with 14C-labelled bisoprolol, the total urinary and fecal excretion was 90 ± 2.7% and 1.4 ± 0.1% of the dose, respectively (mean ± SEM recoveries of the total dose within 168 hours).1
In humans, only oxidative metabolic pathways have been detected for bisoprolol, with no subsequent conjugation.4,5 All metabolites, being very polar, are renally eliminated, and are without pharmacological activity.2 In vitro data from studies in human liver microsomes show that bisoprolol is primarily metabolized via CYP3A4 (~95%) with CYP2D6 having only a minor role.4 The minor contribution of CYP2D6 to the metabolism of bisoprolol observed in vitro is consistent with in vivo data in extensive and restricted debrisoquine metabolizers, which showed no difference between the two groups of metabolizers.2
In patients with hypertension or angina pectoris with liver or kidney function disorders of mild to moderate severity, no dosage adjustment is normally required. 6 In patients with severe renal impairment (creatinine clearance <20 mL/min) and in patients with severe liver function disorders, it is recommended that a daily dose of 10 mg bisoprolol fumarate is not exceeded. 6
Please refer to your local prescribing information.
References
1. Leopold G, Pabst J, Ungethüm W, Bühring K-U. Basic pharmacokinetics of bisoprolol, a new highly beta1-selective adrenoceptor antagonist. J Clin Pharmacol. 1986;26:616-21.
2. Leopold G. Balanced pharmacokinetics and metabolism of bisoprolol. J Cardiovasc Pharmacol. 1986;8(Suppl 11):16–20.
3. Leopold G, Kutz K. Bisoprolol: pharmacokinetic profile. Rev Contemp Pharmacother. 1997;8:35-43.
4. Horikiri Y, Suzuki T, Mizobe M. Stereoselective metabolism of bisoprolol enantiomers in dogs and humans. Life Sci. 1998;63(13):1097-108.
5. Horikiri Y, Suzuki T, Mizobe M. Pharmacokinetics and metabolism of bisoprolol enantiomers in humans. J Pharm Sci. 1998;87(3):289-94
6. Concor® / Concor® COR Product information (abbreviated prescribing information), Merck KGaA, Darmstadt, Germany; July 2017.
In studies comparing the affinity and selectivity of beta-blockers (these early studies did not include nebivolol), bisoprolol was found to have the highest beta1-selectivity of all drugs investigated.1,2,3
One measure of beta1-selectivity is the ratio of the constants of inhibition (inhibition of radioligand binding; ci) for the beta1- and beta2-receptor.3 The constants of inhibition of the beta-blockers, bisoprolol, atenolol, betaxolol and propranolol and the research compound, ICI 118,551 (which has no known therapeutic use in humans but has been used widely in research to understand the action of the beta2 adrenergic receptor) were determined in ligand-binding studies using rat parotid gland (containing mainly beta1-receptors) and rat reticulocytes (containing mainly beta2-receptors) in the presence of human plasma.2 Using a non-specific, radiolabeled ligand, the beta1- and beta2-receptors of the rat parotid gland and reticulocytes were completely occupied.2 This cell suspension was then mixed with the plasma of volunteers pre-treated with different beta-blockers.2 The non-specific radioligand was then displaced from the receptor by addition of this serum enriched with beta-blockers.2 Constants of inhibition of a characteristic magnitude for each beta-blocker and receptor type could be determined from these tests; the smaller the ci-value, the higher the affinity of the beta-blocker for the receptor type concerned. The ratio of ci/β1 to ci/β2 was 1:75 for bisoprolol, 1:35 for atenolol and betaxolol, 1:20 for metoprolol, and 1.8:1 for propranolol.2,3
Comparisons between the beta1-selectivity of bisoprolol with that of nebivolol have reported inconsistent results. Maack et al (2001) reported a higher beta1-selectivity for bisoprolol vs. nebivolol,4 while Brixius et al (2001) found the opposite.5 However, compared with the moderate beta1-selectivity of metoprolol, atenolol, betaxolol,2 both bisoprolol and nebivolol, are highly beta1-selective. 4,5
References
1. Cruickshank JM. The Modern Role of Beta-blockers in Cardiovascular Medicine. Shelton, CT: People's Medical Publishing House-USA;2011, Fig. 1-5.
2. Wellstein A, Palm D, Belz G. Affinity and selectivity of the β-adrenoceptor antagonists in vitro. J Cardiovasc Pharmacol. 1986; 8 (Suppl. 11): 36–40.
3. Wellstein A, Palm D, Betz GG et al. Reduction of exercise tachycardia in man after propranolol and bisoprolol in comparison to beta-adrenoceptor occupancy. Eur Heart J. 1987; 8 (Suppl. M): 3–8.
4. Maack C, Tyroller S, Schnabel P et al. Characterization of 1-selectivity, adrenoceptor-Gs-protein interaction and inverse agonism of nebivolol in human myocardium. Br J Pharmacol. 2001;132:1817–26.
5. Brixius K, Bundkirchen A, Bölck B et al. Nebivolol, bucindolol, metoprolol and carvedilol are devoid of intrinsic sympathomimetic activity in human myocardium. Br J Pharmacol. 2001;133;1330–8.
16
Sympathetic overdrive is associated with the development of many cardiovascular risk factors and it is the main cause of hypertension in young and middle-aged men.1,2 Sympathetic overdrive leads to elevated heart rate and increases the risk of cardiovascular mortality, particularly in middle-aged men with hypertension and/or diabetes.3
The adverse cardiovascular outcomes associated with sympathetic overdrive result from the neural release of norepinephrine and stimulation of beta1 receptors in the heart and kidneys.4 Beta1-blockade helps to prevent the adverse effects of sympathetic overdrive and could protect the heart at every stage of the cardiovascular continuum.5
Beta-blockers are recommended in several current guidelines for the initiation and maintenance of antihypertensive treatment, and there is growing recognition in these guidelines that beta-blockers may be particularly effective in younger patients with sympathetic overdrive.6
1. Cruickshank JM. Int J Cardiol. 2007;120:10–27.
2. Grassi G. Hypertension. 2009;54(4):690–97.
3. Gillman MW, Kannel WB, Belanger A et al. Am Heart J. 1993;125(4):1148–54.
4. Egan BM, Basile J, Chilton RJ et al. J Clin Hypertens. 2005;7(7):409–16.
5. Willenheimer R, Erdmann E. Eur Heart J Suppls. 2009;11(Suppl A):A1–2.
6. Mancia G, Fagard R, Narkiewcz K et al. Eur Heart J. 2013;34:2159–219.
Highly selective beta1-blockers may be preferable to less selective agents when treating patients with hypertension associated with sympathetic overdrive. Highly selective beta1-blockers inhibit sympathetic activity in the heart and kidneys, preserve beta2-mediated vasodilatation, and can reduce the adverse effects mediated by blockade of beta2 receptors in the lungs and peripheral tissues.
Bisoprolol is a highly selective beta1-blocker1-3 that is available as Concor® in more than 90 countries around the world. Bisoprolol provides effective 24-hour blood pressure control with once-daily dosing4, and studies have demonstrated that the treatment is highly effective in comparison to other beta-blockers and other antihypertensive agents in young and middle-aged men. 5 The benefits of bisoprolol have been particularly marked in people who smoke. 6
Bisoprolol has minimal impact on lung function, metabolic parameters and male sexual function, making it suitable for use in a wide range of patients, including those with chronic lung conditions, diabetes or dyslipidemia.7
Bisoprolol is particularly useful for the treatment of young hypertensive patients with additional risk factors for sympathetic overdrive. It may be the preferred option for young hypertensive patients living with high levels of stress11, who smoke,8 who have diabetes10, or who are overweight or obese.9
Thank you for your interest in this toolkit. We hope you will be able make use of these slides when you give talks to other people about this important topic.
1. Wellstein A, Palm D, Belz G. J Cardiovasc Pharmacol. 1986; 8 (Suppl. 11): 36–40.
2. Wellstein A, Palm D, Betz GG et al. Eur Heart J. 1987; 8 (Suppl. M): 3–8. 3. Smith C, Teitler M. Cardiovasc Drugs Ther. 1999;13:123–6.
4. References see slide 39.
5. References see slide 48.
6. References see slides 49, 50.
7.References see slides 53-57.
8. References see slides 49, 13, 14.
9. References see slides 29, 11, 12.
10. References see slides 29, 30, 8.
11. References see slide 10.