
Recommended
Recommended
More Related Content
Similar to Suicide Prevention Training Policies for HealthCare Profess.docx
Similar to Suicide Prevention Training Policies for HealthCare Profess.docx (20)
More from fredr6
More from fredr6 (20)
Recently uploaded
Recently uploaded (20)
Suicide Prevention Training Policies for HealthCare Profess.docx
- 1. Suicide Prevention Training: Policies for Health Care Professionals Across the United States as of October 2017 Janessa M. Graves, PhD, MPH, Jessica L. Mackelprang, PhD, Sara E. Van Natta, RN, and Carrie Holliday, PhD, MN, ARNP Objectives. To identify and compare state policies for suicide prevention training among health care professionals across the United States and benchmark state plan updates against national recommendations set by the surgeon general and the National Action Alliance for Suicide Prevention in 2012. Methods. We searched state legislation databases to identify policies, which we de- scribed and characterized by date of adoption, target audience, and duration and fre- quency of the training. We used descriptive statistics to summarize state-by-state variation in suicide education policies. Results. In the United States, as of October 9, 2017, 10 (20%) states had passed
- 2. legislation mandating health care professionals complete suicide prevention training, and 7 (14%) had policies encouraging training. The content and scope of policies varied substantially. Most states (n = 43) had a state suicide prevention plan that had been revised since 2012, but 7 lacked an updated plan. Conclusions. Considerable variation in suicide prevention training for health care pro- fessionals exists across the United States. There is a need for consistent polices in suicide prevention training across the nation to better equip health care providers to address the needs of patients who may be at risk for suicide. (Am J Public Health. 2018;108:760– 768. doi:10.2105/AJPH.2018.304373) See also Caine and Cross, p. 717. The number of suicides annually in theUnited States exceeds that of traffic crashes or homicide, rendering it the 10th leading cause of death.1 In 2013, 42 826 in- dividuals died by suicide in theUnited States.1 The mortality rate for suicide has increased 24% since 1999 and is currently 13 per 100 000 people,which equates to 115 suicides
- 3. every day.2 Because of its high incidence and potential for prevention, determining how to most effectively prevent suicide is a public health imperative.3 Health care professionals regularly en- counter patients at risk for suicide. In an Australian study, 75% of individuals who died by suicide had seen a health care professional within 3 months preceding their death.4 This suggests health care professionals may play a critical role in identifying at-risk patients and in preventing suicide. However, health care professionals are often not equipped with the training necessary to effectively identify and manage patients at risk for suicide.3,5,6 Even among mental health providers, training in suicide assessment and intervention is not ubiquitous, despite calls for increased training since the late 1980s.7–9 Patients at risk for suicide may, therefore, be inadequately identified and not receive appropriate treatment. In 2001, the US surgeon general released National Strategy for Suicide Prevention, a groundbreaking report that outlined a series of goals to galvanize the nation’s suicide prevention efforts, which included urging states to develop comprehensive suicide prevention plans.10 The subsequent report, issued in 2012 by the surgeon general and the National Action Alliance for Suicide Pre- vention, noted variation in state plans (in-
- 4. cluding the need to address suicide across the lifespan), underscored the importance of in- cluding multiple sectors in prevention plans, and emphasized that education on suicide prevention should be mandated by cre- dentialing and accreditation bodies relevant to health professions.3 Specifically, the report stated that undergraduate and graduate pro- grams for health professionals should “ensure that graduates achieve the relevant core competencies in suicide prevention appro- priate for their respective discipline.”(p47) That report further established benchmark standards for suicide prevention education by advising that curricula be evidence based and by describing ways states may promote the adoption of suicide prevention training by legislating minimum standards of training. The 2012 National Strategy for Suicide Pre- vention was not alone in encouraging suicide awareness and prevention education for health care professionals. The World Health Organization asserted that health care pro- fessionals (e.g., physicians, nurses, psychologists, social workers, emergency medical staff) are among the key stakeholders responsible for preventing suicide. Indeed, suicide prevention experts have reiterated that health care pro- fessionals are in an optimal position to contribute to suicide prevention, if properly trained.9 ABOUT THE AUTHORS Janessa M. Graves, Carrie Holliday, and Sara Van Natta are with the College of Nursing, Washington State University,
- 5. Spokane. Jessica L. Mackelprang is with the Department of Psychological Sciences, Swinburne University of Technology, Melbourne, Australia. Sara E. Van Natta is also with Seattle Children’s Hospital, Seattle, WA. Correspondence should be sent to Janessa M.Graves,Washington State University, College of Nursing, POBox 1495, Spokane, WA 99210 (e-mail: [email protected]). Reprints can be ordered at http://www.ajph.org by clicking the “Reprints” link. This article was accepted February 8, 2018. doi: 10.2105/AJPH.2018.304373 760 Public Health Ethics Peer Reviewed Graves et al. AJPH June 2018, Vol 108, No. 6 AJPH LAW & ETHICS mailto:[email protected] http://www.ajph.org In response to these calls to action, some states have implemented policies that en- courage or require suicide prevention training for “qualified health care professionals,” a broad descriptor defined differently be- tween states. With the passing of the Matt Adler Suicide Assessment, Treatment, and Management Act (“Adler Act”; House Bill 2366), Washington became the first state to mandate suicide-related training in clinical practice. The Adler Act was passed in 2012 and requires the following “qualified health care professionals” to complete suicide pre- vention and assessment training: advisers,
- 6. counselors, chemical dependency pro- fessionals, marriage and family therapists, mental health counselors, occupational therapy practitioners, psychologists, and social workers. In 2014, the Adler Act was amended to include additional disciplines: chiropractors, dentists, dental hygienists, naturopaths, licensed practical nurses, registered nurses, advanced registered nurse practitioners, physicians and surgeons (allopathic and os- teopathic), physician assistants (allopathic and osteopathic), physical therapists, and physical therapist assistants (House Bill 2315, 2014). Effective July 23, 2017, the listedWashington health care professionals were mandated to complete at least 6 hours of continuing ed- ucation on suicide assessment, treatment, and management. Trainings must be established in consultation with experts and must “in- clude content specific to veterans and the assessment of issues related to imminent harm via lethal means or self-injurious behaviors.” For select professions identified by disci- plining authorities (e.g., pharmacists, den- tists), training may be reduced to 3 hours. After the passage of the Adler Act, several states developed similar legislation; however, the status of and variation in state-based policies mandating suicide prevention train- ing has not been reported. We documented the status of state suicide prevention plans and examined policies mandating suicide pre- vention training for qualified health care
- 7. professionals across the United States, in- cluding variation in the target audience, duration of mandated training, and frequency of training. Determining how laws vary across the nation may aid states in developing or refining legislation related to suicide pre- vention education, potentially promoting greater consistency of training between states. This may, in turn, lead to improvements in suicide prevention, assessment, management, and treatment on a national scale. METHODS We employed 2 approaches to identify state policies related to suicide prevention education for health care providers. We queried online legislation databases for each state legislative branch (e.g., Washington State: www.apps.gov.wa/billinfo). Because the search capacity of some state databases is limited, we also searched for legislative in- formation from each state’s House and Senate using 2 legislation tracking services that record the history, updates, and ongoing processes of state bills (i.e., Open States and LegiScan) to ensure that the data were comprehensive.We used the following search terms: “suicide,” “suicide prevention training,” “health care professional,” and “health care professional.” We conducted an initial search on January 28, 2017. We repeated the search on October 9, 2017. We re-reviewed all policies to ensure bill data were up to date.
- 8. We employed 2 methods to ensure the validity of policy data. First, we examined historical notes for each law, such as legislative bills and initiatives (available on state data- bases) for policy details, information, focus, and specific action dates (e.g., date of adop- tion). We coded amendments to bills as data for that piece of legislation, thereby over- riding the original version of the bill. Second, we located supplemental documentation using resources archived online by the Suicide Prevention Resource Center.11 We first identified states’ most recent suicide pre- vention plans through the Suicide Prevention Resource Center archive and then confirmed them individually via state government Web sites. If we could not locate state plans, we obtained confirmation via online search en- gines or communication with state contacts listed on the Suicide Prevention Resource Center Web site. Definitions We defined suicide prevention training as any training intended to inform qualified health care professionals about suicide prevention, assessment, management, or treatment. We separated qualified health care professionals into 2 categories: (1) mental health and behavioral health care pro- fessionals, and (2) general health care pro- fessionals. The definition of a health care professional varies between states. For ex- ample, the bill mandating suicide prevention
- 9. training for health care professionals in Utah (House Bill 209, signed 2015) targets be- havioral health care professionals, defined as recreational therapists, social workers, mar- riage and family therapists, clinical mental health counselors, and substance use disorder counselors. In Washington State, the defi- nition is broader; it includes registered nurses and physicians, among others. For the purpose of this study,mental health and behavioral health care professionals were professionals who provide clinical care with the objective of improving mental health or conducting mental health research. These included psychiatrists, psychologists, social workers, counselors (including rehabilitation counselors and licensed behavioral coun- selors), behavior analysts, psychiatric and mental health nurse practitioners, and occu- pational therapists. General health care professionals included physicians (not psy- chiatrists), nurse practitioners (not explicitly defined as psychiatric or mental health nurse practitioners), certified nurse specialists, physician assistants, certified nurse midwives, certified registered nurse anesthetists, physical therapists, medical assistants, licensed practical nurses, and registered nurses. Policy Variables We coded each state policy in relation to the following characteristics: law or bill name and number, date of adoption, target audience, training duration, and training
- 10. frequency. We defined target audience as the groups of qualified health care pro- fessionals mandated to receive training. Date of adoption was the day, month, and year when the policy was signed or approved by the governor after being passed by the leg- islature or when the policy was ratified, whichever occurred first. Duration was the length of the training (in hours) mandated by the legislation. Duration included the initial training duration and subsequent required training, if specified. Frequency of training AJPH LAW & ETHICS June 2018, Vol 108, No. 6 AJPH Graves et al. Peer Reviewed Public Health Ethics 761 http://www.apps.gov.wa/billinfo was how often the training must be completed. We coded each state suicide prevention plan dichotomously as “updated” (amended or issued in 2012 or after) or “not updated” (issued before 2012 and thereby lacking amendment in response to the 2012 National Strategy for Suicide Prevention).3 Data Analysis We entered data into Microsoft Excel (Microsoft Corp., Redmond, WA) to sum- marize variables.We used descriptive statistics
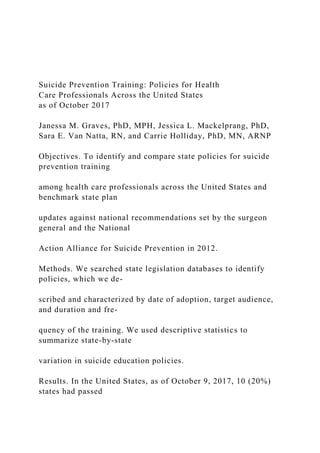
- 11. (e.g., frequency distributions, counts) to de- scribe variation in legislative characteristics across the United States, including existence of a policy, target audience, duration and frequency of training, and updated versus not updated. RESULTS As ofOctober 9, 2017, all states had a state suicide prevention plan. Forty-three (86%) states had a state suicide prevention plan that had been issued or revised in 2012 or later (Figure 1; Figure A, available as a supple- ment to the online version of this article at http://www.ajph.org), whereas 7 (14%) states did not (Table 1). Most state suicide prevention plans were written for the general population, but a few (e.g., Oregon, Pennsylvania) had plans for suicide pre- vention among youths or older adults specifically. Sixteen (32%) states had a policy related to suicide prevention training for health care professionals generally or for mental or be- havioral health care professionals specifically, 10 of which had 1 ormore policies mandating training for qualified health care professionals (Table 2). In most states, the target audience was mental or behavioral health care pro- fessionals (Table 2). In Indiana, the target audience was emergency medical services providers exclusively. In Washington, Nevada, and West Virginia, general health
- 12. care professionals (e.g., nurses, physicians) were also required to complete training. The duration and frequency of training mandated in those 10 states varied from 1 or more hours on license renewal to 6 hours every 6 years (Table 2). The training requirements for mental and behavioral health care pro- fessionals in Washington State were more stringent than were the requirements for general health care providers (i.e., 6 hours every 6 years vs 6 hours 1 time). Seven states had enacted policies that encourage qualified health care professionals to complete suicide prevention training (Tables 1 and 2; Figure B, available as a sup- plement to the online version of this article at http://www.ajph.org). For example, Mon- tana required the state suicide prevention program to include training related to suicide assessment for health care professionals. Similarly, Colorado encouraged the Suicide Prevention Commission, among other enti- ties, to host training opportunities for health care providers (Table 2). Training was not mandated in any of those states, however, except Indiana, where training was both mandated and encouraged. In addition to the 16 states with legislation mandating or encouraging training for health care providers, 5 had legislation in progress at the time of this writing that, if passed, would affect training on suicide prevention for health care professionals (Table 1; Figure B).
- 13. Of the 2 bills under consideration inMissouri, 1 would mandate training for mental or be- havioral health care providers and the other would require training for pharmacists. In New Jersey, the proposed policies related specifically to general health care providers who care for pediatric patients. Texas had 2 bills in progress, 1 targeting general health care professionals and 1 focusing onmental or behavioral health care professionals. The bill under consideration in Virginia would re- quire training for general health care pro- fessionals. Lastly, North Carolina had a bill in progress related to state suicide prevention plan activities, including providing, but not requiring, training for health care providers. Connecticut, Maine, and Minnesota had bills that failed to pass the Senate or House in recent years and did not have policies under consideration at the time of this study. 2% 2% 2% 2% 2% 4% 12% 10% 8% 18% 18% 20% 0
- 16. St at es Year Updated prior to 2012 Updated in 2012 or later (n = 1)(n = 1) (n = 1) (n = 1) (n = 1) (n = 2) (n = 6) (n = 5) (n = 4) (n = 9) (n = 9) (n = 10) FIGURE 1—Publication Years for US State Suicide Prevention Plans Relative toRelease of the 2012National Strategy for Suicide Prevention as of October 9, 2017 AJPH LAW & ETHICS 762 Public Health Ethics Peer Reviewed Graves et al. AJPH June 2018, Vol 108, No. 6 http://www.ajph.org http://www.ajph.org
- 17. TABLE 1—Status of State Suicide Prevention Plans in the United States on October 9, 2017 Suicide Prevention Plan Status and Scope of Suicide Prevention Training Policy State Not Revised Since 2012 Revised Since 2012 Adopted, Requires Training Adopted, Encourages Training In Progress, Requires Training In Progress, Encourages Training No Policy Alabama X X Alaska X X Arizona X X
- 18. Arkansas X X California X X Colorado X X Connecticut X X Delaware X X Florida X X Georgia X X Hawaii X X Idaho X X Illinois X X Indiana X X X Iowa X X Kansas X X Kentucky X X Louisiana X X Maine X X Maryland X X Massachusetts X X
- 19. Michigan X X Minnesota X X Mississippi X X Missouri X X Montana X X Nebraska X X Nevada X X X New Hampshire X X New Jersey X X New Mexico X X New York X X North Carolina X X North Dakota X X Ohio X X
- 20. Oklahoma X X Oregon X X Pennsylvania X X Continued AJPH LAW & ETHICS June 2018, Vol 108, No. 6 AJPH Graves et al. Peer Reviewed Public Health Ethics 763 Among the 24 states that had made progress in expanding suicide prevention training by either mandating, encouraging, or introducing bills (i.e., under consideration or failed) that would strengthen training re- quirements for health care professionals, 5 (i.e., California, Illinois, Louisiana, Michigan, and West Virginia) had not revised their state suicide prevention plan since 2012. DISCUSSION The 2012 National Strategy for Suicide Pre- vention outlined priority areas and strategic directions for suicide prevention on a national scale, including the importance of compre- hensive state-based suicide prevention plans and suicide prevention training for personnel in health professions. We documented the status of state suicide prevention plans across
- 21. the United States and examined policies mandating suicide prevention training for health care professionals. According to this study, 5 years after the release of the 2012 report, 14% (n= 7) of states had yet to revise their plans in accordance with the updated national strategy. However, there has been a surge in the number of plans updated in recent years (Figure 1), which may indicate collective momentum toward preventing suicide across the nation. Despite the explicit recommendation that education on suicide prevention be incorporated into the training of health care professionals, however, few states require such education. It is critical that each state maintain a comprehensive suicide prevention plan that tailors national recommendations to the unique needs of their population. State plans are essential for identifying and engaging relevant stakeholders, including credentialing bodies that oversee the practice of health care professionals, and to ensuring implementa- tion of actions toward attaining suicide pre- vention goals. Of the 10 states with a policy mandating that health care professionals complete training specific to suicide pre- vention, most targeted mental and behavioral health care professionals. Only 3 (i.e., Nevada, Washington, West Virginia) have broadened the target audience to include some general health care professionals, and 1 (i.e., Indiana) included only professionals who deliver emergencymedical services.We hope
- 22. more states will heed the urgings of the surgeon general, the National Alliance for Suicide Prevention, and suicide prevention experts to ensure that the spectrum of health care providers are sufficiently trained.3,12 Health care professionals are uniquely situated to identify individuals who may be at risk for suicide and to provide or facilitate access to treatment. However, this is possible only if health care professionals are equipped with the necessary knowledge and skills to intervene in an ethical and evidence-based manner. Schmitz et al. argue that the “lack of training required of mental health pro- fessionals regarding suicide has been an egregious, enduring oversight by the mental health disciplines.”9(p297) The same can be argued for other health care professionals, who, despite limited training, are often the primary communicators with patients at risk for suicide. For example, nurses are frontline providers who interact with patients at risk for suicide; however, such patients may not be identified because of the lack of suicide prevention training in nursing curricula.5 General health care professionals are also more likely than are mental health providers to be the last point of contact in the health care system for a suicide decedent.4,13,14 Because of the variability in state plans, it should come as no surprise that in a recent study, Silva et al. found differences in suicide knowledge and confidence in working with suicidal people
- 23. among a large sample of behavioral health professionals from several states.15 States with the highest levels of knowledge had enacted suicide prevention initiatives several years before the study, which the authors posited may have explained the differences. The toll of suicide across the United States is great in terms of emotional suffering, TABLE 1—Continued Suicide Prevention Plan Status and Scope of Suicide Prevention Training Policy State Not Revised Since 2012 Revised Since 2012 Adopted, Requires Training Adopted, Encourages Training In Progress, Requires Training In Progress, Encourages Training No
- 24. Policy Rhode Island X X South Carolina X X South Dakota X X Tennessee X X Texas X X Utah X X Vermont X X Virginia X X Washington X X West Virginia X X Wisconsin X X Wyoming X X AJPH LAW & ETHICS 764 Public Health Ethics Peer Reviewed Graves et al. AJPH June 2018, Vol 108, No. 6
- 25. TABLE 2—Target Audience, Duration, Frequency, Date of Adoption, Bill and State Policies Related to Suicide Prevention Training for Health Care Professionals in the United States on October 9, 2017 State Law or Bill Date of Adoption Target Audience or Content/Explanation Minimum Duration and Frequency States with laws that require training California Assembly Bill 89 09/01/2017 Psychologists 6 h at the point of licensure, renewal, or reinstatement Indiana House Bill 1430a 04/28/2017 Emergency medical services providers Not specified Kentucky KRS 210:366 (House Bill 92)b 03/20/2015 Social workers, marriage and family therapists, professional counselors, pastoral counselors, and psychologists; alcohol and drug counselors, occupational therapists, peer support specialists 6 h every 6 y (3-h training may be approved for content appropriate for profession or if content is
- 26. outside the professional’s scope of practice) Nevada Assembly Bill 105c 05/26/2017 Physicians, physician assistants, advanced practice registered nurses, osteopathic physicians, psychologists, certified autism behavior interventionists 2 h within 2 y of initial licensure; 2 h every 4 y thereafter Detoxification technicians, alcohol, drug, and gambling counselors 1 h of instruction for each year of certification Marriage and family therapists, clinical professional counselors 2 h every 2 y to renew license Assembly Bill 387 05/08/2017 Social workers 2 h every 2 y to renew license Senate Bill 286 06/14/2017 Licensed behavior analysts, licensed assistant behavior analysts 2 h as condition of license renewal New Hampshire Senate Bill 33 05/07/2015 Pastoral psychotherapists, clinical social workers, clinicalmental health counselors, marriage and family therapists 3 h every 2 y to renew license Pennsylvania House Bill 64 07/08/2016 Psychologists, social workers, marriage and family therapists, professional counselors 1 h as a condition to renew license
- 27. Tennessee Senate Bill 489; House Bill 948 05/19/2017 Social workers, marriage and family therapists, professional counselors, pastoral counselors, alcohol and drug abuse counselors, psychologists, occupational therapists, other direct staff working in the field of mental health and substance abuse 2 h every 2 y Utah House Bill 209 03/23/2015 Therapeutic recreation technicians, recreation specialists, recreational therapists, clinical social workers, certified social workers, social service workers, marriage and family therapists, clinical mental health counselors, substance use disorder counselors 2 h as condition of licensure and license renewal Washington RCW 43.70.442 (House Bill 1424)d 05/10/2017 Chiropractors, dentists, dental hygienists, naturopaths, licensed
- 28. practical nurses, registered nurses, advanced registered nurse practitioners, osteopathic physicians, osteopathic physician assistants, physical therapists, physical therapist assistants, physicians, physician assistants (does not include certified registered nurse anesthetists, osteopathic physicians and surgeons who hold a postgraduate license in osteopathic medicine or surgery, or physicians who are residents holding a limited license) 6 h 1 time (3-h training may be approved if content is outside the professional’s scope of practice) Advisers, counselors, chemical dependency professionals, marriage and family therapists, mental health counselors, occupational therapy practitioners, psychologists, advanced social workers, independent clinical social workers, social worker associates 6 h every 6 y (3-h training may be approved if content is outside the professional’s scope of practice)
- 29. West Virginia House Bill 2804e 04/26/2017 Registered professional nurses (registered nurses and licenses practical nurses), advanced nurse practitioners, psychologists, social workers, professional counselors 2 h for each renewal/reporting period for continuing education requirements States with laws that encourage training Colorado Senate Bill 147 05/04/2016 Suicide prevention commission and other entities are strongly encouraged to develop and implement professional development resources and training opportunities for health systems, including mental and behavioral health systems, primary care providers, physician and mental health clinics in educational institutions, and community mental health centers NA Continued AJPH LAW & ETHICS
- 30. June 2018, Vol 108, No. 6 AJPH Graves et al. Peer Reviewed Public Health Ethics 765 medical costs, and lost productivity. That burden is carried by individuals who expe- rience suicidal ideation and survive attempts, the loved ones of those individuals and those bereaved by suicide, and the health care professionals who care for those individuals and families. Death of a patient by suicide has serious personal and professional ramifications for health care providers.16–19 Although health care professionals are routinely tasked with the responsibility of providing care to patients who may be at risk for suicide, ed- ucation on the topic is not a compulsory aspect of most educational programs. Despite calls to action over 3 decades from academics TABLE 2—Continued State Law or Bill Date of Adoption Target Audience or Content/Explanation Minimum Duration and Frequency Hawaii CCR 157 (House Bill 55, HD1 SD2 CD1) 05/03/2007 States that the department of health may establish and operate
- 31. a statewide suicide early intervention and prevention program to carry out suicide prevention training programs for health care providers NA Illinois 410 ILCS 53/30 (House Bill 1643) 08/13/2007 Encourages the director of public health to ensure that pilot suicide prevention plans (outlined in the legislation) include training for health providers and physicians NA Indiana House Bill 1430a 04/27/2017 The Division of Mental Health and Addiction to develop and provide an evidence-based training program for health care providers, including mental health and behavioral health providers NA Louisiana RS 37:24–27 (Senate Bill 539)
- 32. 06/09/2014 Requires the Louisiana Department of Health and Hospitals to offer the following professionals certified, licensed, or registered in Louisiana access to a list of training programs in suicide assessment, intervention, treatment, and management through posting links to such trainings on the department’s official Web site: mental health counselors, social workers, psychiatrists, physicians, surgeons, midwives, psychologists, medical psychologists, registered nurses or advance practice registered nurses, physician assistants, addiction counselors NA Michigan . . .f Public acts related to appropriations for community health that include statements regarding “initiatives that train health care practitioners and faculty in managing pain, providing palliative care and suicide
- 33. prevention” NA Montana MCA 53–21-1101 (Senate Bill 478) 05/08/2007 Requires state suicide prevention officer to direct statewide suicide prevention program with evidence-based activities, including training for medical professionals, social service providers, and other groups on recognizing the early warning signs of suicidality, depression, and other mental illnesses NA Note. NA =not applicable. Data are fromsearchesof individual state legislativeWeb sites,Open States, and LegiScan andare accurate asofOctober 9, 2017. Bills passed subsequent to this date are not included. aIndiana House Bill 1430 includes text requiring emergency medical services providers to complete suicide prevention training as well as text relating to the provision of a suicide prevention training program for health care providers. bKentucky State legislation was originally adopted into law as Senate Bill 72 (2013) and later expanded to include alcohol and drug support peer specialists in 2015 (House Bill 92). cNevada State legislationwasoriginally adopted into
- 34. lawasAssembly Bill 93 (2015) and later amendedwithAssembly Bill 105 (2017), SenateBill 286 (2017), and Assembly Bill 387 (2017) to revise training requirements. dWashington State legislation was originally adopted into law as House Bill 2366 (2012) and was amended in 2013 (House Bill 1376), 2014 (House Bill 2315), 2015 (House Bill 1424), 2016 (House Bill 2793), and 2017 (House Bill 1424). The information here refers to the most recently adopted amendment. eWest Virginia House Bill 2804 specifies that trainingmust pertain tomental health conditions common to veterans and family members of veterans, including training on inquiring aboutwhether the patients are veterans or familymembers of veterans and screening for conditions such as posttraumatic stress disorder, risk of suicide, depression, and grief and prevention of suicide. fSeveral Michigan State Public Acts for appropriations were identified (e.g., 2002 Public Act 519) that include the following statement: “The department shall promote activities that preserve the dignity and rights of terminally ill and chronically ill individuals. Priority shall be given to programs, such as hospice, that focus on individual dignity and quality of care provided persons with terminal illness and programs serving persons with chronic illnesses that reduce the rate of suicide through the advancement of the knowledge and use of improved, appropriate pain management for these persons; and initiatives that train health care practitioners and faculty in managing pain, providing palliative care and suicide prevention.” However, no bills related to suicide prevention education for health care providers (beyond the appropriations) were identified. AJPH LAW & ETHICS
- 35. 766 Public Health Ethics Peer Reviewed Graves et al. AJPH June 2018, Vol 108, No. 6 and policymakers alike, relatively modest increases in suicide prevention training have been observed among health-related training programs. As a result, despite frequently encountering suicidal patients, many mental, behavioral, and general health care professionals continue to report a paucity of training or limited confidence in working with at-risk patients.20,21 Even among health care professionals who endorse a good level of knowledge and confidence in suicide assessment, the majority are keen to receive further training.22 Pre- vious research suggests that lack of training is a common reason qualified health care pro- fessionals have a negative attitude toward working with patients at risk for suicide,23 whichmay affect the quality of care provided. This gap in training calls into question whether health care professionals are in- advertently practicing beyond the boundaries of their competence.9 Studies have shown that suicide prevention training strengthens skills and knowledge and improves attitudes among health care professionals.24–28 Perhaps mandatory trainingwill be necessary to ensure that health care professionals are prepared
- 36. with the skills necessary to identify and sup- port at-risk patients, particularly if future research identifies a relationship between compulsory training and improved patient outcomes. Although legislation may be an effective way to ensure that suicide prevention training is disseminated universally among health care professionals, additional approaches to tack- ling deficits in knowledge and skills exist. Accrediting bodies (e.g., American Psycho- logical Association, Liaison Committee on Medical Education) have a responsibility to ensure that graduates are prepared to identify patients at risk for suicide and to respond appropriately. These bodies could revise standards to introduce core competencies related to suicide assessment, as proposed by Schmitz et al.9 There are also evidence-based gatekeeper trainings produced by professional organizations, such as the Recognizing and Responding to Suicide Risk (http://www. suicidology.org/training-accreditation/rrsr), Applied Suicide Intervention Skills Training (https://www.livingworks.net/programs/ asist), and Question, Persuade, and Refer training (https://www.qprinstitute.com), all of which provide individual- or organization-level training. Limitations and Directions For Future Research The most important measure of the ef-
- 37. fectiveness of policies mandating suicide prevention training for health care pro- fessionals is whether suicide-related outcomes (e.g., rate of completed suicides or hospital- izations for suicide attempts) change. How- ever, limited time has elapsed since the enactment of state policies to demonstrate whether a relationship exists between man- datory training and suicide rates; such data are not yet available. Nonetheless, it is promising that health care professionals in states with established suicide prevention initiatives have been shown to evidence higher knowledge and confidence in working with suicidal people.15 Longitudinal analyses to evaluate whether mandatory suicide prevention training for qualified health care professionals affects state suicide rates may be a viable method. Similar methods were used inRussia to investigate the impact of a national alcohol policy on suicide rates.29 Future research is needed to establish best practice training guidelines for health care professionals. Discussion of access to lethal means should be included, including access to firearms, which are used in 50% of suicides in the United States (this rate is 8 times greater than that of other high-income nations).30 Differences between states should be con- sidered, as some risk factors (e.g., rates of firearm ownership) are associated with par- ticularly high levels of risk.31 Moreover, it behooves states to establish data collection plans at the inception of policy changes; this
- 38. would enable the evaluation of mandated training, including provider knowledge and skills before and after training, fidelity to best practice training approaches, and suicide-related patient outcomes. Currently, the duration and frequency of mandated training vary widely. Some state policies require that a specific number of hours be completed at a particular cadence (e.g., every 2 years) as a component of con- tinuing education (i.e., postlicensure), whereas others mandate that training be completed as a condition of obtaining li- censure. This is problematic, particularly at the doctoral level, because physicians- and psychologists-in-training often relocate to different states to complete their residency or predoctoral internship, respectively. If edu- cation on suicide prevention is mandated for health care professionals only during con- tinuing education, wemust assume that many professionals enter the workforce and take on the responsibility of managing at-risk patients without sufficiently robust skills to do so. The legislative landscape is perpetually changing, and this topic is gaining momen- tum as a governmental priority. Thus, bills under consideration at the time of this writing, for example, may or may not pass. Ongoing monitoring of legislative changes related to suicide prevention education re- quirements for health care professionals will be necessary. Amendments result in updates
- 39. to the date of adoption and, oftentimes, changes in bill numbers. This could com- plicate replication, as policy details—the data —may change with amendments. Because each state defines qualified health pro- fessionals differently, disparate terminology should be considered when evaluating poli- cies on a national level. Lastly, the scope of this studywas limited to universal polices focusing on training for health care professionals, and search results do not include professionals in specialized settings (e.g., schools, correctional facilities). Conclusions Suicide is a serious and preventable public health concern that has substantial and en- during impacts on individuals, families, and communities. We have provided a snapshot of current policies across the nation and dis- cussed means by which knowledge and skills gaps may be addressed. By comparing state policies—specifically the date of adoption or introduction, target audience, duration, and frequency—our findings illustrate the gross variability in policies between states and underscore the amount of work yet to be done to address the priority areas outlined in the 2012 National Strategy for Suicide Pre- vention, including requiring suicide preven- tion education for health care professionals.3 Better equipping health care professionals to assess and provide care to patients at risk for suicide may contribute to a meaningful
- 40. decline in the rate of suicide across the nation, AJPH LAW & ETHICS June 2018, Vol 108, No. 6 AJPH Graves et al. Peer Reviewed Public Health Ethics 767 http://www.suicidology.org/training-accreditation/rrsr http://www.suicidology.org/training-accreditation/rrsr https://www.livingworks.net/programs/asist https://www.livingworks.net/programs/asist https://www.qprinstitute.com and it is the responsibility of policymakers, health care professionals, and citizens to ad- vocate change. CONTRIBUTORS J.M. Graves and J. L. Mackelprang are co-first authors. J.M. Graves and S. E. Van Natta conceptualized the study. S. E. VanNatta conducted the literature review, and J.M. Graves and J. L. Mackelprang collected and summa- rized final policy data. All authors contributed to the in- terpretation of the findings, drafted the article, and provided critical feedback and approval of the final article. ACKNOWLEDGMENTS The authors would like to acknowledge Sarah Schaub for her assistancewithgraphics andGageDeMontHansen, Sc. MPA, and Tracy A. Klein, PhD, FNP, ARNP, FAANP, FRE, FAAN for their review of the article and feedback. HUMAN PARTICIPANT PROTECTION This study did not involve human participants and thus institutional review board approval was not required.
- 41. REFERENCES 1. Kochanek KD, Murphy SL, Xu J, Tejada-Vera B. Deaths: final data for 2014.Natl Vital Stat Rep. 2016;65(4): 1–122. 2. Curtin SC,Warner M, Hedegaard H. Increase in Suicide in the United States, 1999–2014. Hyattsville, MD: Na- tional Center for Health Statistics; 2016. 3. US Department of Health and Human Services. Na- tional strategy for suicide prevention. 2012. Available at: www.actionallianceforsuicideprevention.org/NSSP. Accessed February 9, 2018. 4. De LeoD,Draper BM, Snowdon J, Kõlves K. Contacts with health professionals before suicide: missed oppor- tunities for prevention? Compr Psychiatry. 2013;54(7): 1117–1123. 5. Bolster C, Holliday C, Oneal G, Shaw M. Suicide assessment and nurses: what does the evidence show? Online J Issues Nurs. 2015;20(1):2. 6. Sudak D, Roy A, Sudak H, Lipschitz A, Maltsberger J, Hendin H. Deficiencies in suicide training in primary care specialties: a survey of training directors. Acad Psychiatry. 2007;31(5):345–349. 7. Bongar B, Harmatz M. Graduate training in clinical psychology and the study of suicide. Prof Psychol Res Pr. 1989;20(4):209–213. 8. Dexter-Mazza ET, FreemanKA.Graduate training and the treatment of suicidal clients: the students’ perspective. Suicide Life Threat Behav. 2003;33(2):211–218.
- 42. 9. Schmitz WM, Allen MH, Feldman BN, et al. Pre- venting suicide through improved training in suicide risk assessment and care: an American Association of Suici- dology Task Force report addressing serious gaps in US mental health training. Suicide Life Threat Behav. 2012; 42(3):292–304. 10. US Department of Health and Human Services; Office of the Surgeon General.National Strategy for Suicide Prevention: Goals and Objectives for Action. Rockville, MD: US Public Health Service; 2001. 11. Suicide PreventionResourceCenter. States. Available at: http://www.sprc.org/states. Accessed October 9 2017. 12. Stuber J, Quinnett P.Making the case for primary care and mandated suicide prevention education. Suicide Life Threat Behav. 2013;43(2):117–124. 13. Ahmedani BK, Simon GE, Stewart C, et al. Health care contacts in the year before suicide death. J Gen Intern Med. 2014;29(6):870–877. 14. Luoma JB, Martin CE, Pearson JL. Contact with mental health and primary care providers before suicide: a review of the evidence. Am J Psychiatry. 2002;159(6): 909–916. 15. Silva C, Smith AR, Dodd DR, Covington DW, Joiner TE. Suicide-related knowledge and confidence among behavioral health care staff in seven states. Psychiatr Serv. 2016;67(11):1240–1245. 16. Alexander DA, Klein S, Gray NM, Dewar IG, Eagles
- 43. JM. Suicide by patients: questionnaire study of its effect on consultant psychiatrists. BMJ. 2000;320(7249):1571–1574. 17. Gulfi A, Castelli Dransart DA, Heeb JL, Gutjahr E. The impact of patient suicide on the professional reactions and practices of mental health caregivers and social workers. Crisis. 2010;31(4):202–210. 18. Hendin H, Lipschitz A, Maltsberger JT, Haas AP, Wynecoop S. Therapists’ reactions to patients’ suicides. Am J Psychiatry. 2000;157(12):2022–2027. 19. McAdams CR III, Foster VA. Client suicide: its frequency and impact on counselors. J Ment Health Couns. 2000;22(2):107–121. 20. Jahn DR, Quinnett P, Ries R. The influence of training and experience on mental health practitioners’ comfort workingwith suicidal individuals.Prof Psychol Res Pr. 2016;47(2):130–138. 21.Mackelprang JL, Karle J, Reihl KM,CashRE. Suicide intervention skills: graduate training and exposure to suicide among psychology trainees. Train Educ Prof Psychol. 2014;8(2):136–142. 22.Michail M, Tait L, Churchill D. General practitioners’ clinical expertise in managing suicidal young people: implications for continued education. Prim Health Care Res Dev. 2017;18(5):419–428. 23. Chan SW, Chien WT, Tso S. Evaluating nurses’ knowledge, attitude and competency after an education programme on suicide prevention. Nurse Educ Today. 2009;29(7):763–769.
- 44. 24. Berlim MT, Perizzolo J, Lejderman F, Fleck MP, Joiner TE. Does a brief training on suicide prevention among general hospital personnel impact their baseline attitudes towards suicidal behavior? J Affect Disord. 2007; 100(1):233–239. 25. Fenwick CD, Vassilas CA, Carter H, Hague MS. Training health professionals in the recognition, assess- ment and management of suicide risk. Int J Psychiatry Clin Pract. 2004;8(2):117–121. 26. Kishi Y, Otsuka K, Akiyama K, et al. Effects of a training workshop on suicide prevention among emergency room nurses. Crisis. 2014;35(5):357–361. 27.McNielDE, Fordwood SR,WeaverCM,Chamberlain JR, Hall SE, Binder RL. Effects of training on suicide risk assessment. Psychiatr Serv. 2008;59(12):1462–1465. 28. Santos JC, Simões RM, Erse MP, Façanha JD, Marques LA. Impact of “+ Contigo” training on the knowledge and attitudes of health care professionals about suicide. Rev Lat Am Enfermagem. 2014;22(4):679–684. 29. PridemoreWA,ChamlinMB,Andreev E.Reduction in male suicide mortality following the 2006 Russian alcohol policy: an interrupted time series analysis. Am J Public Health. 2013;103(11):2021–2026. 30. Grinshteyn E, Hemenway D. Violent death rates: the US compared with other high-income OECD countries, 2010. Am J Med. 2016;129(3):266–273. 31. Miller M, Barber C, White RA, Azrael D. Firearms and suicide in the United States: is risk independent of underlying suicidal behavior? Am J Epidemiol. 2013;
- 45. 178(6):946–955. AJPH LAW & ETHICS 768 Public Health Ethics Peer Reviewed Graves et al. AJPH June 2018, Vol 108, No. 6 http://www.actionallianceforsuicideprevention.org/NSSP http://www.sprc.org/states Copyright of American Journal of Public Health is the property of American Public Health Association and its content may not be copied or emailed to multiple sites or posted to a listserv without the copyright holder's express written permission. However, users may print, download, or email articles for individual use.