The document provides an overview of the anatomy, physiology, and pathologies of the small intestine. It discusses the following key points:
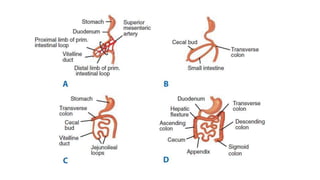
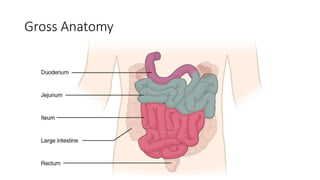
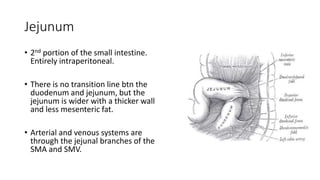
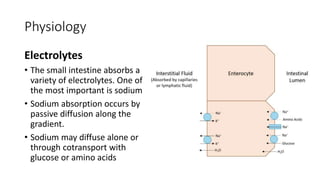
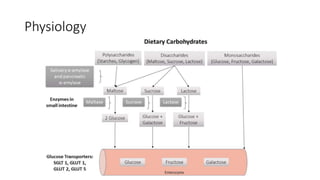
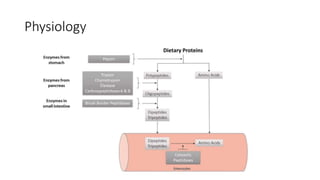
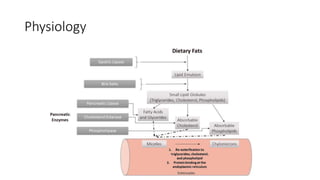
- The small intestine is responsible for digestion and absorption. It starts at the pylorus and ends at the ileocecal valve, measuring around 7 meters long.
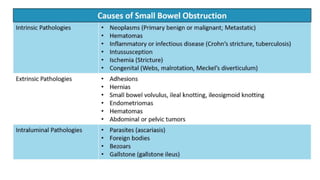
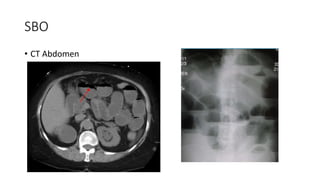
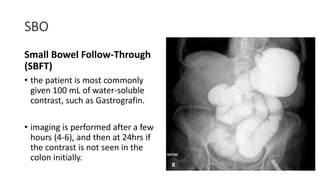
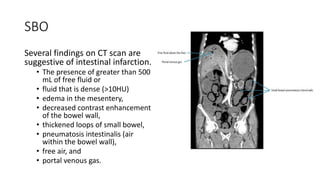
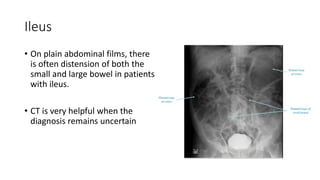
- Common pathologies include small bowel obstruction, which can be diagnosed using imaging like CT scans, and ileus, which results in impaired motility.
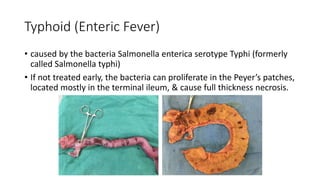
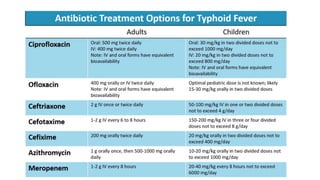
- Infectious diseases like typhoid fever and tuberculosis can also affect the small intestine. Typhoid is caused by Salmonella and can lead to perforation of the ileum if untreated.























































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)














