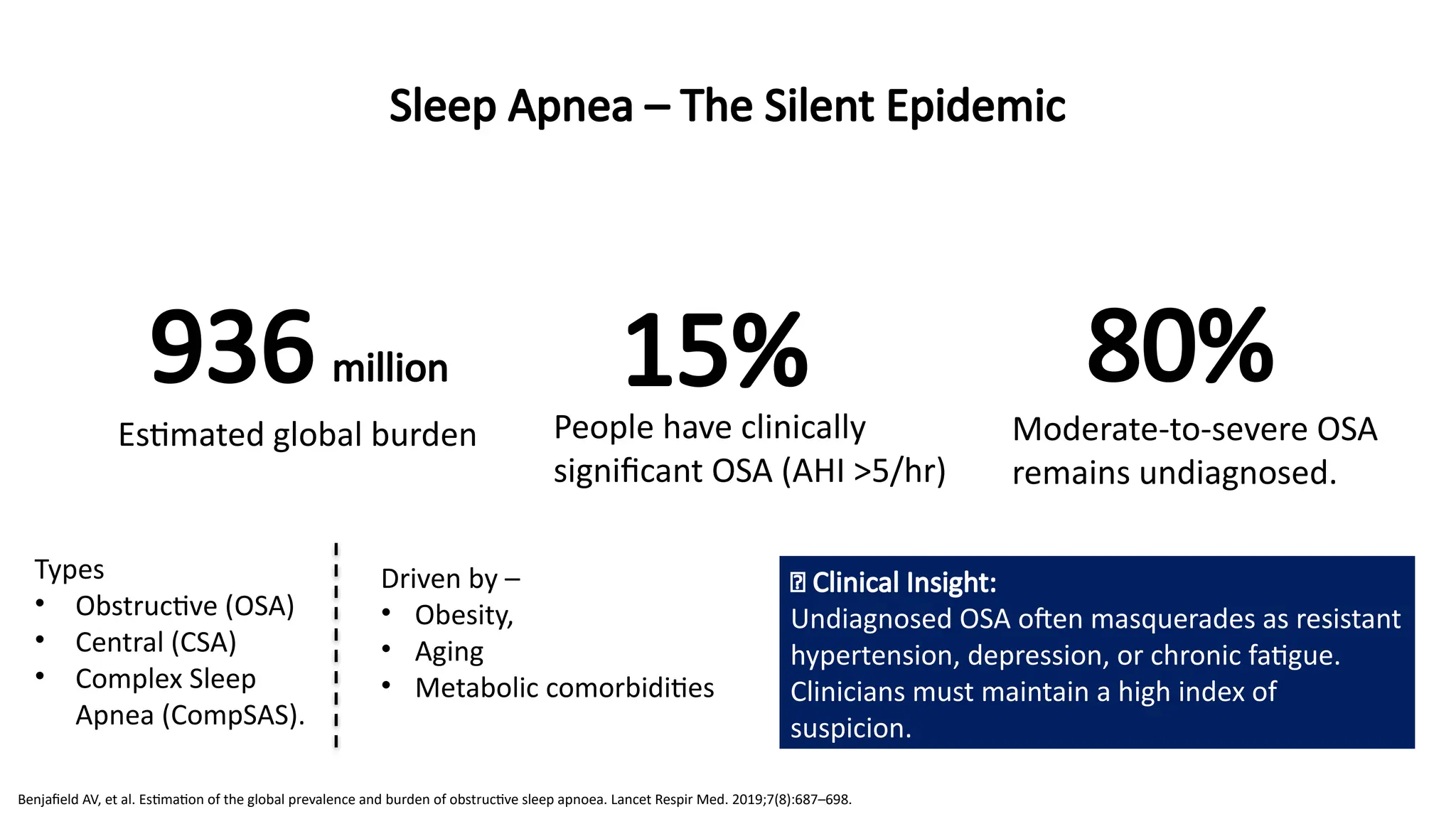
Sleep Apnea –The Silent Epidemic
936 million 15% 80%
Estimated global burden People have clinically
significant OSA (AHI >5/hr)
Moderate-to-severe OSA
remains undiagnosed.
Types
• Obstructive (OSA)
• Central (CSA)
• Complex Sleep
Apnea (CompSAS).
🧠 Clinical Insight:
Undiagnosed OSA often masquerades as resistant
hypertension, depression, or chronic fatigue.
Clinicians must maintain a high index of
suspicion.
Benjafield AV, et al. Estimation of the global prevalence and burden of obstructive sleep apnoea. Lancet Respir Med. 2019;7(8):687–698.
Driven by –
• Obesity,
• Aging
• Metabolic comorbidities
3.
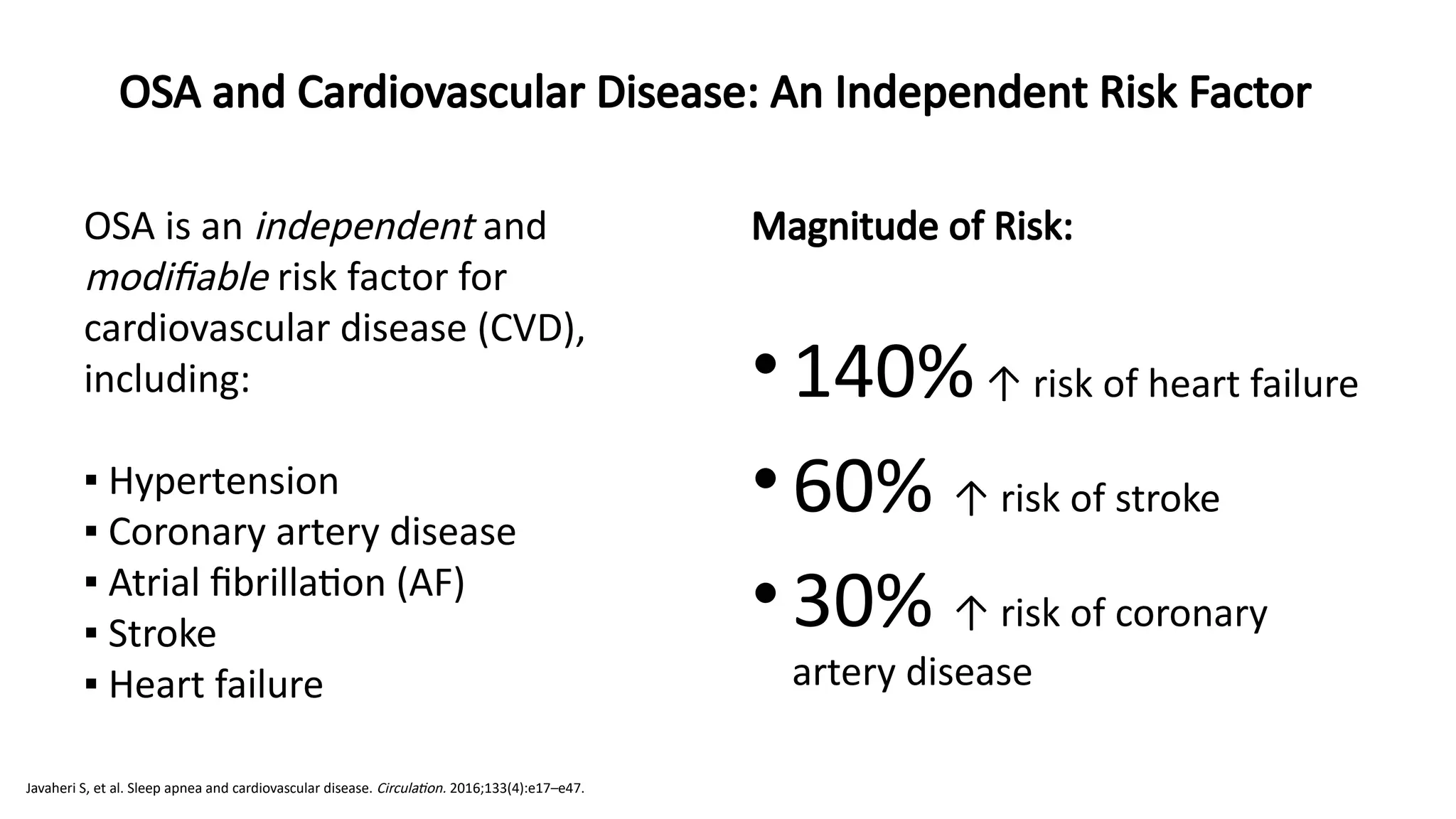
OSA is anindependent and
modifiable risk factor for
cardiovascular disease (CVD),
including:
▪ Hypertension
▪ Coronary artery disease
▪ Atrial fibrillation (AF)
▪ Stroke
▪ Heart failure
Magnitude of Risk:
•140%↑ risk of heart failure
•60% ↑ risk of stroke
•30% ↑ risk of coronary
artery disease
OSA and Cardiovascular Disease: An Independent Risk Factor
Javaheri S, et al. Sleep apnea and cardiovascular disease. Circulation. 2016;133(4):e17–e47.
4.
OSA and CardiovascularDisease: An Independent Risk Factor
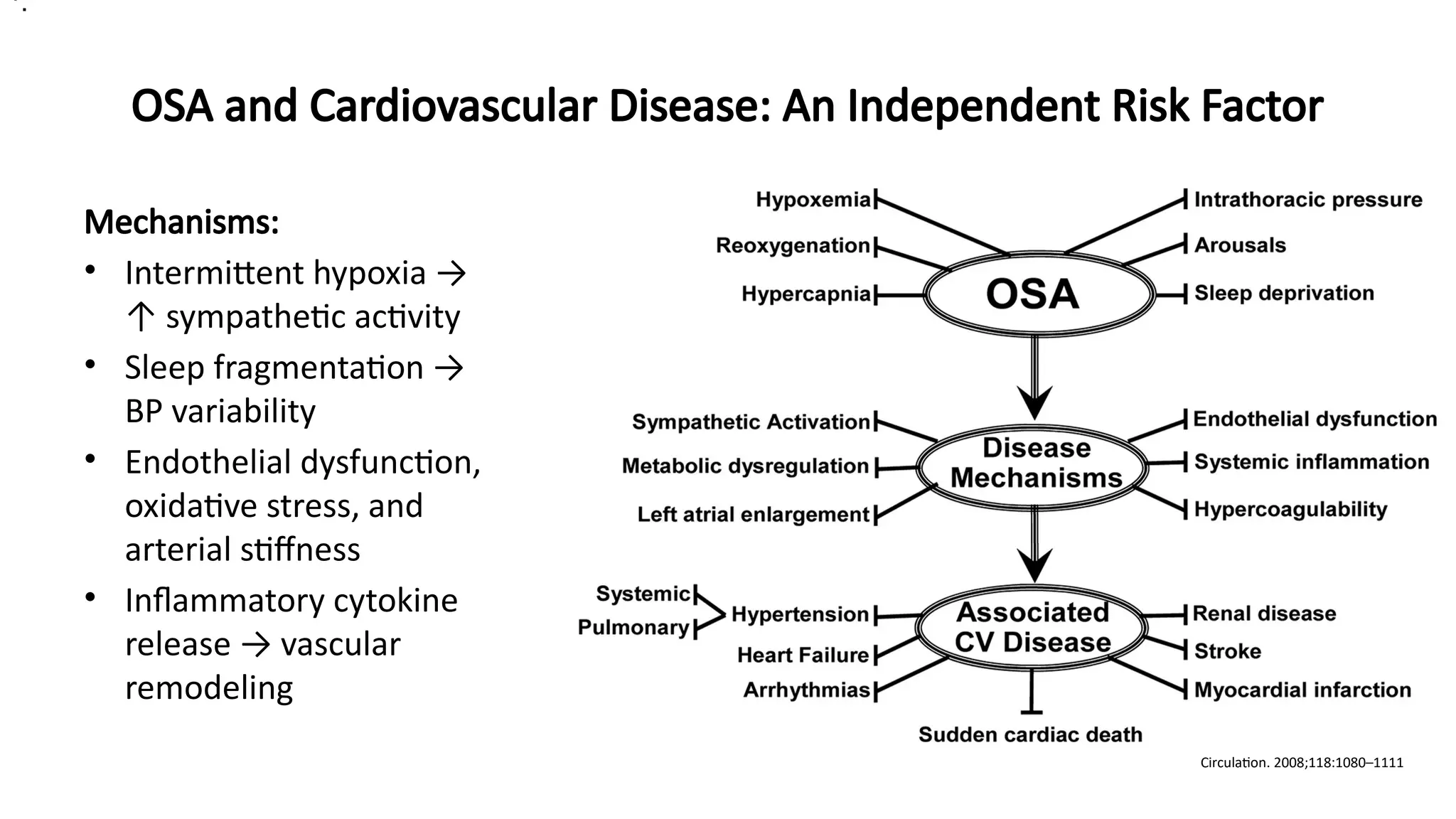
Mechanisms:
• Intermittent hypoxia →
↑ sympathetic activity
• Sleep fragmentation →
BP variability
• Endothelial dysfunction,
oxidative stress, and
arterial stiffness
• Inflammatory cytokine
release → vascular
remodeling
Circulation. 2008;118:1080–1111
•.
5.
OSA and CardiovascularDisease: An Independent Risk Factor
Sánchez-de-la-Torre, Manuel et al. The Lancet Respiratory Medicine, Volume 1, Issue 1, 61 - 72
6.
OSA and CardiovascularDisease: An Independent Risk Factor
•Nocturnal hypertension and a non-dipping BP
pattern are hallmarks of OSA, often missed on
routine clinic measurements.
•The Sleep Heart Health Study and Wisconsin
Sleep Cohort established the dose-response
relationship between OSA severity (AHI) and
CVD risk, independent of BMI.
•Left atrial enlargement, commonly seen in
patients with OSA, can predispose to AF and
worsen its recurrence post-ablation
🧠 Case Nugget:
A 57-year-old male with drug-refractory
hypertension and new-onset paroxysmal
AF is referred for evaluation. Overnight
oximetry shows desaturation; PSG
confirms severe OSA (AHI 42/hr). Post-
CPAP, his BP normalizes, and AF burden
reduces on Holter at 3 months.
💡 Implication:
OSA screening should be part of routine
cardiovascular risk stratification —
especially in patients with resistant
hypertension or arrhythmias.
Marin JM, et al. Long-term cardiovascular outcomes in men with obstructive sleep apnoea–hypopnoea with or without treatment with CPAP: an observational study. Lancet. 2005;365(9464):1046–1053
Young T, et al. Sleep-disordered breathing and cardiovascular disease. JAMA. 2008;300(23):2751–2759.
Am J Respir Crit Care Med Vol 163. pp 19–25, 200
7.
Sleep Apnea andChronic Kidney Disease (CKD): A Two-Way Street
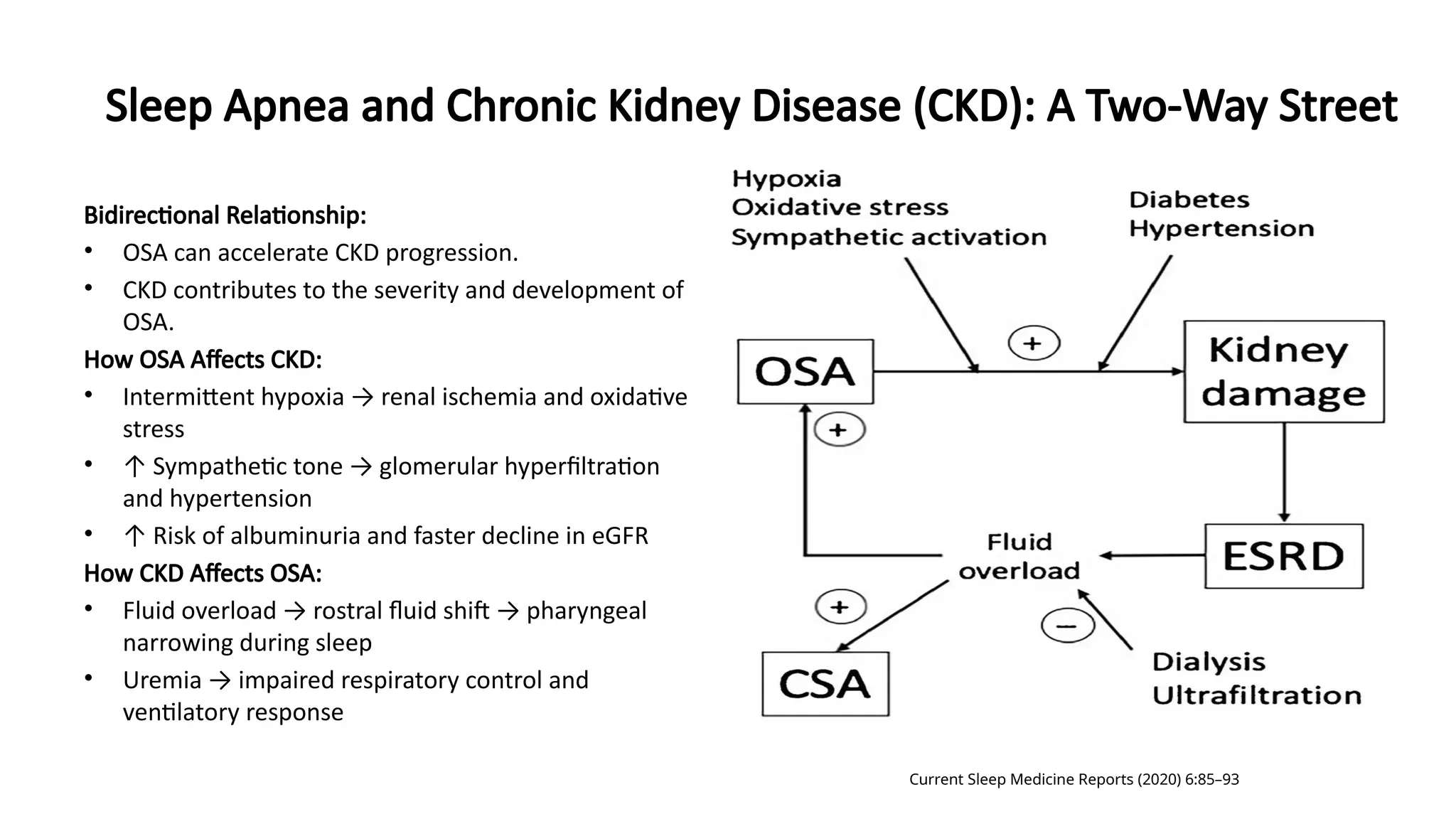
Bidirectional Relationship:
• OSA can accelerate CKD progression.
• CKD contributes to the severity and development of
OSA.
How OSA Affects CKD:
• Intermittent hypoxia → renal ischemia and oxidative
stress
• ↑ Sympathetic tone → glomerular hyperfiltration
and hypertension
• ↑ Risk of albuminuria and faster decline in eGFR
How CKD Affects OSA:
• Fluid overload → rostral fluid shift → pharyngeal
narrowing during sleep
• Uremia → impaired respiratory control and
ventilatory response
Current Sleep Medicine Reports (2020) 6:85–93
8.
Sleep Apnea andChronic Kidney Disease (CKD): A Two-Way Street
• Many CKD patients attribute fatigue to uremia —
but in reality, sleep apnea may be the silent
contributor.
• Fluid shifts, especially when patients lie supine,
worsens pharyngeal obstruction.
• There’s also early evidence linking OSA to
increased renal sympathetic nerve activity,
compounding hypertension.
• Diagnosing OSA early in CKD may slow GFR
decline, reduce BP meds, and improve QoL.
• AHI severity correlates with proteinuria levels in
observational studies.
• For patients on dialysis, untreated OSA is linked to
higher cardiovascular mortality.
Lin CH, Perger E, Lyons OD. Obstructive sleep apnea and chronic kidney disease. Curr Opin Pulm Med. 2018 Nov;24(6):549-554
🧠 Case Nugget:
65-year-old male on maintenance
hemodialysis reports persistent fatigue and
poor sleep. Overnight pulse oximetry reveals
desaturation with frequent apneic spells. PSG
confirms severe OSA. CPAP initiated →
improved morning BP and alertness. eGFR
decline stabilizes over 6 months.
💡 Implication:
Suspect OSA in dialysis or pre-dialysis patients
with excessive daytime sleepiness, refractory
hypertension, or volume overload despite
adherence.
9.
OSA and LungDiseases – The Overlap Syndrome
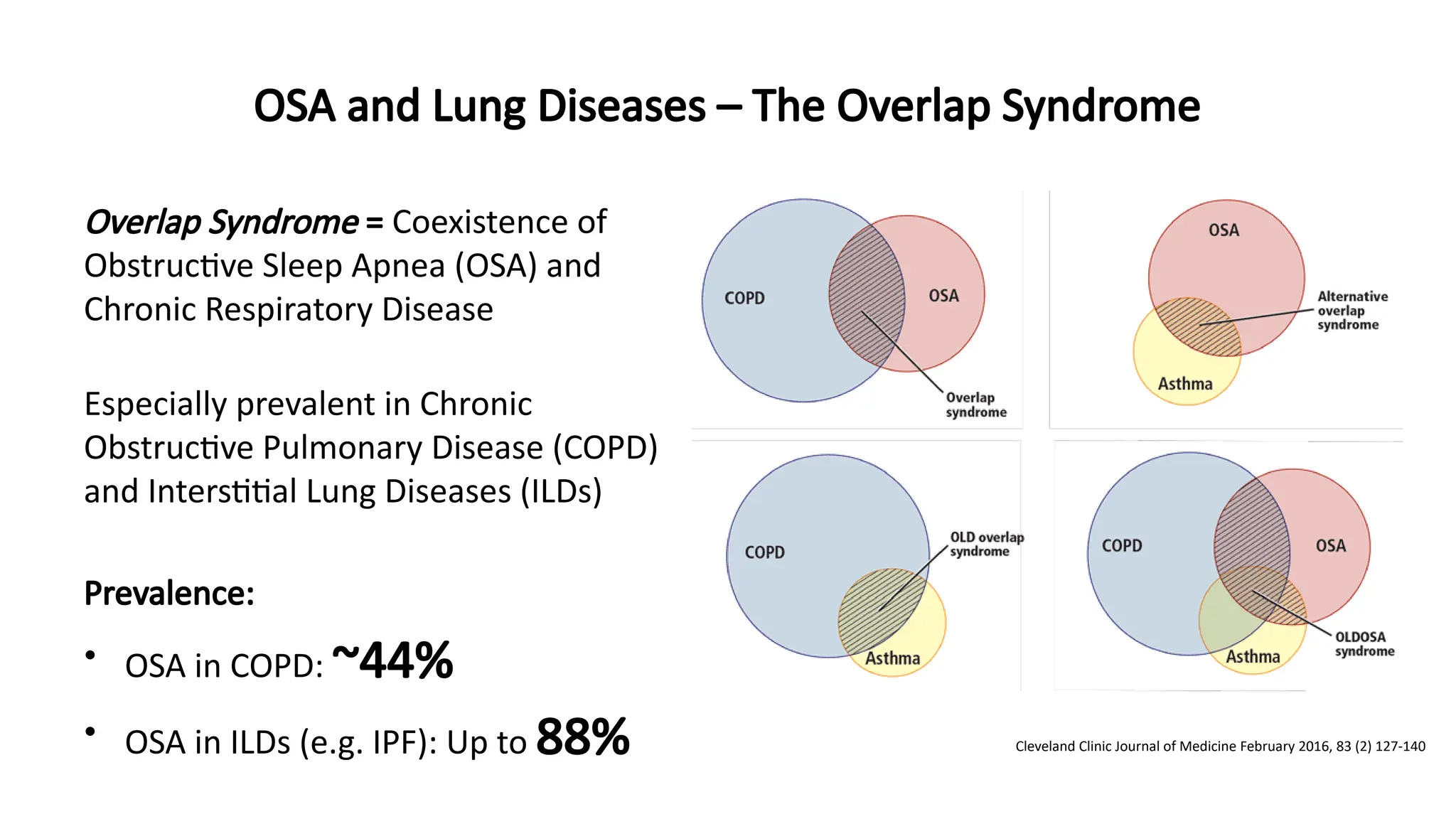
Overlap Syndrome = Coexistence of
Obstructive Sleep Apnea (OSA) and
Chronic Respiratory Disease
Especially prevalent in Chronic
Obstructive Pulmonary Disease (COPD)
and Interstitial Lung Diseases (ILDs)
Prevalence:
• OSA in COPD: ~44%
• OSA in ILDs (e.g. IPF): Up to 88% Cleveland Clinic Journal of Medicine February 2016, 83 (2) 127-140
10.
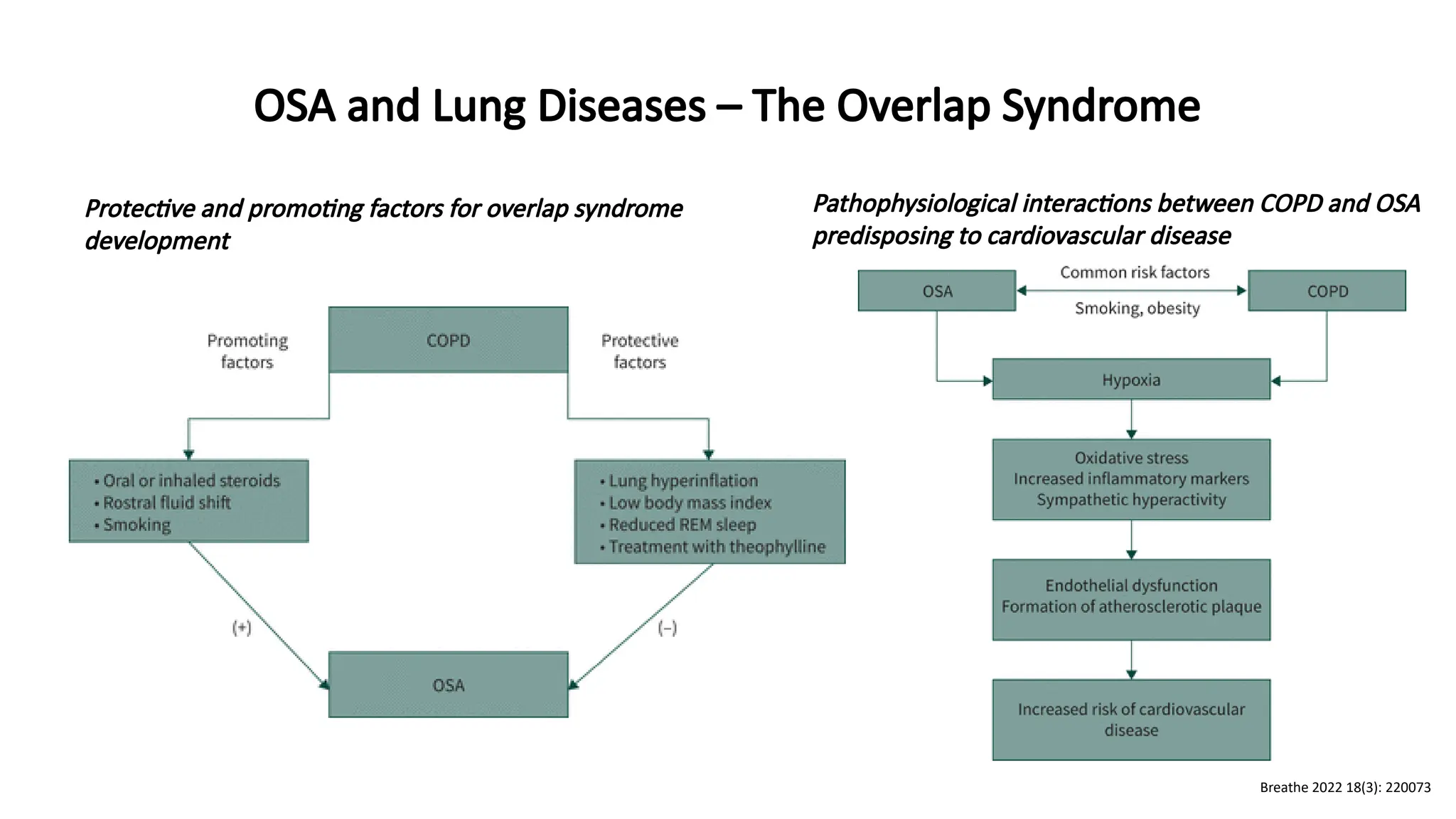
Protective and promotingfactors for overlap syndrome
development
Pathophysiological interactions between COPD and OSA
predisposing to cardiovascular disease
OSA and Lung Diseases – The Overlap Syndrome
Breathe 2022 18(3): 220073
11.
OSA and LungDiseases – The Overlap Syndrome
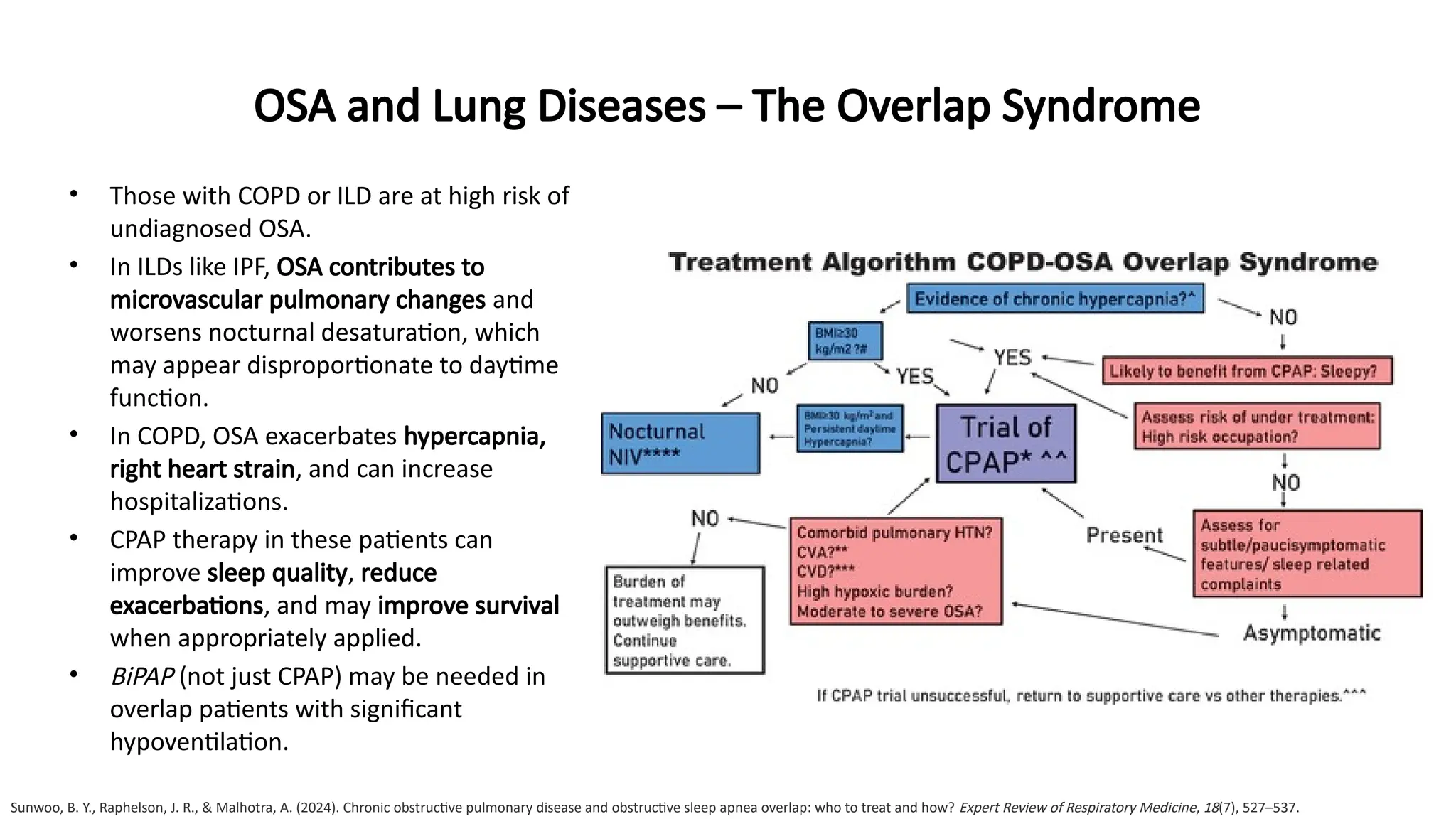
• Those with COPD or ILD are at high risk of
undiagnosed OSA.
• In ILDs like IPF, OSA contributes to
microvascular pulmonary changes and
worsens nocturnal desaturation, which
may appear disproportionate to daytime
function.
• In COPD, OSA exacerbates hypercapnia,
right heart strain, and can increase
hospitalizations.
• CPAP therapy in these patients can
improve sleep quality, reduce
exacerbations, and may improve survival
when appropriately applied.
• BiPAP (not just CPAP) may be needed in
overlap patients with significant
hypoventilation.
Sunwoo, B. Y., Raphelson, J. R., & Malhotra, A. (2024). Chronic obstructive pulmonary disease and obstructive sleep apnea overlap: who to treat and how? Expert Review of Respiratory Medicine, 18(7), 527–537.
12.
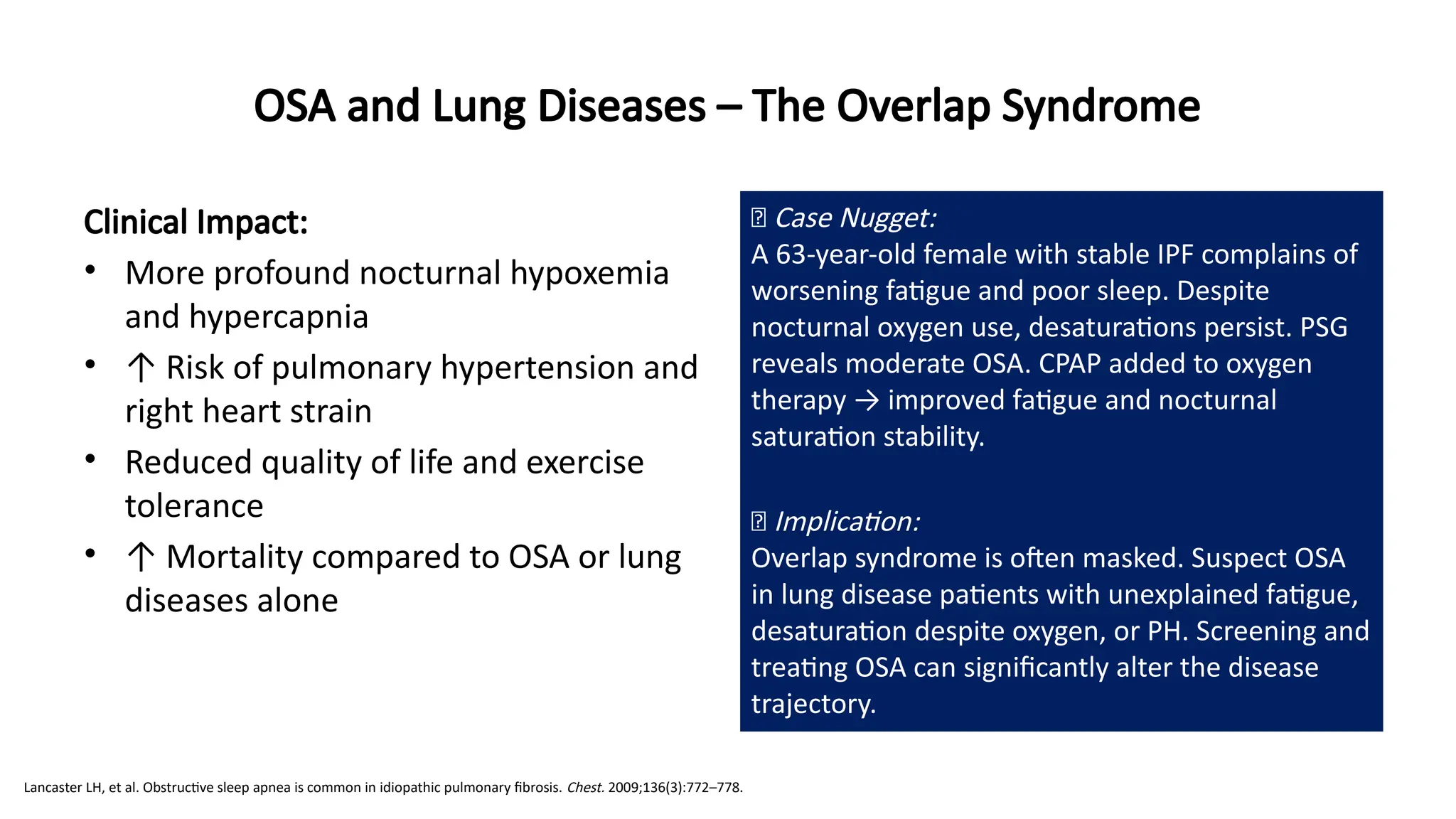
Clinical Impact:
• Moreprofound nocturnal hypoxemia
and hypercapnia
• ↑ Risk of pulmonary hypertension and
right heart strain
• Reduced quality of life and exercise
tolerance
• ↑ Mortality compared to OSA or lung
diseases alone
OSA and Lung Diseases – The Overlap Syndrome
🧠 Case Nugget:
A 63-year-old female with stable IPF complains of
worsening fatigue and poor sleep. Despite
nocturnal oxygen use, desaturations persist. PSG
reveals moderate OSA. CPAP added to oxygen
therapy → improved fatigue and nocturnal
saturation stability.
💡 Implication:
Overlap syndrome is often masked. Suspect OSA
in lung disease patients with unexplained fatigue,
desaturation despite oxygen, or PH. Screening and
treating OSA can significantly alter the disease
trajectory.
Lancaster LH, et al. Obstructive sleep apnea is common in idiopathic pulmonary fibrosis. Chest. 2009;136(3):772–778.
13.
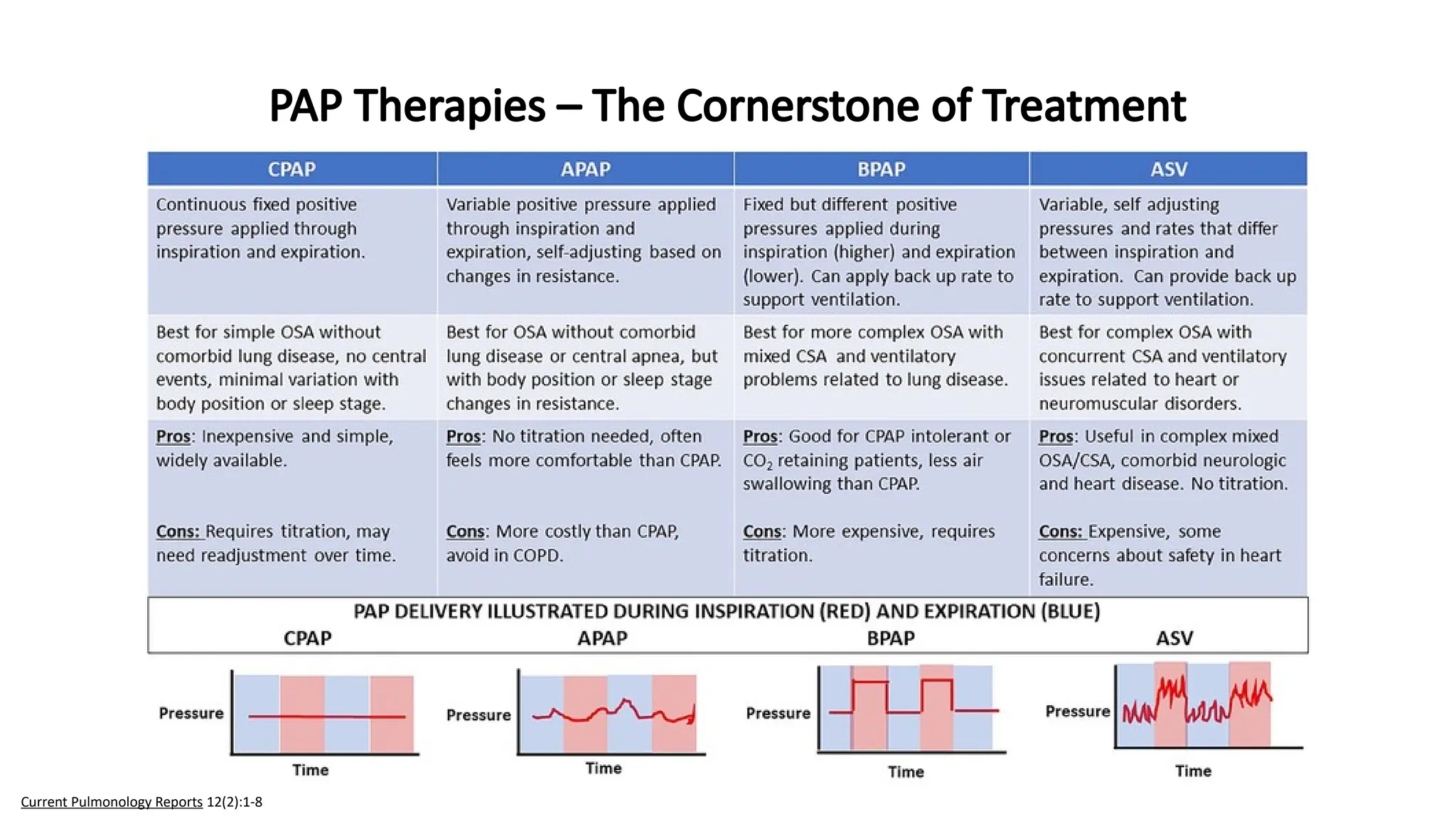
PAP Therapies –The Cornerstone of Treatment
Current Pulmonology Reports 12(2):1-8
14.
• Pulmonologists mustbe active participants in
selecting, titrating, and troubleshooting PAP therapy.
• CPAP is not one-size-fits-all and early discomfort or
nonadherence often stems from poor device or mask
matching.
• APAP is ideal for patients with positional or REM-
predominant OSA.
• BiPAP is underused in overlap syndrome, particularly
useful for those with CO₂ retention or restrictive lung
disease.
• ASV has been a game-changer for central apnea, yet
contraindicated in HFrEF patients post SERVE-HF trial.
PAP Therapies – The Cornerstone of Treatment
🧠 Case Nugget:
A 52-year-old male with AHI 39/hr and poor sleep
compliance is intolerant to CPAP due to pressure
intolerance. Shifted to APAP with ramp features →
improved comfort and >6 hrs/night use. Daytime
fatigue resolved
💡 Implication:
PAP type selection should be tailored. Early mask
fitting and titration strategy directly influence
long-term adherence.
Current Pulmonology Reports 12(2):1-8
15.
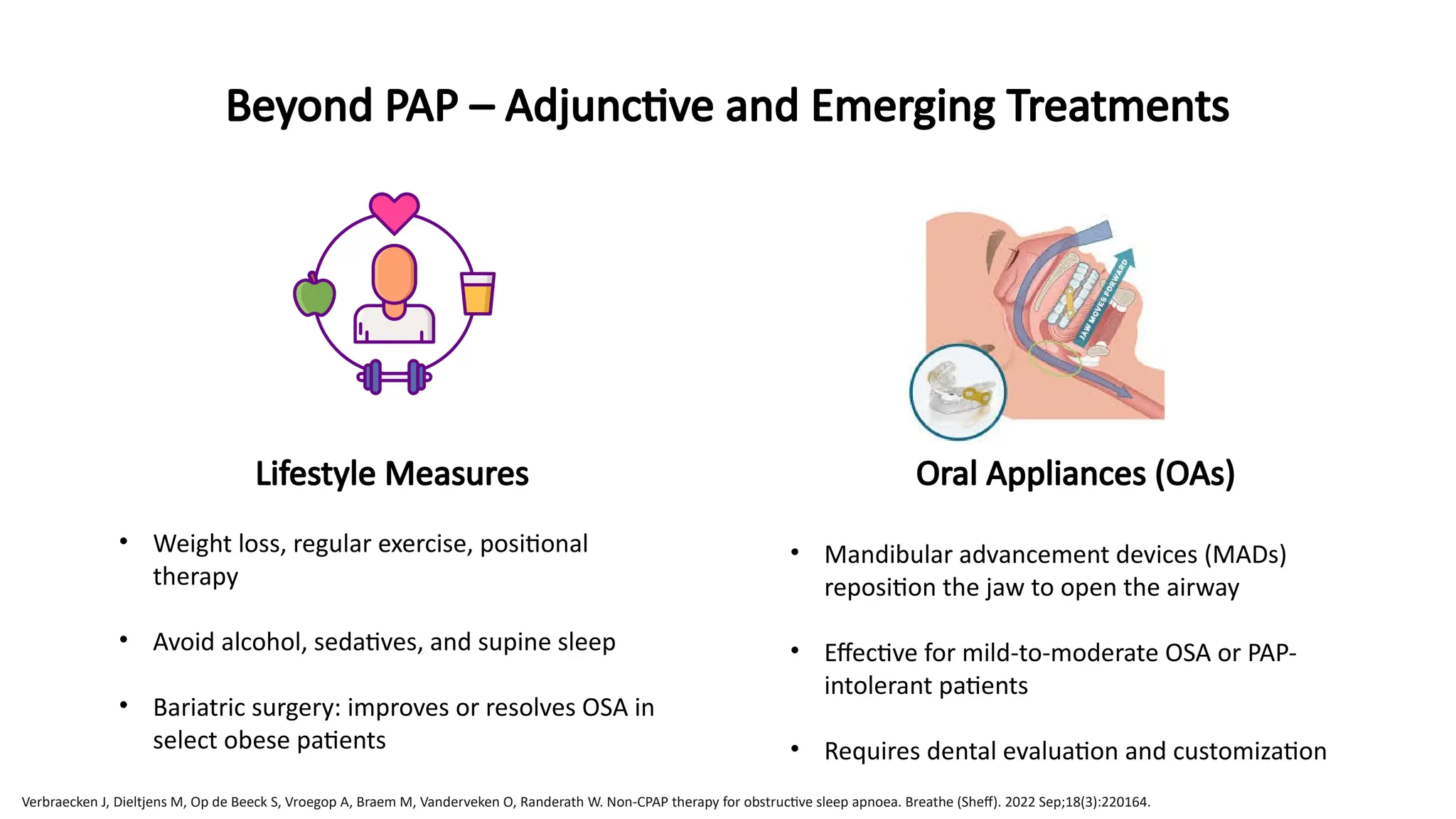
Lifestyle Measures
• Weightloss, regular exercise, positional
therapy
• Avoid alcohol, sedatives, and supine sleep
• Bariatric surgery: improves or resolves OSA in
select obese patients
Oral Appliances (OAs)
• Mandibular advancement devices (MADs)
reposition the jaw to open the airway
• Effective for mild-to-moderate OSA or PAP-
intolerant patients
• Requires dental evaluation and customization
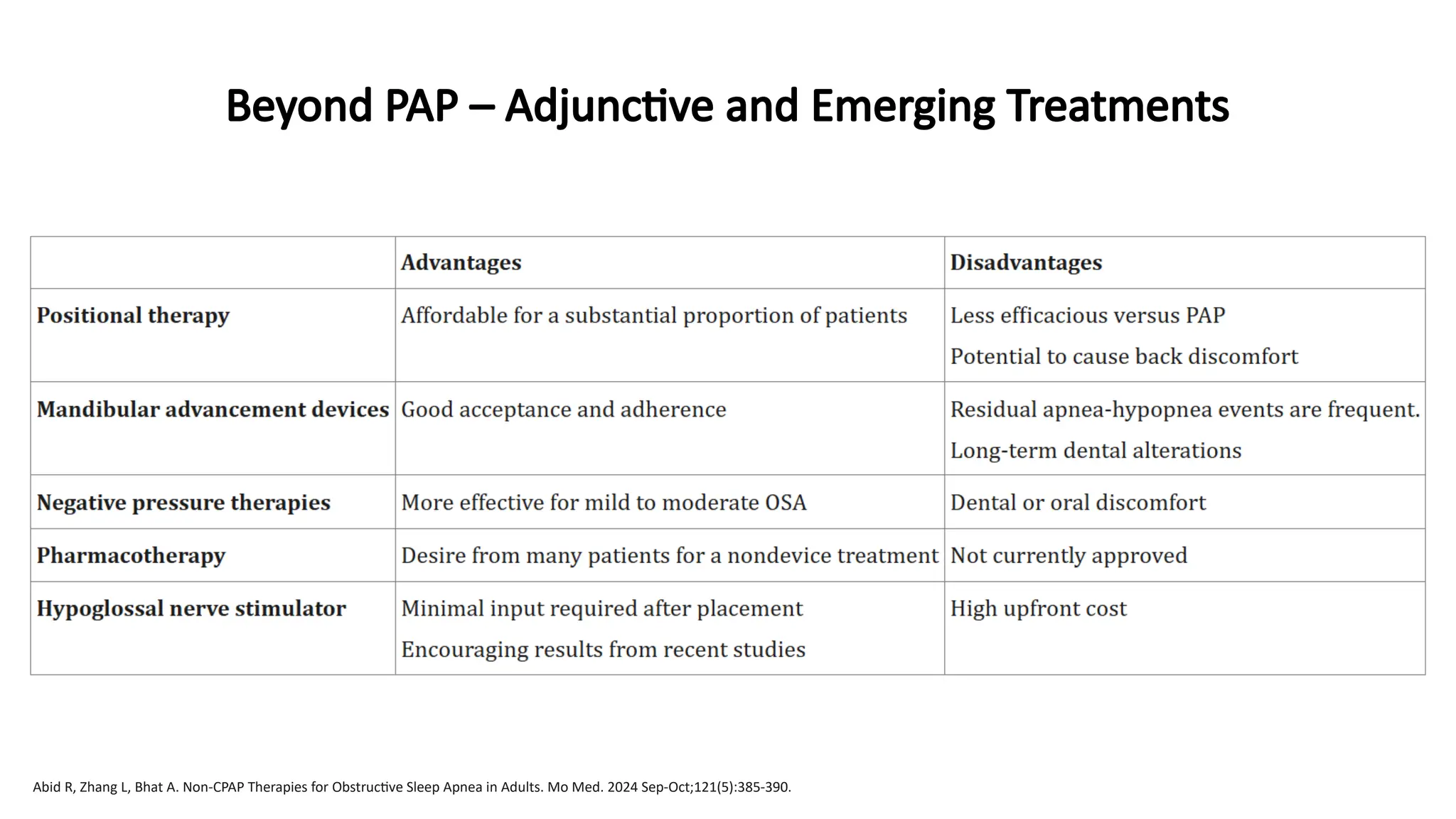
Beyond PAP – Adjunctive and Emerging Treatments
Verbraecken J, Dieltjens M, Op de Beeck S, Vroegop A, Braem M, Vanderveken O, Randerath W. Non-CPAP therapy for obstructive sleep apnoea. Breathe (Sheff). 2022 Sep;18(3):220164.
16.
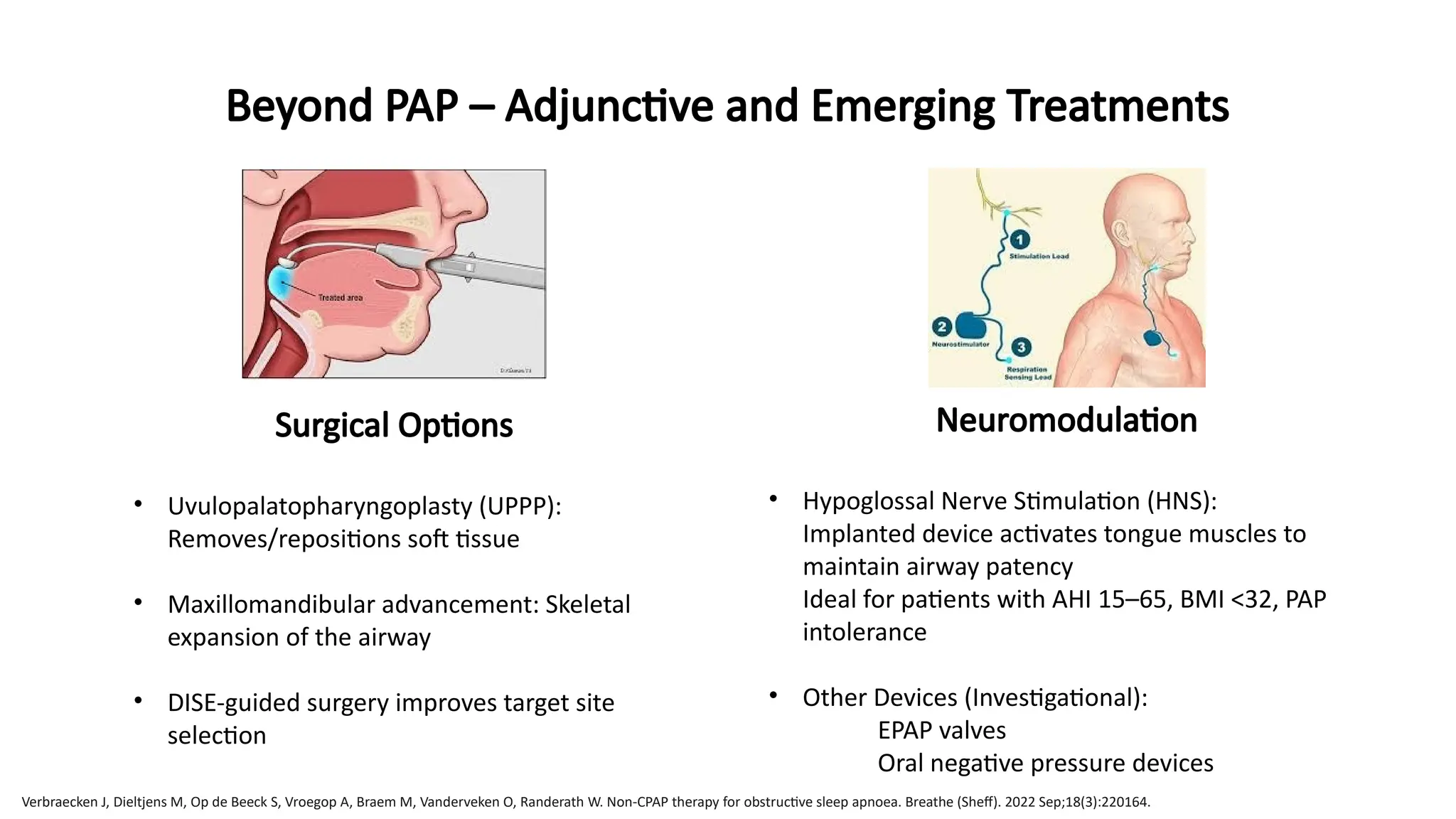
Surgical Options
• Uvulopalatopharyngoplasty(UPPP):
Removes/repositions soft tissue
• Maxillomandibular advancement: Skeletal
expansion of the airway
• DISE-guided surgery improves target site
selection
Beyond PAP – Adjunctive and Emerging Treatments
Neuromodulation
• Hypoglossal Nerve Stimulation (HNS):
Implanted device activates tongue muscles to
maintain airway patency
Ideal for patients with AHI 15–65, BMI <32, PAP
intolerance
• Other Devices (Investigational):
EPAP valves
Oral negative pressure devices
Verbraecken J, Dieltjens M, Op de Beeck S, Vroegop A, Braem M, Vanderveken O, Randerath W. Non-CPAP therapy for obstructive sleep apnoea. Breathe (Sheff). 2022 Sep;18(3):220164.
17.
Beyond PAP –Adjunctive and Emerging Treatments
Abid R, Zhang L, Bhat A. Non-CPAP Therapies for Obstructive Sleep Apnea in Adults. Mo Med. 2024 Sep-Oct;121(5):385-390.
18.
Beyond PAP –Adjunctive and Emerging Treatments
• It is essential to break the misconception that CPAP or
nothing is the treatment paradigm.
• Many patients, especially those with mild-to-moderate OSA,
anatomical variation, or CPAP intolerance benefit from
alternatives.
• MADs have strong evidence and high patient satisfaction
when fitted properly.
• HNS (Inspire device) offers a non-CPAP, non-surgical solution
with growing evidence from randomized trials (STAR trial).
• Bariatric surgery is effective not just for OSA severity but also
for reversing related comorbidities, though relapse is
possible if weight returns.
• Positional therapy (e.g. lateral sleep training) is effective in
positional OSA (supine AHI > 2× non-supine AHI).
• Encourage you to adopt a multi-modal, shared decision-
making approach tailored to patient phenotype and
preferences.
🧠 Case Nugget:
A 48-year-old woman with BMI 27 and mild OSA
(AHI 11/hr) is unable to tolerate CPAP. Fitted with
a custom MAD → 70% reduction in AHI, improved
sleep, no desaturation events on repeat HSAT.
💡 Implication:
Not all OSA needs CPAP. Patient-centric treatment
pathways—especially in mild cases—can improve
adherence and outcomes.
Breathe 2022 18(3): 220164
19.
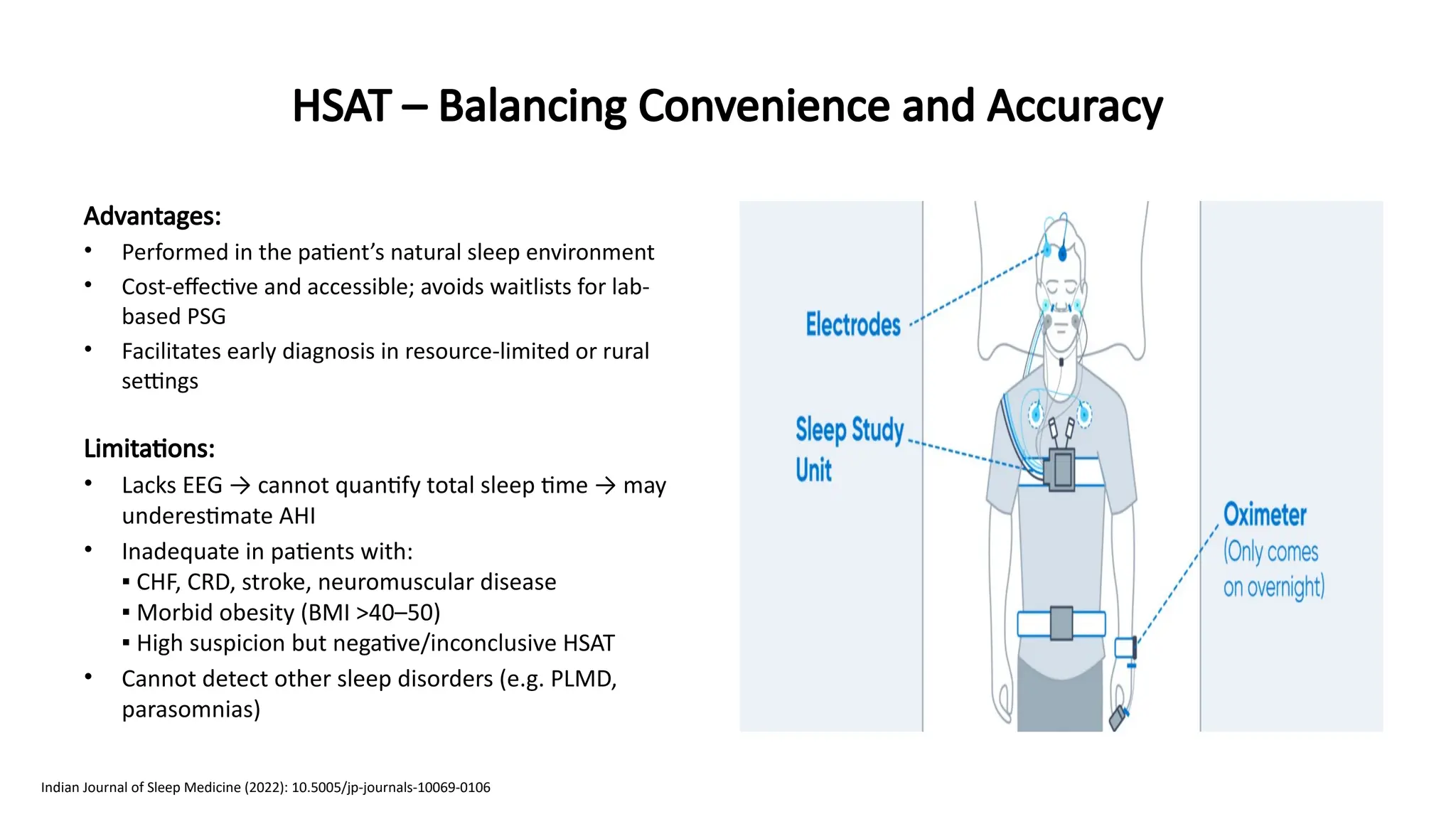
Advantages:
• Performed inthe patient’s natural sleep environment
• Cost-effective and accessible; avoids waitlists for lab-
based PSG
• Facilitates early diagnosis in resource-limited or rural
settings
Limitations:
• Lacks EEG → cannot quantify total sleep time → may
underestimate AHI
• Inadequate in patients with:
▪ CHF, CRD, stroke, neuromuscular disease
▪ Morbid obesity (BMI >40–50)
▪ High suspicion but negative/inconclusive HSAT
• Cannot detect other sleep disorders (e.g. PLMD,
parasomnias)
HSAT – Balancing Convenience and Accuracy
Indian Journal of Sleep Medicine (2022): 10.5005/jp-journals-10069-0106
20.
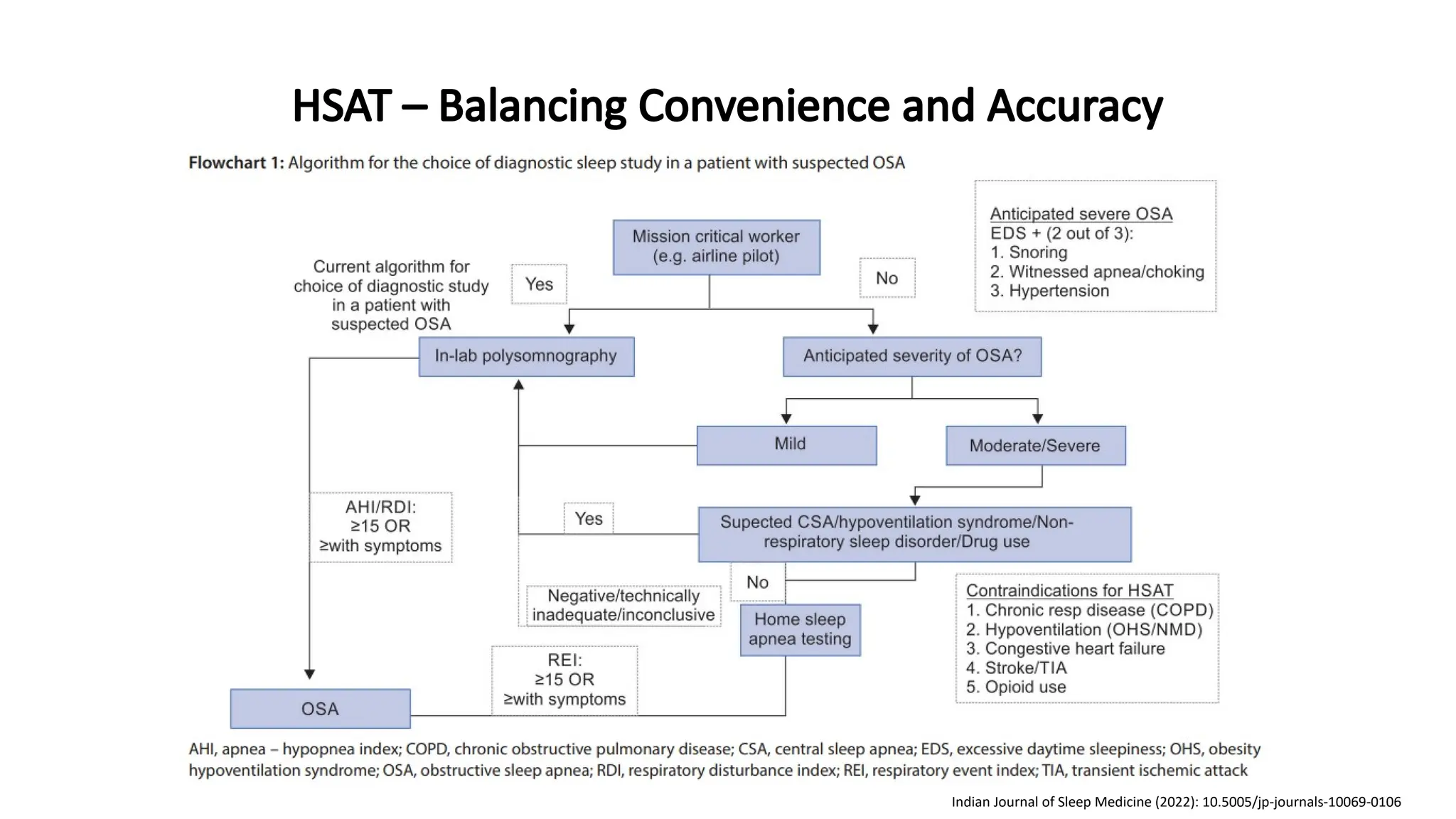
HSAT – BalancingConvenience and Accuracy
Indian Journal of Sleep Medicine (2022): 10.5005/jp-journals-10069-0106
21.
HSAT – BalancingConvenience and Accuracy
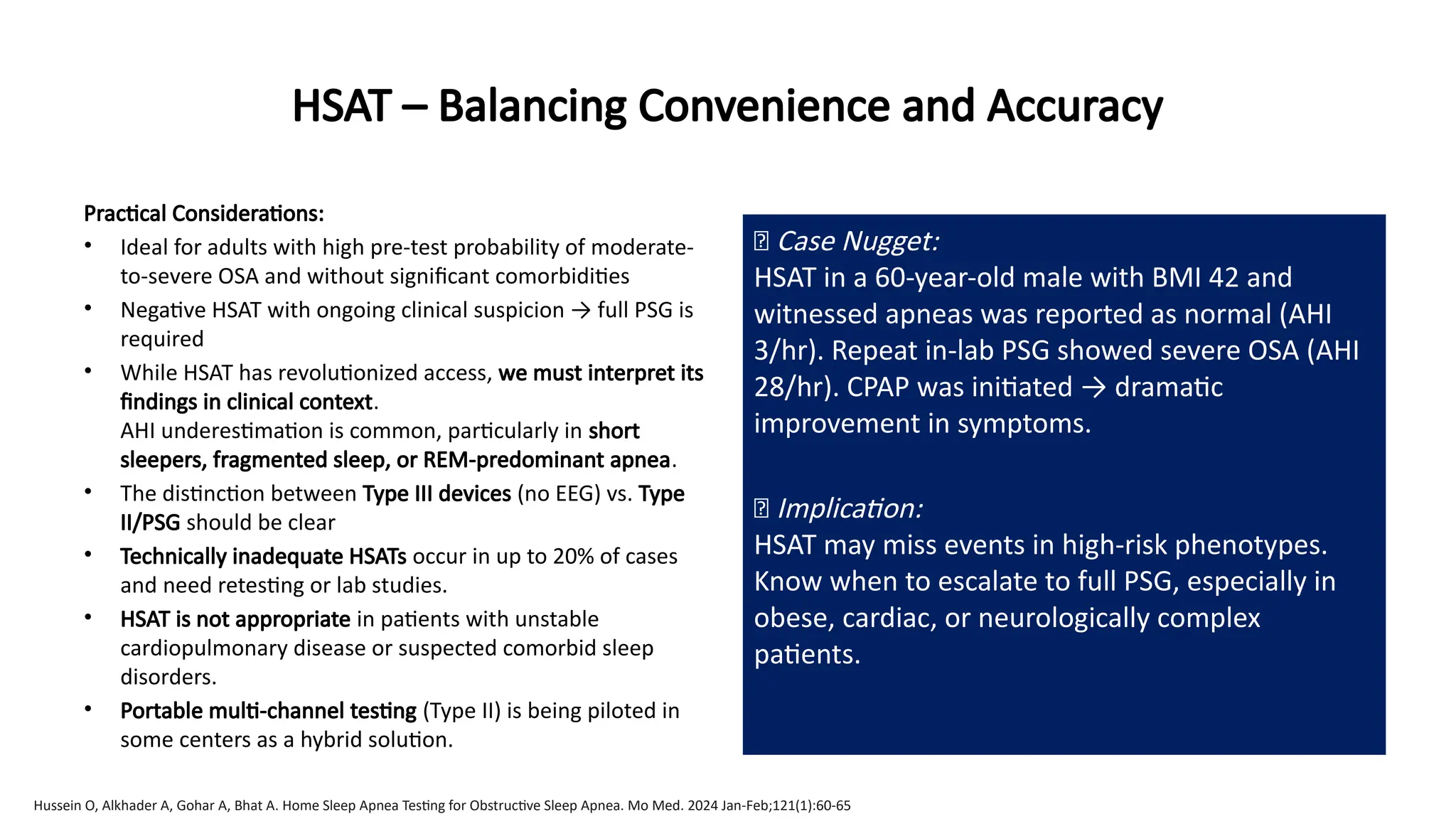
Practical Considerations:
• Ideal for adults with high pre-test probability of moderate-
to-severe OSA and without significant comorbidities
• Negative HSAT with ongoing clinical suspicion → full PSG is
required
• While HSAT has revolutionized access, we must interpret its
findings in clinical context.
AHI underestimation is common, particularly in short
sleepers, fragmented sleep, or REM-predominant apnea.
• The distinction between Type III devices (no EEG) vs. Type
II/PSG should be clear
• Technically inadequate HSATs occur in up to 20% of cases
and need retesting or lab studies.
• HSAT is not appropriate in patients with unstable
cardiopulmonary disease or suspected comorbid sleep
disorders.
• Portable multi-channel testing (Type II) is being piloted in
some centers as a hybrid solution.
🧠 Case Nugget:
HSAT in a 60-year-old male with BMI 42 and
witnessed apneas was reported as normal (AHI
3/hr). Repeat in-lab PSG showed severe OSA (AHI
28/hr). CPAP was initiated → dramatic
improvement in symptoms.
💡 Implication:
HSAT may miss events in high-risk phenotypes.
Know when to escalate to full PSG, especially in
obese, cardiac, or neurologically complex
patients.
Hussein O, Alkhader A, Gohar A, Bhat A. Home Sleep Apnea Testing for Obstructive Sleep Apnea. Mo Med. 2024 Jan-Feb;121(1):60-65
22.
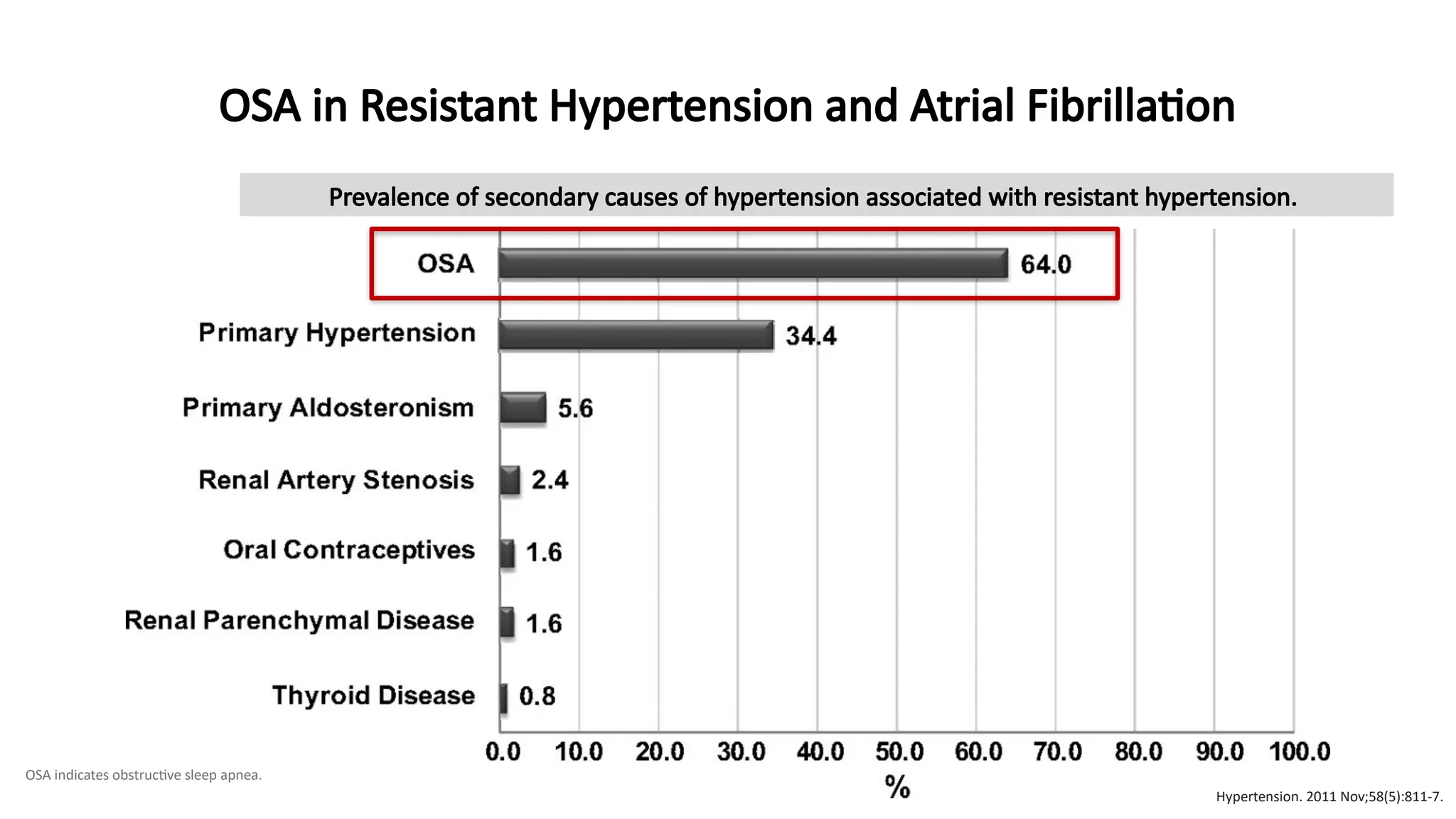
Prevalence of secondarycauses of hypertension associated with resistant hypertension.
OSA indicates obstructive sleep apnea.
OSA in Resistant Hypertension and Atrial Fibrillation
Hypertension. 2011 Nov;58(5):811-7.
23.
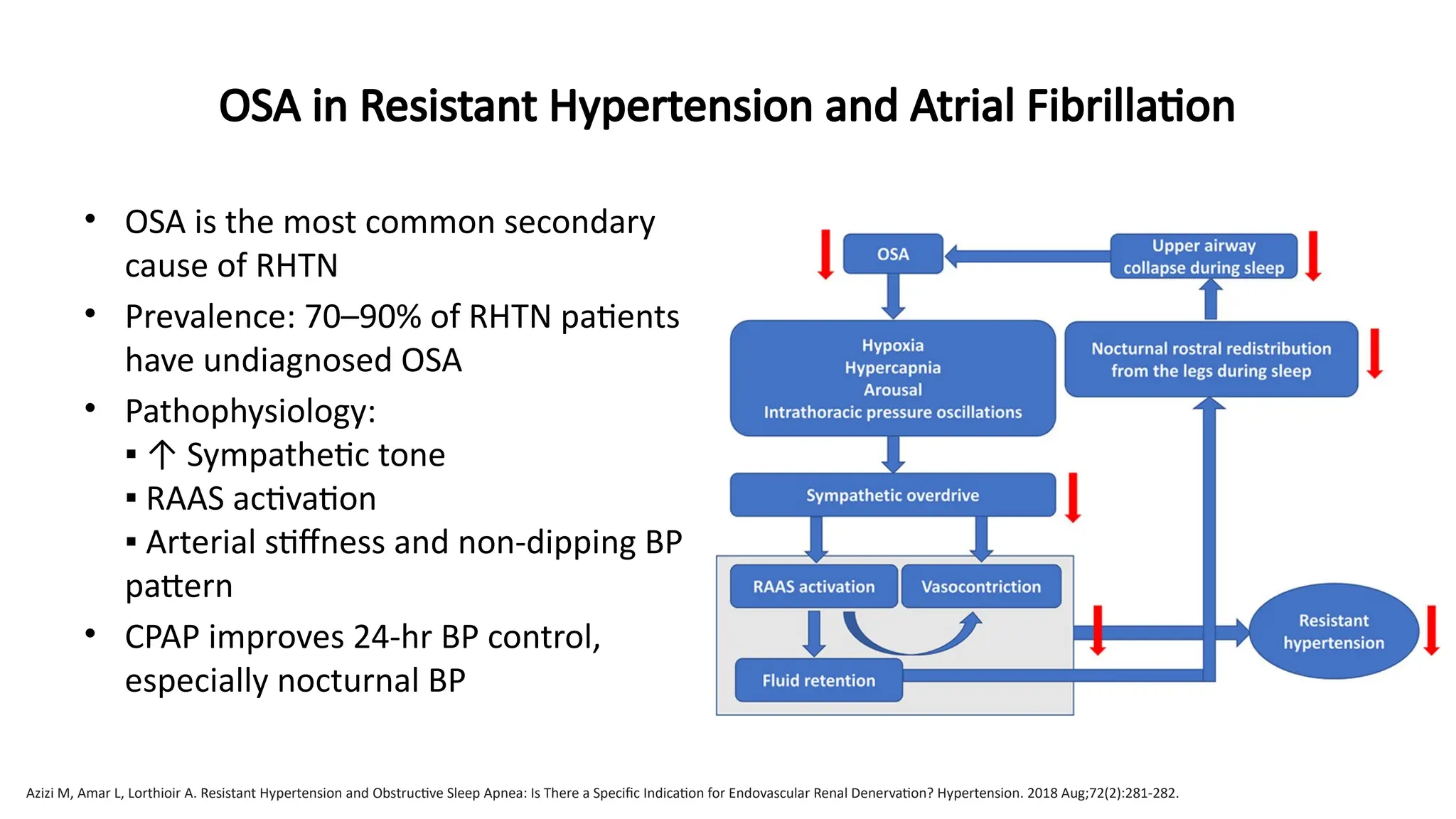
• OSA isthe most common secondary
cause of RHTN
• Prevalence: 70–90% of RHTN patients
have undiagnosed OSA
• Pathophysiology:
▪ ↑ Sympathetic tone
▪ RAAS activation
▪ Arterial stiffness and non-dipping BP
pattern
• CPAP improves 24-hr BP control,
especially nocturnal BP
Azizi M, Amar L, Lorthioir A. Resistant Hypertension and Obstructive Sleep Apnea: Is There a Specific Indication for Endovascular Renal Denervation? Hypertension. 2018 Aug;72(2):281-282.
OSA in Resistant Hypertension and Atrial Fibrillation
24.
OSA in ResistantHypertension and Atrial Fibrillation
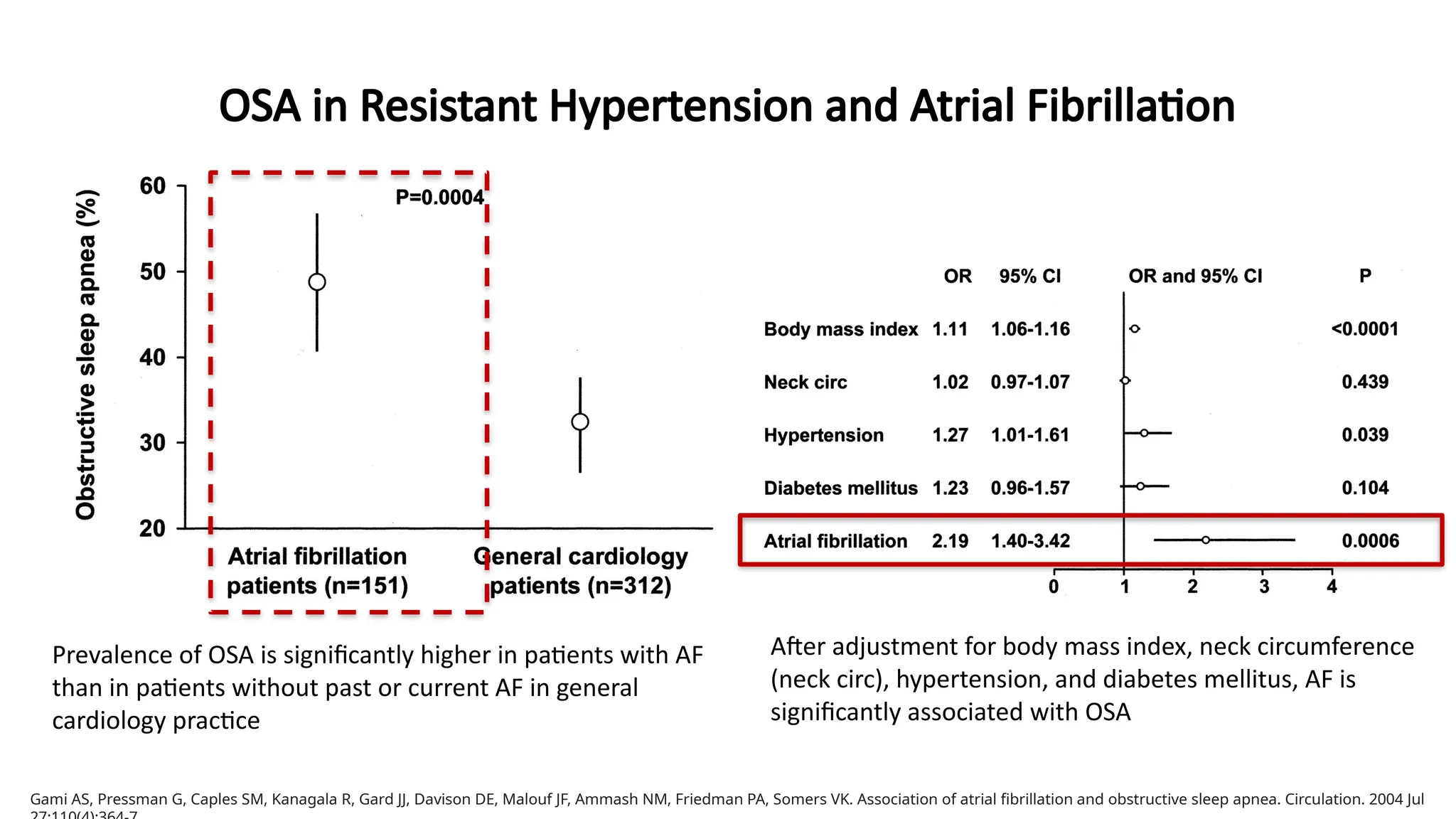
After adjustment for body mass index, neck circumference
(neck circ), hypertension, and diabetes mellitus, AF is
significantly associated with OSA
Prevalence of OSA is significantly higher in patients with AF
than in patients without past or current AF in general
cardiology practice
Gami AS, Pressman G, Caples SM, Kanagala R, Gard JJ, Davison DE, Malouf JF, Ammash NM, Friedman PA, Somers VK. Association of atrial fibrillation and obstructive sleep apnea. Circulation. 2004 Jul
25.
OSA in ResistantHypertension and Atrial Fibrillation
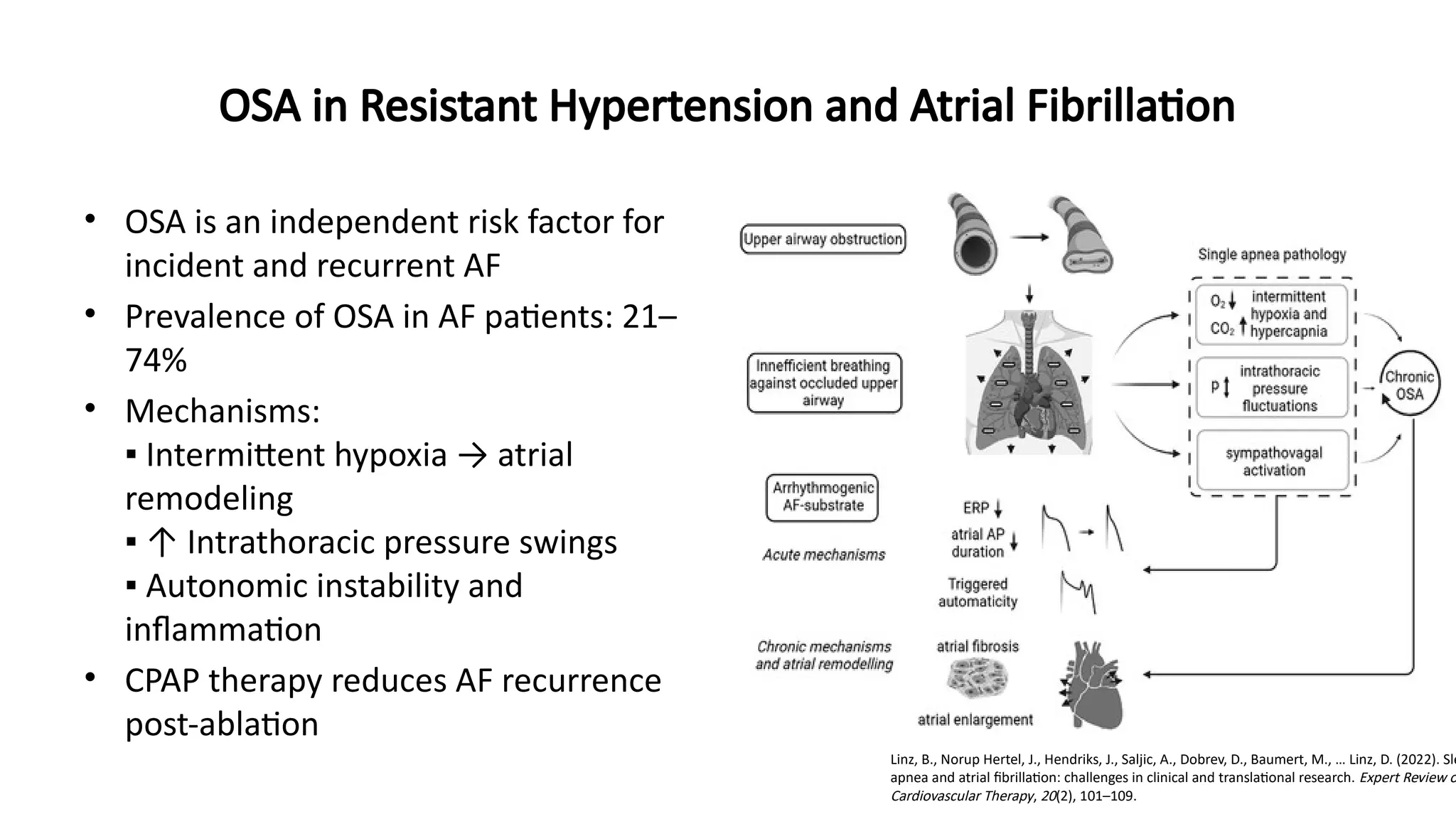
• OSA is an independent risk factor for
incident and recurrent AF
• Prevalence of OSA in AF patients: 21–
74%
• Mechanisms:
▪ Intermittent hypoxia → atrial
remodeling
▪ ↑ Intrathoracic pressure swings
▪ Autonomic instability and
inflammation
• CPAP therapy reduces AF recurrence
post-ablation
Linz, B., Norup Hertel, J., Hendriks, J., Saljic, A., Dobrev, D., Baumert, M., … Linz, D. (2022). Sle
apnea and atrial fibrillation: challenges in clinical and translational research. Expert Review o
Cardiovascular Therapy, 20(2), 101–109.
26.
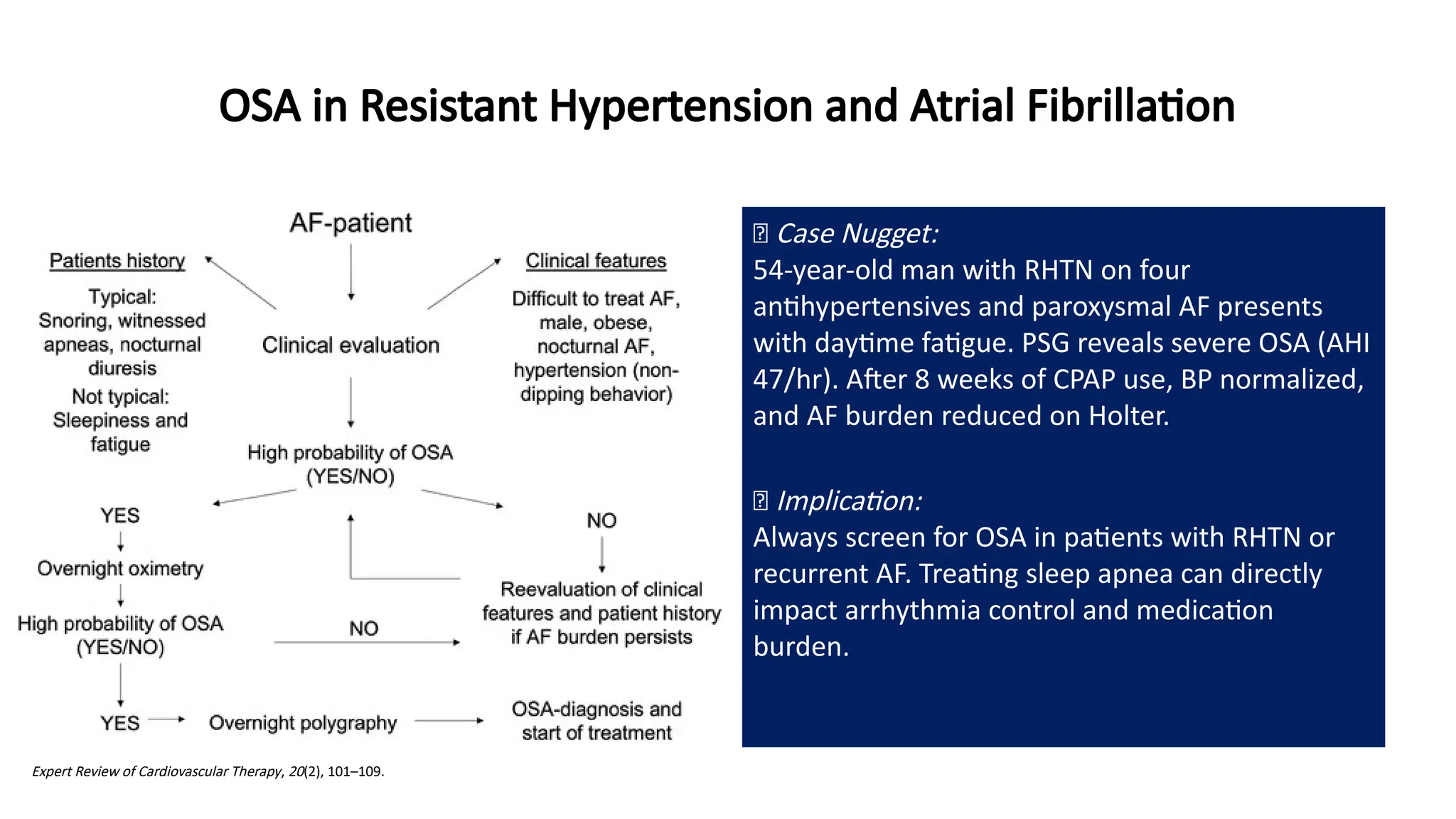
🧠 Case Nugget:
54-year-oldman with RHTN on four
antihypertensives and paroxysmal AF presents
with daytime fatigue. PSG reveals severe OSA (AHI
47/hr). After 8 weeks of CPAP use, BP normalized,
and AF burden reduced on Holter.
💡 Implication:
Always screen for OSA in patients with RHTN or
recurrent AF. Treating sleep apnea can directly
impact arrhythmia control and medication
burden.
Expert Review of Cardiovascular Therapy, 20(2), 101–109.
OSA in Resistant Hypertension and Atrial Fibrillation
27.
Conclusion – TowardsHolistic Sleep Apnea Management
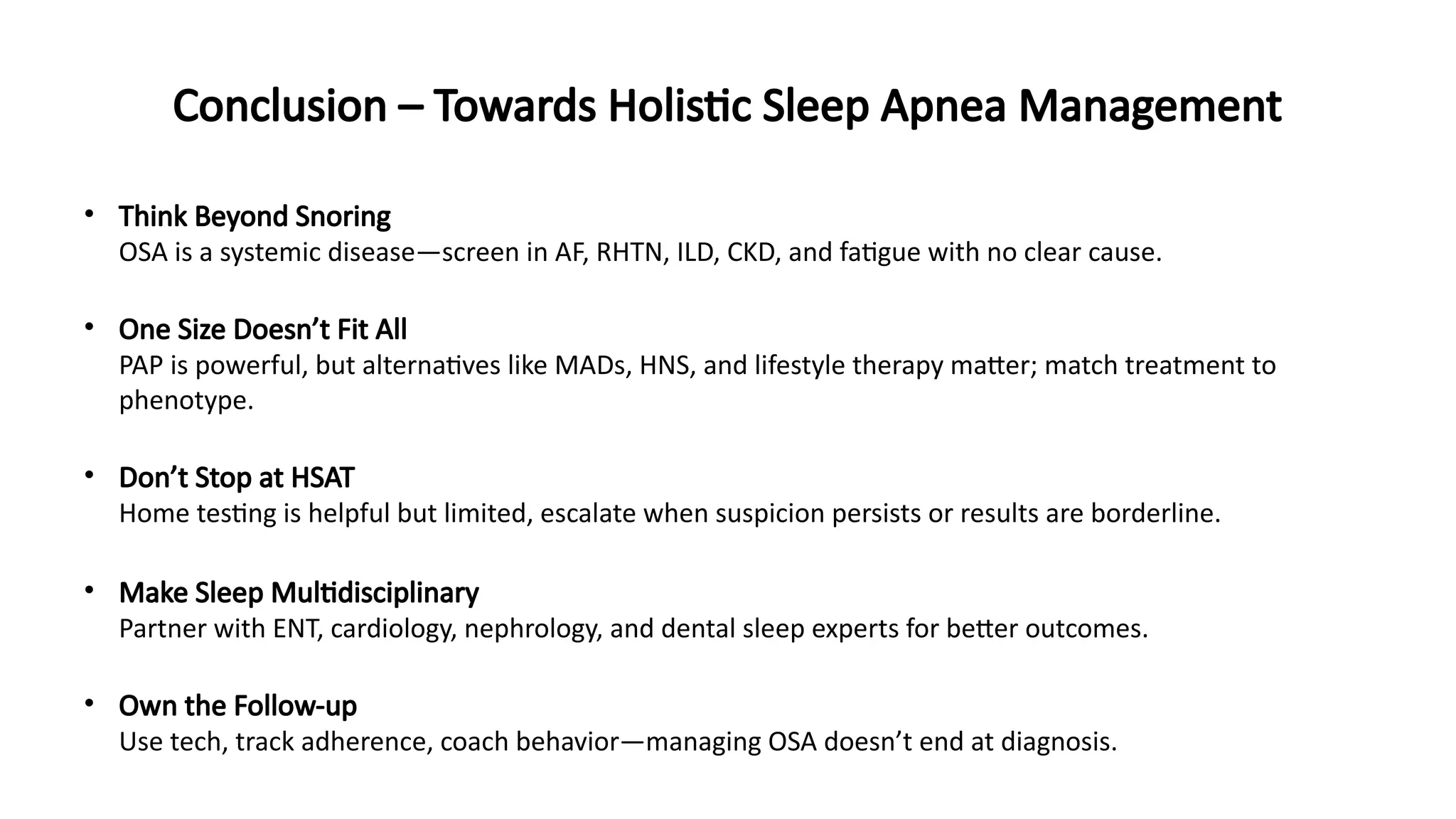
• Think Beyond Snoring
OSA is a systemic disease—screen in AF, RHTN, ILD, CKD, and fatigue with no clear cause.
• One Size Doesn’t Fit All
PAP is powerful, but alternatives like MADs, HNS, and lifestyle therapy matter; match treatment to
phenotype.
• Don’t Stop at HSAT
Home testing is helpful but limited, escalate when suspicion persists or results are borderline.
• Make Sleep Multidisciplinary
Partner with ENT, cardiology, nephrology, and dental sleep experts for better outcomes.
• Own the Follow-up
Use tech, track adherence, coach behavior—managing OSA doesn’t end at diagnosis.
#2 Emphasize that OSA is not just a sleep disorder but a systemic condition. Undiagnosed OSA is common even in tertiary care. This is especially true in women, elderly patients, and those with obesity or multiple comorbidities. OSA should be considered in patients with metabolic syndrome, unexplained fatigue, or treatment-resistant hypertension.
#3 OSA contributes to cardiovascular morbidity through a cascade of sympathetic activation, vascular remodeling, and systemic inflammation. Even after adjusting for BMI and age, the risk remains elevated. The Sleep Heart Health Study and Wisconsin Cohort support this.
#4 OSA contributes to cardiovascular morbidity through a cascade of sympathetic activation, vascular remodeling, and systemic inflammation. Even after adjusting for BMI and age, the risk remains elevated. The Sleep Heart Health Study and Wisconsin Cohort support this.
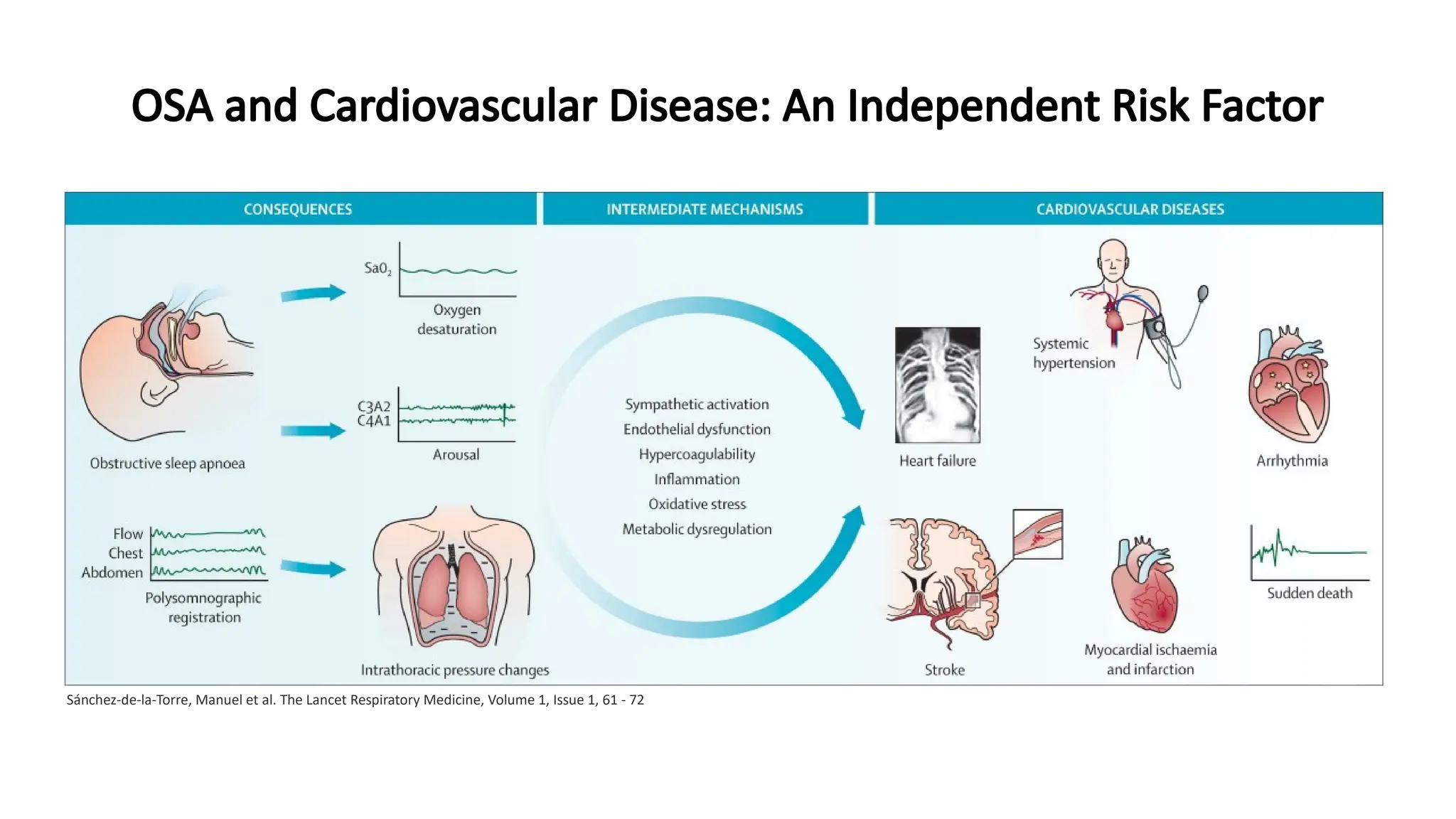
#5 We start on the left with classic features of OSA:
Obstructive episodes during sleep cause intermittent oxygen desaturation (seen in the SaO₂ graph),
Along with cortical arousals that fragment sleep, and
Intrathoracic pressure changes due to effort against a closed airway—picked up on polysomnography (flow, chest, abdomen tracings).
These lead to chronic activation of harmful physiological pathways (center column):
Sympathetic overactivity — persistent catecholamine surges raise blood pressure and heart rate.
Endothelial dysfunction — promotes atherogenesis.
Inflammation and oxidative stress — fuel cardiovascular remodeling.
Metabolic dysregulation and hypercoagulability — increase the risk of thrombotic events.
Moving to the right side, the end-organ consequences include:
Systemic hypertension — often nocturnal and non-dipping,
Arrhythmias, especially atrial fibrillation and ventricular ectopy,
Heart failure — especially right heart strain in overlap syndromes,
Stroke and myocardial infarction, and in severe cases,
Sudden cardiac death, particularly during REM sleep when OSA is most pronounced.
You may want to emphasize that these mechanisms operate silently and chronically, often in patients who don’t meet the “classic” OSA phenotype.
🩺 Clinical Reinforcement:
This pathophysiology underscores why OSA should be suspected in patients with:
Resistant hypertension,
Recurrent AF post-ablation,
Nocturnal angina or cardiac events,
Unexplained fatigue or cognitive decline.
#7 Pulmonologists must consider renal implications of untreated OSA. CKD patients often attribute fatigue to uremia. However, sleep apnea frequently coexists and exacerbates renal hypoxia and blood pressure variability.
#9 This is a critical pulmonology slide. Many CRD patients are never evaluated for OSA despite significant overlap. Overlap syndrome leads to higher cardiovascular and respiratory mortality. BiPAP may be preferred in cases with hypercapnia.
#10 This slide addresses the complex interplay between COPD and OSA, a combination known as Overlap Syndrome, which significantly worsens patient outcomes—especially cardiovascular risk.
🔹 On the left, we see factors that influence overlap development:
Promoting factors:
▪ Use of steroids (oral/inhaled)
▪ Rostral fluid shift during sleep
▪ Smoking — a shared risk for both diseases
Protective factors:
▪ Lung hyperinflation (mechanical splinting effect)
▪ Lower BMI
▪ Reduced REM sleep
▪ Theophylline therapy (stimulates respiration)
This illustrates why not all COPD patients develop OSA, and vice versa.
🔹 On the right, we zoom into the shared pathophysiological pathway that makes this overlap so dangerous:
OSA and COPD share common risk factors: obesity and smoking.
Both contribute to chronic hypoxia, which triggers:
▪ Oxidative stress
▪ Increased inflammatory mediators
▪ Sympathetic overactivation
These feed into endothelial dysfunction and plaque formation, ultimately increasing the risk of cardiovascular disease.
🩺 Clinical Takeaway:
Patients with overlap syndrome have more severe nocturnal desaturation and are at higher risk for pulmonary hypertension, right heart failure, and sudden cardiac events. Screen aggressively and consider BiPAP or nocturnal oxygen + CPAP strategies for management.
#13 This slide compares the four major types of Positive Airway Pressure (PAP) therapies, each tailored to different OSA phenotypes and comorbidities.
CPAP is the first-line therapy for uncomplicated OSA. It's simple, inexpensive, but often poorly tolerated due to fixed pressure.
APAP adjusts pressure based on resistance—ideal for patients with positional or REM-related OSA and those who can't tolerate fixed CPAP.
BiPAP delivers higher inspiratory pressure—especially useful in CO₂ retainers, neuromuscular weakness, or overlap syndrome.
ASV is reserved for complex cases (e.g., central apneas or Cheyne–Stokes in CHF), but should be avoided in HFrEF with low EF.
Tip: Focus on comfort, comorbidities, and pressure needs when deciding. Patient education and early follow-up are critical for long-term adherence.
#20 This algorithm helps determine when to use in-lab polysomnography (PSG) versus home sleep apnea testing (HSAT).
🔹 Start with risk stratification:
If the patient is a mission-critical worker (e.g., airline pilot), or has suspected central sleep apnea (CSA) or hypoventilation, they must go for full in-lab PSG—no shortcuts.
🔹 For typical OSA:
If symptoms suggest moderate to severe OSA (EDS + ≥2: snoring, witnessed apneas, hypertension), in-lab PSG is preferred.
If mild OSA is suspected and there are no red flags, HSAT is acceptable.
🔹 Avoid HSAT in patients with:
COPD or other chronic respiratory diseases
Hypoventilation syndromes (OHS, neuromuscular)
CHF
Stroke or TIA
Opioid use
🔹 If HSAT is inconclusive, move to in-lab PSG.
#22 This chart drives home a critical clinical point:
Obstructive Sleep Apnea (OSA) is the most common secondary cause of resistant hypertension, present in 64% of such cases—far more than other commonly screened causes like:
Primary aldosteronism (5.6%)
Renal artery stenosis (2.4%)
Thyroid disease, oral contraceptives, renal parenchymal disease—all <2%
🔹 And yet, OSA is often the least screened in real-world practice.
🔹 In atrial fibrillation (AF), especially post-ablation, untreated OSA significantly increases the risk of recurrence.
💡 Practical Takeaway:
Any patient on ≥3 antihypertensives—including a diuretic—should be evaluated for OSA, particularly if they also report snoring or daytime fatigue.
Also, screen all AF patients for OSA pre-ablation.
This is low-hanging fruit where pulmonologists can lead cross-specialty collaboration with cardiology and internal medicine.
#23 This slide explains why OSA is the most common secondary cause of resistant hypertension (RHTN)—often missed.
🔹 Up to 90% of RHTN patients may have undiagnosed OSA.
🔹 Mechanisms include:
Recurrent hypoxia → ↑ sympathetic drive
RAAS activation → vasoconstriction + fluid retention
Non-dipping BP pattern due to disrupted sleep
🔹 Also note the contribution of nocturnal rostral fluid shift, especially in supine patients.
🔹 CPAP therapy has been shown to lower 24-hour BP—especially nocturnal values—improving cardiovascular outcomes.
💡 Reminder: Screen all patients with RHTN and AF—even if they don’t have classic OSA symptoms.
#24 This slide highlights the strong association between OSA and atrial fibrillation (AF).
In this study, OSA prevalence was significantly higher in AF patients compared to general cardiology patients (P=0.0004).
Even after adjusting for BMI, neck circumference, hypertension, and diabetes, AF independently increased the odds of having OSA (OR 2.19, P=0.0006).
🔹 In clinical practice, this means:
Any patient with AF—especially if recurrent or post-ablation—should be screened for OSA, regardless of body habitus.
#25 This schematic shows the chain reaction triggered by a single obstructive apnea event and how it promotes atrial fibrillation:
Upper airway obstruction leads to ineffective inspiratory effort against a closed airway, generating large negative intrathoracic pressures.
This causes intermittent hypoxia and hypercapnia, which activate the sympathetic nervous system and increase oxidative stress.
These fluctuations alter atrial electrophysiology—affecting ERP (effective refractory period) and action potential duration—leading to atrial fibrosis and substrate remodeling.
Over time, this repeated stress contributes to chronic atrial enlargement, setting the stage for persistent or recurrent AF.
The visual helps bridge the mechanical events of OSA with electrophysiologic remodeling, reinforcing why managing OSA can modify AF outcomes.
#26 This flowchart outlines a pragmatic approach to identifying undiagnosed OSA in patients with atrial fibrillation.
🔹 It starts with clinical suspicion—based on both patient history (like snoring or nocturnal symptoms) and clinical features (such as obesity, male gender, non-dipping hypertension, or difficult-to-control AF).
🔹 If OSA probability is high:
Overnight oximetry is used as a quick, accessible screening step.
If still suspicious, move to overnight polygraphy for confirmation.
🔹 If initial probability is low, but AF persists or escalates, a re-evaluation is recommended—this ensures we don’t miss evolving sleep-disordered breathing.
🔹 Once diagnosed, OSA treatment is initiated, ideally improving both AF control and cardiovascular outcomes.
#27 Summarize that OSA is systemic. Pulmonologists must act as coordinators, not just diagnosticians. Mention integrated care models and digital health tools as the future. Reinforce shared decision-making.