The negative impacts of adolescent sexuality problems among secondary school ...
Sexual Risk Behaviors Research
1. www.postersession.com
Table 1: Participants and Recruitment
Procedure
Focus Group
- Concurrent mixed methods were used during this procedure.
- 12 members were recruited through text message, class, and social media.
- We used a semi-structured format to conduct two focus group interviews
consisting of 6 individuals each.
- We asked questions best describing our participant’s knowledge of
STDs/STIs.
- The recording methods used were audio recordings on electronic devices
and hand typed recordings.
- All recordings were transcribed and imported into ATLAS.ti.
Survey
- Concurrent mixed methods were used during this procedure.
- We used an online questionnaire through SurveyGizmo.
- 73 participants were recruited through an electronic link via text message
and social media sites.
- 17 participants completed a hard copy questionnaire.
- The survey results were uploaded to SurveyGizmo and then transferred to
Excel.
- All results were imported into SPSS Statistics software. Quantitative Results:
Mean = 21.21
SD = 2.053
N = 90
Variables and Hypothesis
Limitations
- The number of incidents in sexually transmitted infections (STIs)
have shown a noticeable increase in young adults within the last
decade.3
- As of 2015, there were 110 million cases of STIs, with an
additional 20 million in new cases each year, and costing the
American health care system 16 billion dollars annually.3
- In the year 2014, the number of cases for chlamydia in California
were 60,034 and 114,243 for male and female, respectively.2
- In Orange County alone, rates of chlamydia, gonorrhea, and
syphilis in just the male population have increased by 34%, 65%,
and 92%, respectively.4
- According to Victor Vroom’s Expectancy Theory, expectations
conduct a person’s decisional behaviors. Thus, this theory
addresses a viable explanation between both genders and the
interpretation of sexual decisional behaviors.10
- This study aims to highlight the relationship between gender and
sexual risk behaviors to determine which gender will engage in
higher sexual risk behaviors.
- We believe that males will engage in a higher incidence of sexual
risk behaviors due to biological factors, supported by the cognitive
assumptions from the Expectancy Theory.
- Despite the findings of this research study, there are many
contributors to STIs. We believe that gender could be one of
these factors, however more research is needed to confirm. Future
health programs can be tailored if this study is found to be true.
The purpose of this study is to determine if there is an association
between gender and sexual risk behaviors.
Our hypothesis states that males will engage in higher sexual risk
behaviors than females due to higher levels of testosterone.
Independent Variable Dependent Variable
Sexual Risk Behaviors Gender
- We found no significant difference between gender and sexual risk
behaviors. However existing literature has shown other factors that
contribute to the increase in number of STIs.
- Contributing factors to high risk sexual behaviors include, but not limited
to, are condom efficacy use1
, poor access to contraceptives9
, lack of
contraceptive knowledge7
, unsatisfactory family planning services6
, and the
cost of contraceptives.5
- Existing literature in MSM individuals expressed how condom use interferes
with the intimacy component in sexually active in individuals resulting in no
use of protection.8
- The expectancy theory is refuted due to the results of the study. Gender did
not show to be the leading driving factor to higher sexual risk behaviors .
- Future researchers should emphasize the value of this study, complemented
with health educators to pave new avenues in designing preventative health
programs in regards to STIs. Activities might include seminars, educational
material, visuals, and information to reasonable outside resources.
Purpose
Background Table 2: Socio-demographic Characteristics of Study
Participants
Hypothesis Results:
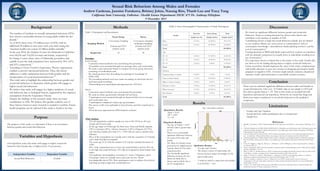
- The Sig. (2-Tailed) = 0.873
and this value is greater than
p=.05.
- There is not a statistically
significant difference between
the mean of the male and
female.
- The Mean for females using
protection was slightly greater
than the Mean for the males
using protection.
- The statistically significant
difference between the two
Means are likely due to
chance and not likely due to
the IV manipulation.
- Gender and Age Variation
- Sexual inactivity within participants due to inexperience
- Sample Size
There were no statistical significant difference between males and females in
sexual risk behaviors. Our t-test (2-Tailed) value in our sample is 0.873 and
this value is greater than p = .05. Due to this result, we accepted the null
hypothesis and rejected our hypothesis. However, we found that drugs and
alcohol are major contributors to sexual risk behaviors in the qualitative
component.
Qualitative Results:
- 16 codes and 5 themes.
- The themes consist of relationship, risk
factors, decision maker, knowledge of STI,
and sexually active.
- “I would say alcohol is a major factor when deciding
to use protection.” - Sean
Fig. 1: Descriptive Statistics
Results
Methods Discussion
Conclusion
Data Analyses
- For our quantitative analysis sample size was n=90. Of those, 60 were
female and 30 were male.
- In the age range of 18 through 30, there were Asian and Pacific Islander
(39%), Caucasian (25%), African American (1.96%), Hispanic (12.75%),
and American Indian (less than 1% ). 7.84% did not want to declare their
ethnicity.
- Most of the respondents are sexually active with the exception of 5 females
and 1 male that did not respond.
- The mean age 21.21 with the median of 21 and the standard deviation of
2.053.
- 60% of the respondents are in a low risk sexual behavior and the 30% are
in the high risk sexual behavior. 10% did not respond for both females and
males.
- Our qualitative demographics consisted of 1 Asian, 3 Hispanics, and 8
Caucasians. Some are sexually active and some are not. All are
knowledgeable about STIs. Most participants seem to indicate that alcohol
and drug use lead to high risk sexual behaviors.
References
1. Blashill, A., & Safren, S. (2015). Body dissatisfaction and condom use self-efficacy: A meta-analysis. Body Image, 12, 73-
77.
2. California Department of Public Health (CDPH) (2014). Chlamydia, cases and incidence rates, California counties and
selected city health jurisdictions. Retrieved from http://www.cdph.ca.gov/data/statistics/Documents/STD-Data-
Chlamydia-Provisional-Tables.pdf
3. Center of Disease & Prevention (CDC) (2015). Incidence, prevalence, and cost of sexually transmitted infections in
the United States. Retrieved from http://www.cdc.gov/std/stats/sti-estimates-fact-sheet-feb-2013.pdf
4. California Department of Public Health (CAPH) (2014). California Local Health Jurisdiction: STD Data Summaries.
Provisional Data. Retrieved from (https://www.cdph.ca.gov/data/statistics/Documents/STD-Data-LHJ-Orange.
pdf)
5. Foster, D., Higgins, J., Biggs, M., McCain, C., & Brindis, C. (2011). Willingness to Have Unprotected Sex. Journal of
Sex Research, 0(0), 1-8.
6. Garg, S., & Singh, R. (2014). Need for integration of gender equity in family planning services. Indian Journal of Medical
Research, 140(Suppl 1), 147-151.
7. Ritter, T., Dore, A., & McGeechan, K. (2015). Contraceptive knowledge and attitudes among 14-24-year-olds in New
South Wales, Australia. Australian and New Zealand Journal of Public Health, 39(3), 267-269.
8. Starks, T., Payton, G., Golub, S., Weinberger, C. , & Parsons, J. (2014). Contextualizing condom use: Intimacy
interference, stigma, and unprotected sex. Journal of Health Psychology, 19(6), 711-720.
9. Sidze, E., Lardoux, S., Speizer, I., Faye, C., Mutua, M., et al. (2014). Young women's access to and use of
contraceptives: The role of providers' restrictions in urban senegal. International Perspectives on Sexual and Reproductive
Health, 40(4), 176-183.
10. Vroom, V, H. (1964). Work and motivation. John Wiley & Sons, Inc. Expectancy Theory Cognitive Model. The
model and concepts of Valence, Expectancy and Force.
Sexual Risk Behaviors Among Males and Females
Andrew Cardenas, Jasmine Furukawa, Brittney Johns, Nasung Kim, Thanh Luu and Tracy Tang
California State University, Fullerton - Health Science Department: HESC 475 Dr. Anthony DiStefano
9 December 2015
Gender
Interview Survey Group Total
Sample size (%) Sample size(%) Sample size(%)
Male 8 (7.8%) 30 (29.4%) 38 (37.3%)
Female 4 (3.9%) 60 (58.8%) 64 (62.8%)
Total 102 (100%)
Age
18 - 20 2 (2.0%) 31 (30.4%) 22 (32.4%)
21 - 23 8 (7.8%) 50 (49.0%) 58 (56.9%)
24 - 30 2 (2.0%) 9 (8.8%) 11 (10.8%)
Total 102 (100%)
Ethnicity
American Indian or Alaskan 0 (0.0%) 1 (1.0%) 1 (1.0%)
Asian or Pacific Islander 1 (1.0%) 40 (39.2%) 41 (40.2%)
Black or African American 0 (0.0%) 2 (2.0%) 2 (2.0%)
Hispanic or Latino 3 (2.9%) 13 (12.8%) 16 (15.7%)
White/Caucasian 8 (7.8%) 26 (25.5%) 34 (33.3%)
Not Declared 0 (0.0%) 8 (7.8%) 8 (7.8%)
Total 102 (100%)
Table 2: Socio-Demographic Characteristics of Study Participants
Methods
Table 1: Participants and Recruitment
Focus Group Survey
Sampling Method
Convenience Sampling
(Friends and CSUF
students used)
Convenience Sampling
& Random Sampling
(Friends and CSUF
students used)
Sample Size 12 90