CONTENTS
INTRODUCTION
TERMINOLOGIES
GOALS OF OCCLUSAL ADJUSTMENT
SELECTIVE GRINDING :
INDICATIONS AND CONTRAINDICATIONS
IN NATURAL DENTITION
IN COMPLETE DENTURE
LABORATORY AND CLINICAL REMOUNTING PROCEDURES
3.
INTRODUCTION
• If theimportance of occlusion in dentistry were universally understood, no dentist would even consider
practicing without a working knowledge of the principles and skill required for successful occlusal
equilibrium.
• Whether dentists realize it or not, adjusting occlusion is a process that they are expected to do many
times a day, in any active practice.
It is usually done by a guess approach of grinding down the restoration until patient can close into
contact with the rest of the tooth regardless of the relationship of the mandible to the maxilla or the
position of the TMJ.
Such attempts are unbelievably crude when compared with the process based on correct equilibration
principles. It is always mutilative and unpredictable.
So the proper equilibration on properly selected patients is one of the most predictable service a dentist
4.
The primarypurpose of occlusal equilibration / correction is to
eliminate deflective occlusal contact that interferes with
physiologic function of TMJ.
And to achieve the purpose we must understand different
mandibular position, functions, and how they affect anterior
guidance and how the AG combines with the condylar guidance to
dictate ideal occlusal contour on posterior teeth.
5.
TERMINOLOGIES
Occlusion: Thestatic relationship between the incising or masticating surfaces of the
maxillary or mandibular teeth .
Articulation : The static and dynamic contact relationship between the occlusal
surfaces of the teeth during function
Centric relation: A maxillomandibular relationship, independent of tooth contact,
in which the condyles articulate in the anterior-superior position against the
posterior slopes of the articular eminences; in this position, the mandible is
restricted to a purely rotary movement; from this unstrained, physiologic,
maxillomandibular relationship, the patient can make vertical, lateral or
protrusive movements; it is a clinically useful, repeatable reference position.
6.
Centric occlusion: the occlusion of opposing teeth when the
mandible is in centric relation; this may or may not coincide with
the maximal intercuspal position.
Maximal intercuspal position :the complete intercuspation of the
opposing teeth independent of condylar position, sometimes
referred to as the best fit of the teeth regardless of the condylar
position.
7.
BALANCED OCCLUSION:Stable,simultaneous contact of the
opposing upper and lower teeth in centric relation position and a
continuous smooth bilateral gliding from this position to any
eccentric position within the normal range of mandibular function
Balancing side (non working) - That side of the mandible that
moves towards the medial line in a lateral excursion.
Working side - the side towards which the mandible moves in a
lateral excursion.
8.
GOALS OF OCCLUSALADJUSTMENT
The primary goal of any occlusal adjustment is Occlusal stability,
which is achieved by
• Elimination of Prematurity
• Elimination of Interferences
• Establishment of Centric Forces Directed Axially
• Establishment of Optimal Occlusion with out loss of OVD and
shapes of cusps and fossae.
9.
HOW TO RECOGNIZEA STABLE OCCLUSION
Stable stops on all the teeth when condyles are in centric relation.
Anterior guidance is in harmony with the border movement of the
envelope of function
Disclusion of all posterior teeth in protrusive movements
Disclusion of all posterior teeth on the non working side/balancing
side
Non interference of all posterior teeth on the working side, with
either the lateral anterior guidance or the border movements of the
condyle.
10.
SIGNS OF ANUNSTABLE OCCLUSION
Hypermobility of one or more teeth
Excessive wear
Migration of one or more teeth
Horizontal shifting
Intrusion
supraeruption
11.
• OCCLUSAL EQUILIBRATION:
Themodification of the occlusal form of the teeth with the intent of equalizing
occlusal stress, producing simultaneous occlusal contacts or harmonizing cuspal
relations.
• OCCLUSAL RESHAPING :
The intentional alteration of the occlusal surfaces of teeth to change their form.
12.
INDICATIONS FOR SELECTIVEGRINDING
• In the treatment of the mandibular dysfunction syndrome, where there is a lateral deflection to intercuspal
position from retruded occlusion(CR position). It should be considered only after reversible therapy.
• As a Pre-restorative treatment for fixed and removable prostheses where cusp interference has been
diagnosed. The removal of interferences and prematurities before tooth preparation saves chair time during the
seating of castings or prostheses.
• Indicated as Post-orthodontic treatment in adults.
• Indicated in treatment of trauma from occlusion, for decreasing mobility and fremitus.
• Indicated in Post-periodontal treatment where cusp interference and mobility on closure have been diagnosed.
• For Improvement in appearance of incisor and canine teeth.
• As emergency treatment of tooth extrusion following periodontal abscess.
13.
CONTRAINDICATIONS:
Severe overclosure.
Sensitive, worn and adolescent teeth.
Patients who are preoccupied with their teeth and for whom the
mouth and teeth have become an outlet for irrelevant muscle
activity.
14.
Treatment goals ofselective grinding
When the condyles are in the musculoskeletalstable(CR) position
and the articular discs are properly interposed ,all possible posterior
teeth contact evenly and simultaneously between centric cusp tips
and opposing flat surfaces.
When the mandible is moved laterally , the laterotrusive contacts on
the teeth disocclude the posterior teeth .
When the mandible is protruded the contacts on the the anterior
teeth disocclude the posterior teeth
In an upright head position ((alert feeding position) the posterior
teeth contact more heavily than the anterior teeth .
15.
AIMS IN THECORRECTION
Most of the damage occurs from functional occlusal disharmony which is within
limited range ( roughly 2mm) away from the centric position except in bruxism.
So this 2 mm rule is a convenient yardstick for the correction procedures.
In other words all teeth are placed in function for 2mm in each lateral excursion and
for 2mm in protrusive excursion.
• Occlusal therapy is any treatment that alters a patient’s occlusal condition. It can be
used to improve the function of masticatory system through the influence of occlusal
contact patterns and by altering the functional jaw position.
Types
▫ Reversible
▫ Irreversible
16.
Reversible therapy temporarilyalters the occlusal condition, the joint position, or
both.
• When this therapy is removed patient’s original condition might return.
Ex: occlusal appliance therapy
Irreversible occlusal therapy permanently alters the occlusal condition so that the
original condition cannot be recovered.
Ex: selective grinding, fixed prosthetic procedures and orthodontic therapy.
17.
RULE OF THIRDS
The success in achieving the treatment goals using a selective grinding
procedure alone is determined by the degree of misalignment of the teeth.
Since it is necessary to work within the confines of the enamel, only
minimal corrections can be made.
The “rule of thirds” is helpful in predicting the success of a selective
grinding procedure.
It deals with the buccolingual arch discrepancy when the condyles are in the
musculoskeletally stable position .
18.
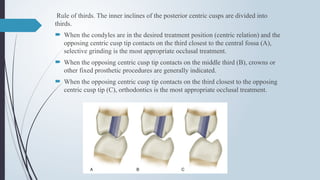
Rule of thirds.The inner inclines of the posterior centric cusps are divided into
thirds.
When the condyles are in the desired treatment position (centric relation) and the
opposing centric cusp tip contacts on the third closest to the central fossa (A),
selective grinding is the most appropriate occlusal treatment.
When the opposing centric cusp tip contacts on the middle third (B), crowns or
other fixed prosthetic procedures are generally indicated.
When the opposing centric cusp tip contacts on the third closest to the opposing
centric cusp tip (C), orthodontics is the most appropriate occlusal treatment.
19.
Once thebuccolinglial discrepancy of the posterior teeth is examined (i.E., Rule of thirds), the
patient applies force to the teeth
An anterosuperior shift of the mandible from CR to ICP will be noted.
The shorter the slide, the more likely it is that sg can be accomplished within the confines of the
enamel .
• The direction of the slide in the sagittal plane can also influence the success or failure of selective grinding.
(Horizontal and the vertical).
• Slide has a great horizontal component, it is more difficult to eliminate, within the confines of the
enamel.
• If it is almost parallel with the arc of closure (i.E., Large vertical component), elimi
nating it is
usually easier.
20.
Therefore boththe distance and the
direction of the slide are helpful in predicting
the outcome of selective grinding.
When cusps are relatively tall – direction of CR
to ICP slide is predominantly vertical (large
arrow).
When cusps are relatively flat – direction of CR
to ICP slide is greater horizontal component
(large arrow).
21.
Equilibration procedure canbe divided into 4 part:
Reduction of all contacting tooth surfaces that interfere with
completely seated condylar position
Selective reduction of tooth structure that interferes with lateral
excursions.
Elimination of all posterior tooth structres that interfere wuth
protrusive excursions
Harmonization of the anterior guidance : it is most often required to
do this in conjuction with the correction of lateral and protrusive
interferences
22.
RULES OF SELECTIVEGRINDING
RULE 1: NARROW STAMP CUSPS BEFORE RESHAPING FOSSAE
RULE 2 DON’T SHORTEN A STAMP CUSP
RULE 3: ADJUST CENTRIC INTERFERENCES FIRST
RULE 4 ELIMINATE ALL POSTERIOR INCLINE CONTACTS. PRESERVE CUSP
TIPS ONLY.
23.
DEVELOPING AN ACCEPTABLECENTRIC RELATION
CONTACT POSITION
The goal of this step is to create desirable tooth contacts when the condyles are in their
musculoskeletally stable (CR) position. In many patients an unstable occlusal condition exists
in CR and creates a slide to the more stable ICP.
Another way of describing this goal is to refer to it as elimination of the centric relation slide.
A slide of the mandible is created by the instability of contacts between opposing tooth
inclines. When the cusp tip contacts a flat surface in centric relation and force is applied by
the elevator muscles, no shift occurs.
Thus the goal in achieving acceptable contacts in ICP is to alter or reshape all inclines into
either cusp tips or flat surfaces.
Contacts from cusp tip to flat surface are also desirable since they effectively direct occlusal
forces through the long axes of the teeth.
24.
Eliminating Interferencesto Centric Relation For simplicity, centric
relation interferences can be differentiated into two types:
1. Interference to the arc of closure
2. Interference to the line of closure
Interference to the arc of closure
As the condyles rotate on their centric relation axis, each lower
tooth follows an arc of closure (Figure 33-2). Any tooth structure
that interferes with this closing arc has the effect of displacing the
condyles down and forward to achieve maximal intercuspation at
the most closed occlusal position. Most deviations from the arc of
closure require the condyle to move forward. Primary interferences
that deviate the condyle forward produce what is commonly called
an anterior slide.
The basic grinding rule to correct an anterior slide is always MUDL:
Grind the Mesial inclines of Upper teeth or the Distal inclines of
Lower teeth
25.
The CRslide can be classified as
anterosuperior,
anterosuperior and to the right, or
anterosuperior and to the left.
Each is created by specific opposing inclines. A basic understanding of these makes
establishing an acceptable CR position much simpler
26.
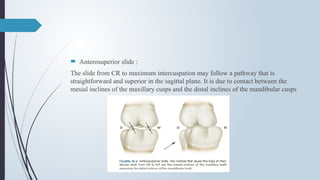
Anterosuperior slide:
The slide from CR to maximum intercuspation may follow a pathway that is
straightforward and superior in the sagittal plane. It is due to contact between the
mesial inclines of the maxillary cusps and the distal inclines of the mandibular cusps
27.
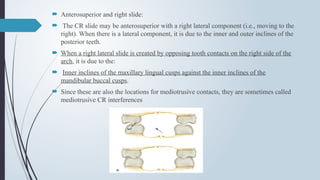
Anterosuperior andright slide:
The CR slide may be anterosuperior with a right lateral component (i.e., moving to the
right). When there is a lateral component, it is due to the inner and outer inclines of the
posterior teeth.
When a right lateral slide is created by opposing tooth contacts on the right side of the
arch, it is due to the:
Inner inclines of the maxillary lingual cusps against the inner inclines of the
mandibular buccal cusps.
Since these are also the locations for mediotrusive contacts, they are sometimes called
mediotrusive CR interferences
28.
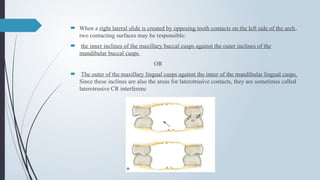
When aright lateral slide is created by opposing tooth contacts on the left side of the arch,
two contacting surfaces may be responsible:
the inner inclines of the maxillary buccal cusps against the outer inclines of the
mandibular buccal cusps
OR
The outer of the maxillary lingual cusps against the inner of the mandibular lingual cusps.
Since these inclines are also the areas for laterotrusive contacts, they are sometimes called
laterotrusive CR interferenc
29.
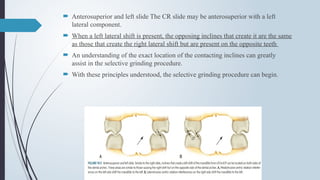
Anterosuperior andleft slide The CR slide may be anterosuperior with a left
lateral component.
When a left lateral shift is present, the opposing inclines that create it are the same
as those that create the right lateral shift but are present on the opposite teeth
An understanding of the exact location of the contacting inclines can greatly
assist in the selective grinding procedure.
With these principles understood, the selective grinding procedure can begin.
30.
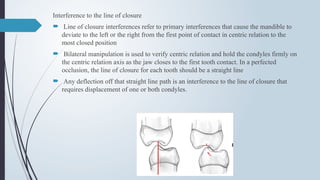
Interference to theline of closure
Line of closure interferences refer to primary interferences that cause the mandible to
deviate to the left or the right from the first point of contact in centric relation to the
most closed position
Bilateral manipulation is used to verify centric relation and hold the condyles firmly on
the centric relation axis as the jaw closes to the first tooth contact. In a perfected
occlusion, the line of closure for each tooth should be a straight line
Any deflection off that straight line path is an interference to the line of closure that
requires displacement of one or both condyles.
31.
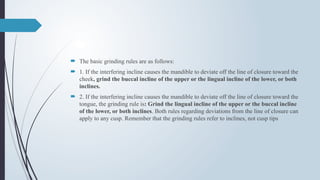
The basicgrinding rules are as follows:
1. If the interfering incline causes the mandible to deviate off the line of closure toward the
cheek, grind the buccal incline of the upper or the lingual incline of the lower, or both
inclines.
2. If the interfering incline causes the mandible to deviate off the line of closure toward the
tongue, the grinding rule is: Grind the lingual incline of the upper or the buccal incline
of the lower, or both inclines. Both rules regarding deviations from the line of closure can
apply to any cusp. Remember that the grinding rules refer to inclines, not cusp tips
32.
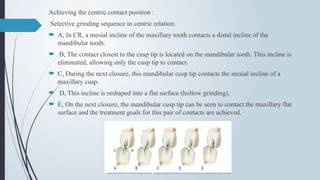
Achieving the centriccontact position :
Selective grinding sequence in centric relation.
A, In CR, a mesial incline of the maxillary tooth contacts a distal incline of the
mandibular tooth.
B, The contact closest to the cusp tip is located on the mandibular tooth. This incline is
eliminated, allowing only the cusp tip to contact.
C, During the next closure, this mandibular cusp tip contacts the mesial incline of a
maxillary cusp.
D, This incline is reshaped into a flat surface (hollow grinding).
E, On the next closure, the mandibular cusp tip can be seen to contact the maxillary flat
surface and the treatment goals for this pair of contacts are achieved.
33.
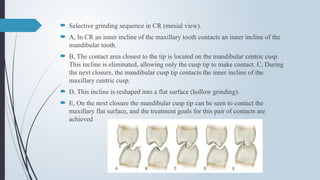
Selective grindingsequence in CR (mesial view).
A, In CR an inner incline of the maxillary tooth contacts an inner incline of the
mandibular tooth.
B, The contact area closest to the tip is located on the mandibular centric cusp.
This incline is eliminated, allowing only the cusp tip to make contact. C, During
the next closure, the mandibular cusp tip contacts the inner incline of the
maxillary centric cusp.
D, This incline is reshaped into a flat surface (hollow grinding).
E, On the next closure the mandibular cusp tip can be seen to contact the
maxillary flat surface, and the treatment goals for this pair of contacts are
achieved
34.
An acceptable CRposition is developed when :
Equal and simultaneious contacts occur between cusp tips and flat surfaces on all
posterior teeth
When the mandible is guided into centric relation and force is applied ,no side
shift or slide occurs
When the patient closes and taps in centric all posterior teeth are felt evenly
When, this is accomplished,orthopedic stability has been achieved
35.
Developing an acceptablelateral and protrusive
guidance
Acceptable laterotrusive contacts occur between the buccal cusps and not the
lingual cusps
During a straight protrusive movement the mandibular incisors pass down the
lingual surfaces of maxillary incisors , thus disoccluding the posterior teeth
During lateroprotrusive movement the lateral incisors can also be involved in the
guidance
As the movement becomes more lateral the canines begin to contribute to the
guidance
36.
ADJUSTMENT FOR LATERAL
INTERFERENCES
Ask the patient to close in CR and visualize the relationship of the anterior teeth
then assist the patient through laterotrusive movements
it is recommended to clear the balancing interferences first , the working and
finally the protrusive.
Balncing side interferences on second molars are most commonly missed
interferences
On the working side the canines must contact during the laterotrusive movements
and disocclude the posteriors teeth( canine guidance)
When canines are not positioned such that they can immediately provide
latertrusive guidance, a group function guidance –where the mandible is laterally
guided by the premolars and mesiobuccal cusps of the first molars.
37.
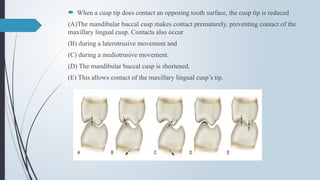
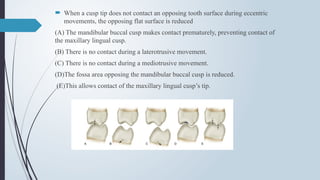
When acusp tip does contact an opposing tooth surface, the cusp tip is reduced
(A)The mandibular buccal cusp makes contact prematurely, preventing contact of the
maxillary lingual cusp. Contacts also occur
(B) during a laterotrusive movement and
(C) during a mediotrusive movement.
(D) The mandibular buccal cusp is shortened.
(E) This allows contact of the maxillary lingual cusp’s tip.
38.
When acusp tip does not contact an opposing tooth surface during eccentric
movements, the opposing flat surface is reduced
(A) The mandibular buccal cusp makes contact prematurely, preventing contact of
the maxillary lingual cusp.
(B) There is no contact during a laterotrusive movement.
(C) There is no contact during a mediotrusive movement.
(D)The fossa area opposing the mandibular buccal cusp is reduced.
(E)This allows contact of the maxillary lingual cusp’s tip.
39.
During aprotrusive movement, posterior protrusive contacts can occur between
the distal inclines of the maxillary lingual cusps and the mesial inclines of the
mandibular buccal cusps.
When these potential contact sites are added to the occlusal surface of the
posterior teeth, it is possible to visualize all the potential areas of eccentric
contacts on the posterior teeth
40.
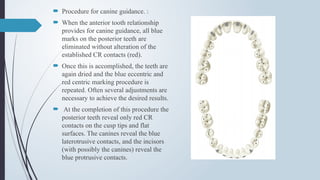
Procedure forcanine guidance. :
When the anterior tooth relationship
provides for canine guidance, all blue
marks on the posterior teeth are
eliminated without alteration of the
established CR contacts (red).
Once this is accomplished, the teeth are
again dried and the blue eccentric and
red centric marking procedure is
repeated. Often several adjustments are
necessary to achieve the desired results.
At the completion of this procedure the
posterior teeth reveal only red CR
contacts on the cusp tips and flat
surfaces. The canines reveal the blue
laterotrusive contacts, and the incisors
(with possibly the canines) reveal the
blue protrusive contacts.
41.
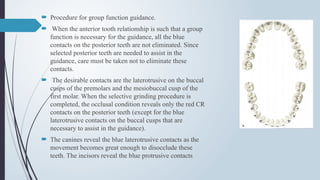
Procedure forgroup function guidance.
When the anterior tooth relationship is such that a group
function is necessary for the guidance, all the blue
contacts on the posterior teeth are not eliminated. Since
selected posterior teeth are needed to assist in the
guidance, care must be taken not to eliminate these
contacts.
The desirable contacts are the laterotrusive on the buccal
cusps of the premolars and the mesiobuccal cusp of the
first molar. When the selective grinding procedure is
completed, the occlusal condition reveals only the red CR
contacts on the posterior teeth (except for the blue
laterotrusive contacts on the buccal cusps that are
necessary to assist in the guidance).
The canines reveal the blue laterotrusive contacts as the
movement becomes great enough to disocclude these
teeth. The incisors reveal the blue protrusive contacts
42.
force isapplied to the inferior border and angle of the mandible in a superomedial
direction as the patient moves in the mediotrusive direction.
It assists the condyle in making a border movement that may not occur during normal
function but can occur during parafunctional activity.
Any tooth contacts that occur during this assisted movement are identified and eliminated
during the selective grinding procedure.
43.
EVALUATION INTHE UPRIGHT HEAD-POSITION (Alert Feeding Position) The
selective grinding procedure is not complete until the upright head position has been
evaluated.
Evaluation for postural changes of the mandible must be accomplished before the
patient is dismissed.
In the upright position with the head tilted forward approximately 30 degrees (placing
the Frankfort plane 30 degrees off horizontal), the patient closes on the posterior teeth.
It is important to determine whether a postural change in the mandibular position has
occurred that will cause anterior tooth contacts to be heavier than posterior tooth contact
If this has occurred, the anterior tooth contacts are reduced slightly until the posterior
teeth contact more heavily
44.
The mostsuccessful way to question a patient in the alert feeding position is to
ask the patient to close the mouth and tap the posterior teeth together.
While this is being done, the patient is asked whether the posterior teeth contact
predominantly, the anterior teeth predominantly, or both anterior and posterior
teeth contact equally. If the posterior teeth are contacting predominantly, minimal
postural change has occurred and the selective grinding procedure is complete.
If, however, the anterior teeth are contacting heavily or both anterior and
posterior teeth are contacting evenly, a final adjustment in the alert feeding
position is necessary.
In this upright position the anterior teeth are dried and red marking paper is
placed between them. The patient again taps on the posterior teeth.
Any red CR contacts on the anterior teeth are slightly reduced until the patient
reports feeling predominantly the posterior teeth contacting. Normally one or two
adjustments will accommodate for this postural change of the mandible. As soon
as the posterior teeth are felt more predominantly, the selective grinding
procedure is complete.
45.
PARTIAL SELECTIVE GRINDING
insome instances patients may only need Partial selective grinding.
Ex: very prominent mediotrusive contact restricts mandibular movement
during function – eliminate it without altering other features of occlusion.
INDICATIONS:
Symptoms associated with new restorations – if undesirable contacts are
present –eliminated.
Single tooth experiencing mobility or pulpitis – lighten the tooth in ICP
while eliminating eccentric contacts
46.
IN COMPLETE DENTURES:
A special lingual contact occlusion has been developed with a bilaterally balanced
denture occlusion.
The objective of balancing a denture occlusion is to create simultaneous bilateral
contacts from the centric relation position to all eccentric occlusal positions that are
free of interferences.
These multiple contacts should be smooth, uniform ,and in harmony with the
temporomandibular joints and neuromuscular activity.
Once achieved, first by the proper positioning of the teeth during the setup and then
refined by selective grinding, a lingual contact balanced occlusion also provides lever
stability for the denture bases.
47.
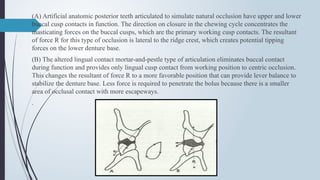
(A) Artificial anatomicposterior teeth articulated to simulate natural occlusion have upper and lower
buccal cusp contacts in function. The direction on closure in the chewing cycle concentrates the
masticating forces on the buccal cusps, which are the primary working cusp contacts. The resultant
of force R for this type of occlusion is lateral to the ridge crest, which creates potential tipping
forces on the lower denture base.
(B) The altered lingual contact mortar-and-pestle type of articulation eliminates buccal contact
during function and provides only lingual cusp contact from working position to centric occlusion.
This changes the resultant of force R to a more favorable position that can provide lever balance to
stabilize the denture base. Less force is required to penetrate the bolus because there is a smaller
area of occlusal contact with more escapeways.
.
48.
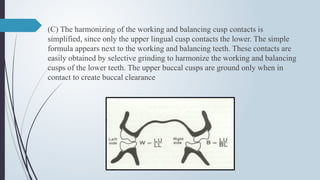
(C) The harmonizingof the working and balancing cusp contacts is
simplified, since only the upper lingual cusp contacts the lower. The simple
formula appears next to the working and balancing teeth. These contacts are
easily obtained by selective grinding to harmonize the working and balancing
cusps of the lower teeth. The upper buccal cusps are ground only when in
contact to create buccal clearance
49.
PREREQUISITES FOR BALANCINGTHE
OCCLUSION :
There are four specific conditions that
must be met by the mandibular posterior
teeth in order to achieve a balanced
occlusion:
(1) the mandibular posterior teeth must be
set so that the occlusal surfaces are
horizontal
(2) the plane of occlusion must have a
proper orientation;
(3) a compensating curve must be set
(4) the teeth must be modified so that there
are no interlocking transverse ridges
The maxillary teeth must be
(1) modified to eliminate buccal cusp
contact,
(2) set so that the upper lingual cusps have
a positive but static centric occlusal
contact, and
(3) have no buccal cusp contacts in lateral
excursions
50.
Errors inocclusal relationships of teeth on complete dentures are caused by various factors .
They include:
changes in the condition of the temporomandibular joints,
unstable trial bases for interarch relationship record,
incorrect use of face-bow, transfer of casts into the articulator,
inaccurately defined vertical and horizontal relation,
irregular arrangement of the posterior teeth,
use of excessive pressure during pressing of acrylic resin into the flask, inadequately closed
flasks during polymerisation, as well as overheating of the finished dentures by final polishing
Occlusal errors can also result from inevitable dimensional changes in the denture material
during and after polymerisation (contractions) and from wearing of the finished dentures in the
mouth
51.
REMOUNT PROCEDURES:
Remountprocedure is any method used to relate restorations to an
articulator for analysis and/or to assist in development of a plan for
occlusal equilibration or reshaping
Remounting can be of two types:
• Laboratory remount
• Clinical remounting
52.
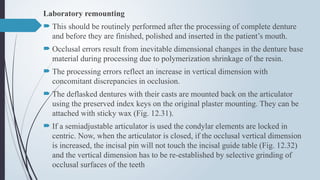
Laboratory remounting
Thisshould be routinely performed after the processing of complete denture
and before they are finished, polished and inserted in the patient’s mouth.
Occlusal errors result from inevitable dimensional changes in the denture base
material during processing due to polymerization shrinkage of the resin.
The processing errors reflect an increase in vertical dimension with
concomitant discrepancies in occlusion.
The deflasked dentures with their casts are mounted back on the articulator
using the preserved index keys on the original plaster mounting. They can be
attached with sticky wax (Fig. 12.31).
If a semiadjustable articulator is used the condylar elements are locked in
centric. Now, when the articulator is closed, if the occlusal vertical dimension
is increased, the incisal pin will not touch the incisal guide table (Fig. 12.32)
and the vertical dimension has to be re-established by selective grinding of
occlusal surfaces of the teeth
53.
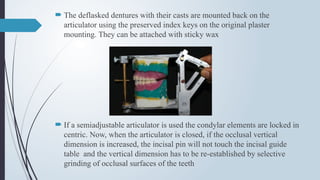
The deflaskeddentures with their casts are mounted back on the
articulator using the preserved index keys on the original plaster
mounting. They can be attached with sticky wax
If a semiadjustable articulator is used the condylar elements are locked in
centric. Now, when the articulator is closed, if the occlusal vertical
dimension is increased, the incisal pin will not touch the incisal guide
table and the vertical dimension has to be re-established by selective
grinding of occlusal surfaces of the teeth
54.
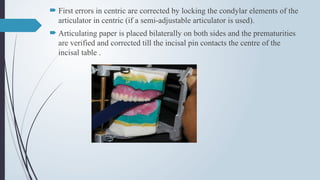
First errorsin centric are corrected by locking the condylar elements of the
articulator in centric (if a semi-adjustable articulator is used).
Articulating paper is placed bilaterally on both sides and the prematurities
are verified and corrected till the incisal pin contacts the centre of the
incisal table .
55.
If abalanced occlusion in eccentric positions has been provided, then the
prematurities in protrusion and lateral excursions are verified.
The incisal pin should smoothly and evenly contact the incisal table during
these movements. Care should be taken not to grind the centric contacts by
using articulating paper of a different colour for checking eccentric
prematurities.
In general, BULL rule (buccal upper, lingual lower) which advocates
grinding of the mentioned cusps without modifying the functional cusps
should be used while performing the corrections.
56.
SELECTIVE GRINDING FORSTATIC CENTRIC
CONTACTS
Once the initial balance is achieved during the setup of
the maxillary posteriors, the complete occlusion must
be refined by selective grinding.
First remove the incisal guide pin so that only the teeth
are holding the proper occluding vertical dimension.
A length of thin articulating paper is placed on the
posterior teeth, and the articulator is gently tapped
several times in centric occlusion.
If marks show on lower cusp inclines, gently grind the
inclines to eliminate deflective contacts.
57.
If thereare any upper lingual cusps out of contact, the nonoccluding maxillary
teeth are repositioned by moving the lingual cusps down into contact. It is also
possible to selectively grind the teeth into a stable centric occlusion. Only the
lower central fossae or marginal ridges should be ground, not the upper lingual
cusps.
If any significant grinding is done on the lower teeth , the occlusal vertical
dimension will be reduced and anterior interference will occur.
The method of attaining a stable centric occlusion in which all the upper lingual
cusps are in the lower common central fossa depends on the assessment of the
problem .
58.
If thenonoccluding upper lingual cusps are nearly in contact, modest
grinding can be done, as it will not significantly close the occlusal
vertical dimension.
If any upper buccal cusps or inclines are in contact, they should be
ground out of contact. Only the upper lingual cusp, that is, the pestle of
the mortar-and-pestle-type lingual contact occlusion, should articulate
with the lower posteriors
The final result after several tappings and spot grindings should be stable
contacts with all upper lingual cusps in the common lower central fossae.
59.
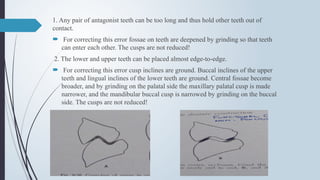
1. Any pairof antagonist teeth can be too long and thus hold other teeth out of
contact.
For correcting this error fossae on teeth are deepened by grinding so that teeth
can enter each other. The cusps are not reduced!
2. The lower and upper teeth can be placed almost edge-to-edge.
For correcting this error cusp inclines are ground. Buccal inclines of the upper
teeth and lingual inclines of the lower teeth are ground. Central fossae become
broader, and by grinding on the palatal side the maxillary palatal cusp is made
narrower, and the mandibular buccal cusp is narrowed by grinding on the buccal
side. The cusps are not reduced!
60.
3. The upperteeth can be positioned too buccally in relation to the lower teeth.
For correcting this error the maxillary lingual cusp is narrowed by broadening the central
fossa, and the mandibular buccal cusp is ground buccally by broadening the central fossa.
Actually, the palatal cusp is ground in the palatal direction and the mandibular buccal cusp
in the buccal direction so that teeth can enter each other. The cusps have not been reduced
or are not reduced!
61.
SELECTIVE GRINDING FORWORKING AND
BALANCING CONTACTS
When the mandible moves to the left, this becomes the working side.
The upper left lingual cusps should contact the lower left lingual cusps. The right
side is then the balancing side, and the upper lingual cusps should contact the
lower buccal cusps
Only one lateral excursion (either the left or right) should be checked at a time.
After the working and balancing contacts for left lateral excursion have been
equilibrated, then check the right lateral excursion.
Place a strip of thin articulating paper between the posterior teeth bilaterally.
While keeping gentle pressure on the maxillary member of the articulator, move it
to the right (this is equivalent to moving the mandible to the left). This duplicates
a left lateral excursion.
62.
Ideally, inthis occlusal scheme there should be five working cusp contacts, five
balancing cusp contacts, and no upper buccal cusp contacts.
When functioning as balancing contacts, upper lingual cusps ride lower buccal
(lingual-facing inclines) cusp inclines diagonally.
W hen acting as working cusps, upper lingual cusps pass between modified
triangular ridges of the lower lingual cusps that run either to the marginal ridge or
to the groove between the cusps of the lower molars
There usually is some prematurity on the working or balancing side that prevents
total working or balancing cusp contact. Grind the marked premature balancing
contacts, heavily marked working side contacts, or both, on the lower teeth. By
selectively spot grinding the premature inclines and cusps, a smooth harmonious
multiple contact of the desired contacts will occur. Do not grind the upper lingual
cusps
63.
There mayalso be upper buccal cusp contact on the working side.
This is usually the result of inadequate buccal cusp rise made during
the setup.
The upper posterior teeth may be reset to increase clearance if the
contact is severe or may be ground if the contact is slight. Do not
grind the lower buccal cusps. There should be no upper buccal cusp
contact in any excursion
64.
As thepremature inclines and high cusps are selectively ground
until there is simultaneous contact of working and balancing cusps,
the cusp rise is gradually reduced. This may create anterior
interference on the working side, which must be eliminated.
Usually, there is sufficient compensating horizontal overlap for any
vertical overlap to allow for a simple solution by grinding.
65.
The lingualof the upper anterior incisal edges and the labial of the
lower anteriors are ground to eliminate any interference that
develops while selectively grinding to balance the occlusion.
Grinding on the anterior teeth should always be conservative so that
the esthetic value of the anterior teeth is not disturbed.
W hen it is apparent that selective grinding to balance the occlusion
will cause anterior interference, the upper posterior teeth should be
reset to open the occlusal vertical dimension enough to clear the
anterior teeth after balancing for eccentric excursions
66.
The finishedresult should be a smooth gliding left lateral excursion
with ten simultaneous working and balancing contacts (five working
and five balancing contacts).
Now equilibrate the right side with opposite lateral excursion in the
same manner.
67.
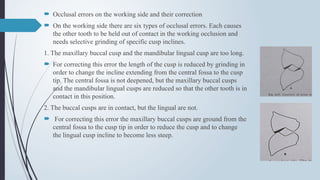
Occlusal errorson the working side and their correction
On the working side there are six types of occlusal errors. Each causes
the other tooth to be held out of contact in the working occlusion and
needs selective grinding of specific cusp inclines.
1. The maxillary buccal cusp and the mandibular lingual cusp are too long.
For correcting this error the length of the cusp is reduced by grinding in
order to change the incline extending from the central fossa to the cusp
tip. The central fossa is not deepened, but the maxillary buccal cusps
and the mandibular lingual cusps are reduced so that the other tooth is in
contact in this position.
2. The buccal cusps are in contact, but the lingual are not.
For correcting this error the maxillary buccal cusps are ground from the
central fossa to the cusp tip in order to reduce the cusp and to change
the lingual cusp incline to become less steep.
68.
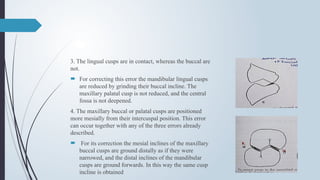
3. The lingualcusps are in contact, whereas the buccal are
not.
For correcting this error the mandibular lingual cusps
are reduced by grinding their buccal incline. The
maxillary palatal cusp is not reduced, and the central
fossa is not deepened.
4. The maxillary buccal or palatal cusps are positioned
more mesially from their intercuspal position. This error
can occur together with any of the three errors already
described.
For its correction the mesial inclines of the maxillary
buccal cusps are ground distally as if they were
narrowed, and the distal inclines of the mandibular
cusps are ground forwards. In this way the same cusp
incline is obtained
69.
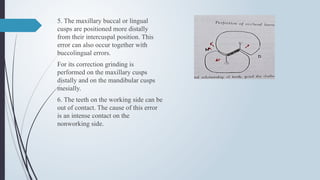
5. The maxillarybuccal or lingual
cusps are positioned more distally
from their intercuspal position. This
error can also occur together with
buccolingual errors.
For its correction grinding is
performed on the maxillary cusps
distally and on the mandibular cusps
mesially.
6. The teeth on the working side can be
out of contact. The cause of this error
is an intense contact on the
nonworking side.
70.
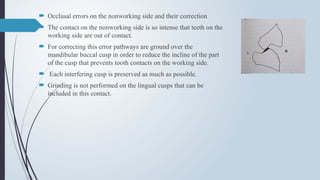
Occlusal errorson the nonworking side and their correction
The contact on the nonworking side is so intense that teeth on the
working side are out of contact.
For correcting this error pathways are ground over the
mandibular buccal cusp in order to reduce the incline of the part
of the cusp that prevents tooth contacts on the working side.
Each interfering cusp is preserved as much as possible.
Grinding is not performed on the lingual cusps that can be
included in this contact.
71.
SELECTIVE GRINDING FORPROTRUSIVE
BALANCE
The upper right and left second molar cusps should ride up the distal inclines of
the lower right and left second molars with enough rise to clear the anteriors.
There should be no interference between the buccal cusps of the upper teeth and
any of the lower buccal cusps.
The movement itself must be smooth and devoid of any “washboard” effect. If
anterior interference occurs, either move or grind the lower offending anterior
tooth slightly or increase the distal incline on the lower second molar by increasing
the compensating curve.
Rectification of errors in protrusion
Reducing distolingual inclines of maxillary buccal cusps and mesiobuccal inclines
of mandibular lingual cusp
72.
SELECTIVE GRINDING OF
NONANATOMICTEETH
When noncusp form posterior teeth are used and selective grinding procedures
are instituted, the occlusal surfaces posterior teeth are altered to make harmonious
contact on the right side and on the left side when the jaws are in centric relation
1. Secure the condylar elements on the articulator against the condylar housing.
2. Place articulating tape over the occlusal surfaces and incisal edges of all of the
mandibular teeth.
3. Tap the teeth together to record the contacting areas.
4. Using a mounted wheel, grind the occlusal surfaces of the teeth until
simultaneous even contacting areas on the right and left are developed. Do not allow
the anterior teeth to make contact. Develop small areas of contact uniformly
dispersed over the occlusal surfaces of the distal of the first premolar, the second
premolar, the first molar, and the mesial of the second molar
73.
5. Polishall altered surfaces with a rubber point.
6. Exercise care to maintain the occlusal surfaces of the mandibular
arch on a plane.
7. When using porcelain teeth in one arch to oppose acrylic resin
teeth in the opposite arch. do all grinding of the occlusal surfaces on
the acrylic resin teeth
74.
STRIPPING METHOD FORTHE OCCLUSAL
EQUILlBRATION OF 0' TEETH
Another acceptable technique to refine the occlusion for cuspless. nonanatomic teeth is the
carborundum stripping technique. which was originally published by Dr. Gronas in 1970
The primary purpose of nonanatomic posterior teeth when set on a flat plane is to eliminate
cuspal inferences. Therefore. it is necessary during the selective grinding procedure in this
technique to maintain the previously established flat occlusal scheme.
A rotary instrument usually produces irregularities in the flat occlusal surfaces. Waterproof
carborundum abrasive paper is the most ideal material to use with this method.
A 220 grit paper is used to modify porcelain teeth. and a fine 320 grit paper is used for acrylic
resin teeth.
Strips of the abrasive paper should be cut in varying widths to allow for the reduction of
individual teeth or to reduce entire quandrants. It should be remembered that the flatness of the
occlusal surfaces must be maintained throughout the entire grinding procedure. The technique
is as follows:
75.
1. Adjusting forCentric Occlusion
a. Locate the premature contacts with articulating ribbon or paper. If there is a grossly
tipped tooth that is above the occlusal plane,reduce the tooth with a stone or bur until a flat
occlusal plane is obtained.
b. Check the eccentric movements. and if any premature contacts are present in any of the
positions,remove them also with a stone or bur before proceeding further with the grind in.
c.place a carborundum strip of the appropriate width with the abrasive side against the
teeth that are to be reduced. and gently close the articulator in centric relation.
d. Apply light pressure to the upper member of the articulator. and pull the strip briskly
between the teeth. Always pull the strip in the same plane as the flat occlusal surfaces of the
teeth in order to avoid rounding of the bucco-occlusal angle of the teeth.
Evaluate the vertical dimension of occlusion carefully throughout the procedure. as the
rapid reduction of the occlusal surfaces could allow overclosure past the original vertical
dimension.
76.
e. Reductionof the contacts with the strips is continued by stripping an equal
number of times with the abrasive side alternated up and down until uniform
bilateral contacts on the posterior teeth are obtained.
By alternating the abrasive side of the paper between the maxillary and
mandibular teeth. it will equalize the reduction between the twoarches and ensure
that the occlusal plane will be kept flat. Finish the reduction with finer grits of
sandpaper strips in order to produce a smoother flat surface.
77.
2. Adjustingfor the Eccentric Occlusion a. Check each eccentric
position (working, balancing, protrusive) and remove any premature
contacts with a flat stone while maintaining a flat occlusal plane.
Following the adjustment of the eccentric positions, the centric
occlusion should again be checked and any necessary modifications
made with the abrasive strips of the appropriate width along with
ensuring that there is no contacting of the maxillary and mandibular
anterior teeth in that position.
78.
CLINICAL REMOUNTING
Occlusalharmony is important for the complete denture to function efficiently, be
comfortable and to preserve the tissues.
Causes of occlusal discrepancy Even after lab remounting and selective grinding
can be due to:
• Errors in jaw relation records.
• Errors in mounting casts on articulator.
• Changes in supporting tissues since impressions were made.
• Differences in tissue adaptation between record bases and processed denture bases.
• Realeff (resiliency like effect)
○ When a passive recording material is used for impression making the
maxillomandibular relation changes in the final denture leading to occlusal
discrepancy (premature contact).
Intraoral correction
There aremany acceptable intraoral methods for correcting occlusal
disharmony. However, the intraoral methods are more accurate if the
uneven contacting of the teeth has been first corrected with laboratory
remount and patient remount procedures. Some of the intraoral
methods follow.
81.
1.ARTICULATING PAPER
• Articulatingpaper alone will not give as accurate an indication of premature contacts
as some other methods.
• The resiliency of the supporting tissues allows the dentures to shift; therefore, the
paper markings are frequently false and misleading.
• The denture bases can move from the basal seat, causing the teeth in the opposite
side of the arch or the opposite end of the arch to contact prematurely and produce
an incorrect marking.
• To place articulating paper on one side of the arch may induce the patient to close to
or away from that side. Articulating paper should be placed on both arches, a
procedure sometimes difficult to do accurately
82.
CENTRAL BEARING DEVICES
Some operators use one type of central bearing device, the correlator, to correct
occlusion in the mouth.
The central bearing pin works on a spring. As the patient closes the mouth, the
pin in the mandibular mounting contacts a metal plate in the vault of the
maxillary denture.
Thus, by holding the maxillary denture up and the mandibular denture down, the
pin creates a tension before the teeth contact. If a premature contact is made by
one tooth, the dentures do not shift because the spring holds the other teeth apart.
The interceptive occlusal contacts are located with articulating ribbon.
The central bearing device can be mounted on dentures in 3 to 4 minutes and will
serve to disprove the theory that occlusion can be corrected by having the patient
close down on a piece of articulating paper alone.
Another type of central bearing device, the Coble device, has a central bearing
pin without a spring. Like the correlator, it requires careful control of the patient
throughout the procedure.
83.
OCCLUSAL WAX
Adhesive green wax is placed on the occlusal surfaces of the mandibular
denture. Points of penetration that occur upon closing with the jaws in
centric relation may be marked with a lead pencil and relieved where
indicated .
With this method one may also locate points of interference during
functional movements. One disadvantage of this method is that shifting
of the dentures over resilient supporting tissues in eccentric jaw positions
will give false markings. This is an excel-lent method for correcting
occlusion in the centric position only
84.
ABRASIVE PASTE
Theuse of abrasive paste in the mouth has many disadvantages. The
shifting of the base as a result of premature contact may result in
altering the occlusion so that centric occlusion does not correspond
to centric relation. Cusps that maintain the occlusal vertical
dimension may be destroyed. Abrasive paste is not selective.
85.
Disadvantages ofintraoral correction
• The resiliency and displaceability of the supporting soft tissues will
mask the premature contacts.
• It is impossible to observe the discrepancy from all aspects with the
dentists’ naked eye.
• Patients also do not identify and quote the problem immediately.
• Occlusal interferences can cause pain which makes the patient avoid
the same, giving false markings.
86.
PATIENT REMOUNT ANDSELECTIVE
GRINDING
The patient remount method is to remount the dentures on an articulator by means of
interocclusal records made in the patient's mouth. This is by far the most accurate
procedure.
It has the following advantages:
1. It reduces palient participation.
2. It permits the dentist to see the procedures better.
3. It provides a stable working foundation; bases are not shifting on resilient tissues.
4. The absence of saliva makes possible more accurate markings with the
articulating paper or tape.
5. Corrections can be made away from the patient, thus preventing occasional
objections when patients see their dentures being ground.
87.
REMOUNT PROCEDURES:
Tocarry out a patient remount procedure, orient the mandibular denture to the maxillary
denture by means of an interocclusal record with the jaws in centric relation.
1. Place two thicknesses of wax on the occlusal surfaces of the mandibular teeth. Soften
with a flame from an alcohol torch or immerse in water at 130°F.
2. Carry to the mouth and have the patient close into the wax when the jaws are in centric
relation. Closure must be short of tooth-tooth contact. The wax record is not acceptable if
the teeth penetrate to make contact. Chill with cold air and remove.
3. Do not return the wax record to the mouth, as it may be distorted by the patient. Trim
the wax so that only slight indentations remain, and expose the facial side so that the
seating of the maxillary denture can be visually checked
88.
After properlyorienting the mandibular denture to the maxillary denture by
means of the interocclusal record, secure it with sticky wax.
Seat the mandibular cast in the denture and attach it to the mandibular member of
the articulator with plaster.
To check what has been recorded to be the patient's centric occlusion, make
another wax interocclusal record. Replace the dentures on the articulator.
With the condylar elements freed, place the teeth in the indentations in the wax
record. The condylar elements should rest against the stops (Fig. 18-10). Repeat
the procedure until two consecutive records are accepted. When the accuracy of
the articulator mountings is verified, occlusal disharmany when the jaws are in
centric relation or in eccentric relation can be corrected by selective grinding
procedures
89.
• Procedure:
○ Theclinical remounting is performed using interocclusal check
records
○ If the original final casts are intact, the dentures are just remounted
on the articulator with the new interocclusal check record and the
centric relation is verified by adjusting the condylar controls
If necessary, the lower cast is mounted again on the articulator in the
new position.
○ If the original final casts are destroyed, then remount casts are made.
90.
Remount cast:A cast formed on prosthesis for the purpose of mounting the
prosthesis on an articulator (GPT8).
Procedure of fabricating a remount cast The undercuts present in the tissue
surface of the dentures are blocked out with plasticine or wax.
The tissue surface of the denture is coated with a separating medium like
petroleum jelly.
Quick setting plaster is vibrated onto the tissue surface, such that it captures
the peripheral roll, but it should not cover the external surface as it may
become difficult to remove the denture from the cast
The maxillary cast can be mounted with a remounting jig (if fabricated after
laboratory remount and selective grinding). Alternately, it can be mounted on
the articulator using a new facebow transfer .
91.
• Themandibular cast is mounted using the interocclusal check
record
• Selective grinding procedures using BULL law (buccal cusp of
upper and lingual cusp of lower are performed to correct occlusal
discrepancies using articulating paper,
• Any area of the denture that is trimmed during denture insertion
should be polished.
92.
T-SCAN
T-scan II®Computerized Occlusal Analysis System
First Introduced By Maness And Others In 1984 As The T-scan I System, The New
Version From Tekscan (Boston, MA) Has Become One Of The Most Practical
Measuring Instruments For Precise Analysis Of Occlusal Contacts.
However, The Use Of The T-scan Alone Has Value As A Precise Recorder Of
Occlusal Interferences And As A Guide For Determining When Occlusal Treatment
Has Been Completed. Amount Of Relative Occlusal Force Is Displayed In 3-
dimensional Colored Bar Graphs.
The Color And Height Of Each Bar Indicates The Intensity Of Force Per Contact.
Problematic Occlusal Contact Will Be Displayed On The 2-dimensional Dental Arch
Window.
93.
CONCLUSION
Teeth orany prosthesis replacing missing teeth aims towards
establishing an occlusal contact that is in harmonious with the
positions of the condyles & the musculature of the mandible.
Complete denture construction is not complete without a
remounting procedure. So in order to achieve patient comfort, long
term success of dentures it is mandatory to follow both the
laboratory and the clinical remounting procedures to eliminate all
the factors that cause occlusal errors.