This document discusses screening guidelines for various cancers in women, including cervical, ovarian, endometrial, and breast cancer. It provides details on:
- The purpose and criteria for effective cancer screening programs
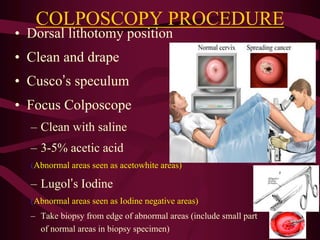
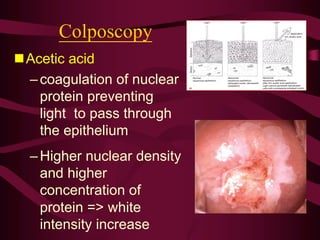
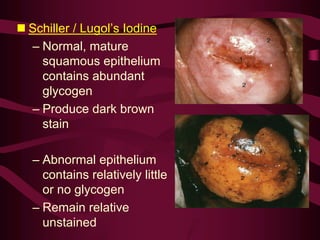
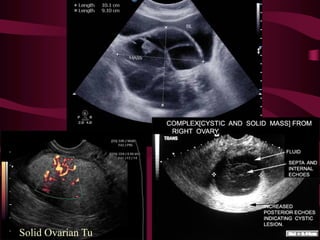
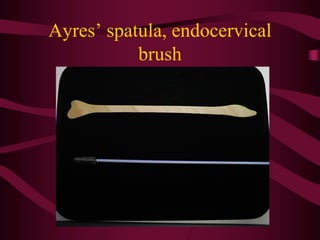
- Screening recommendations and techniques for each cancer type, including cervical cytology, colposcopy, transvaginal ultrasound, and mammography
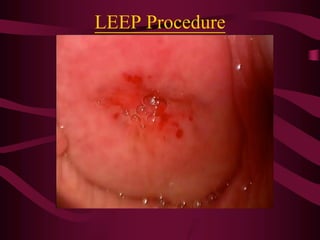
- Management of abnormal screening results, such as follow up tests or procedures for lesions of different grades
- Challenges with screening for some cancers like ovarian cancer due to limitations in current screening tests





































![DOC-20241220-WA0005[1].pptx screening of breast cancer](https://cdn.slidesharecdn.com/ss_thumbnails/doc-20241220-wa00051-250706171952-02b5ca46-thumbnail.jpg?width=640&height=640&fit=bounds)




















![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
















