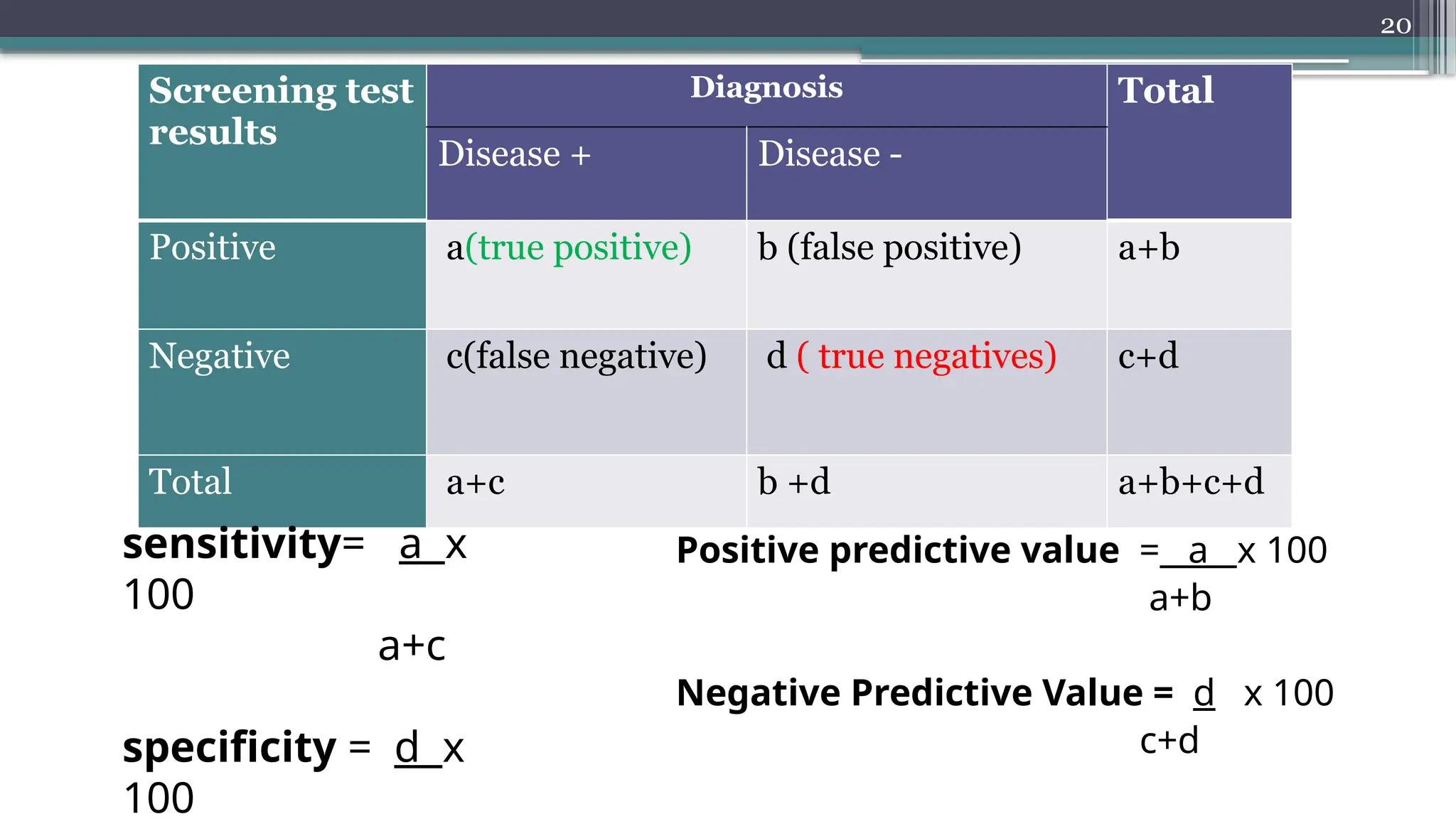
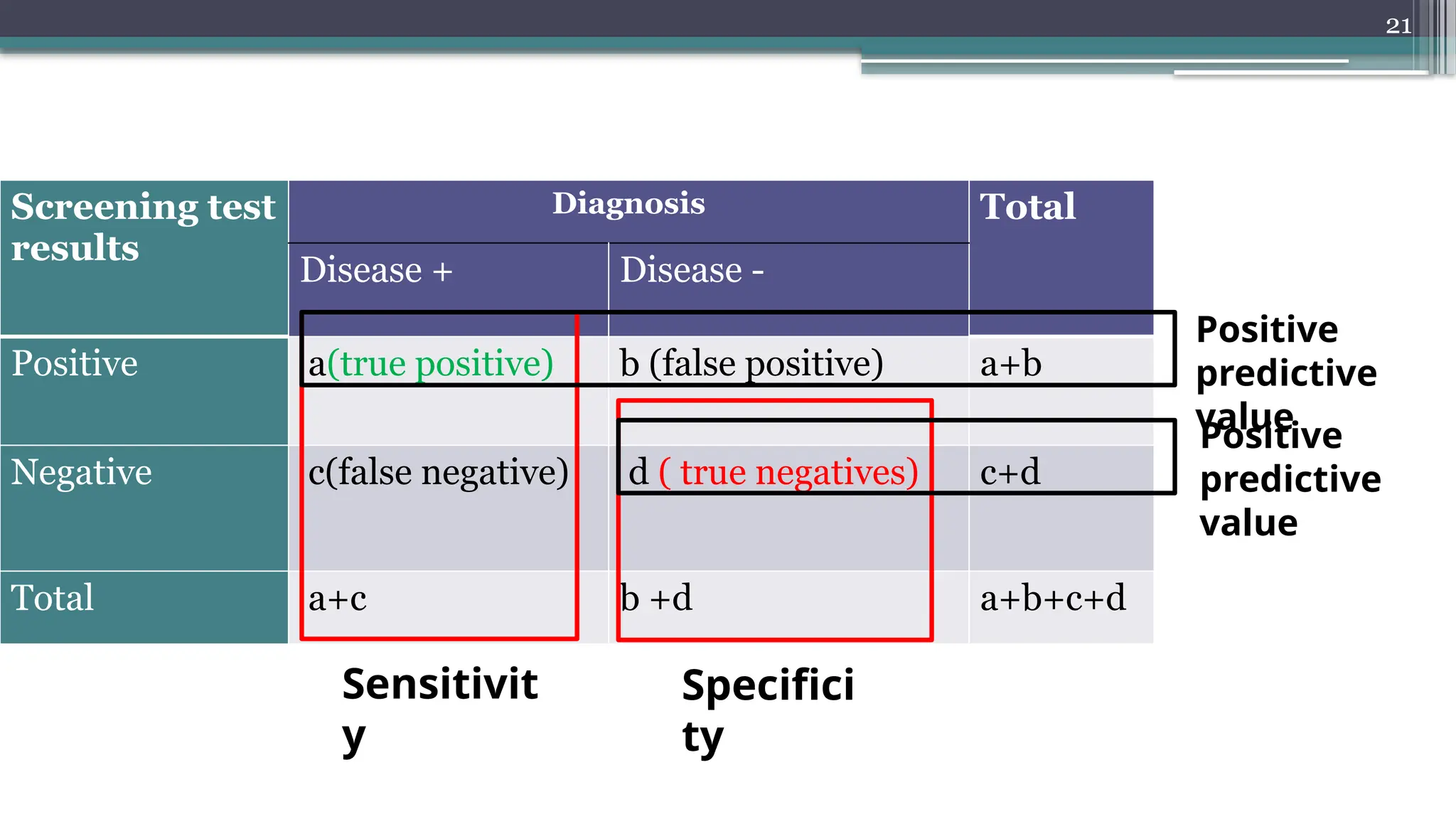
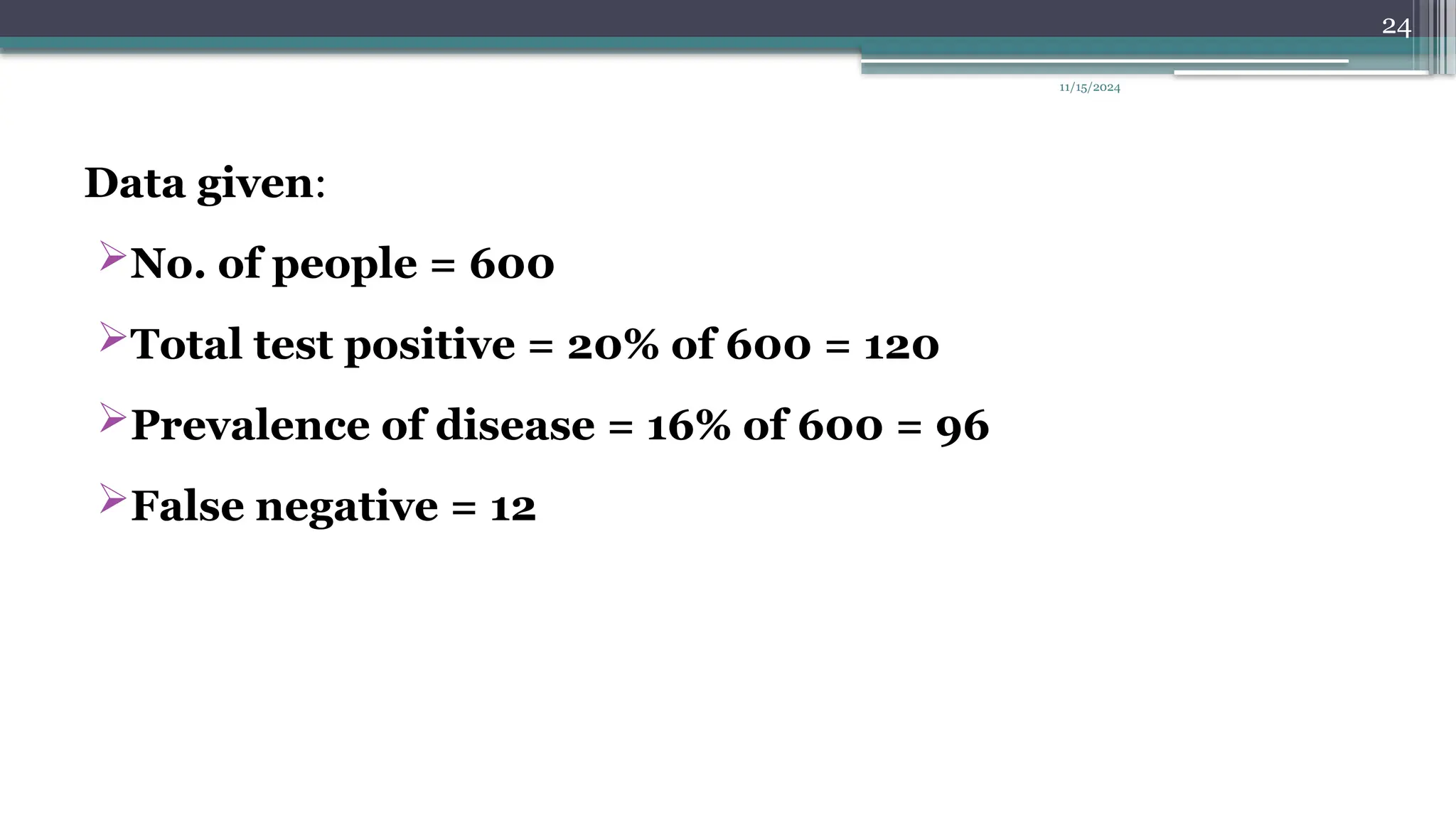
The document discusses the concept of disease screening, emphasizing the difference between screening tests and diagnostic tests, including their definitions, purposes, and criteria for effectiveness. It covers important metrics such as sensitivity, specificity, and predictive values to assess the accuracy of screening tests, along with examples and problems related to breast cancer and diabetes screening. The document concludes with calculations illustrating the application of these principles in practical scenarios.