The document outlines learning objectives and provides information about schizophrenia, including:
- Risk factors include genetic and environmental factors such as family history and obstetric complications.
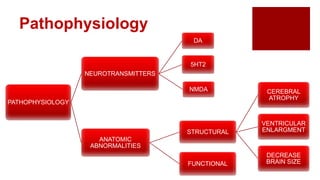
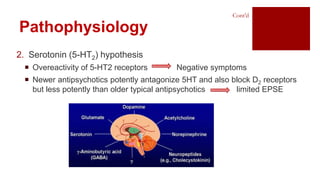
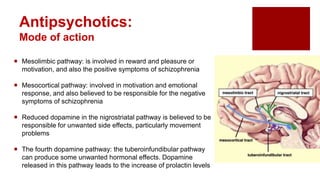
- Pathophysiology may involve dopamine, serotonin, and NMDA receptor abnormalities and structural brain changes.
- Symptoms include positive symptoms like delusions and hallucinations, and negative symptoms such as reduced speech.
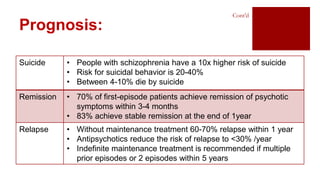
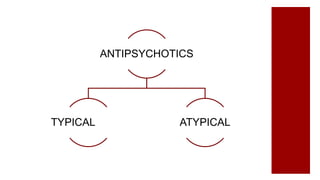
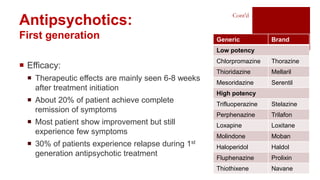
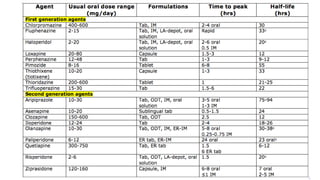
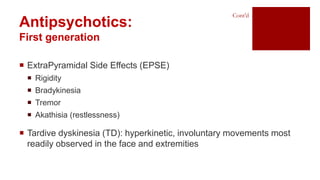
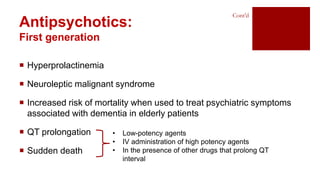
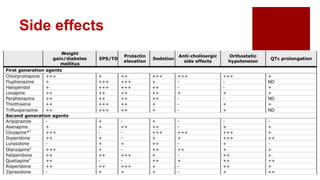
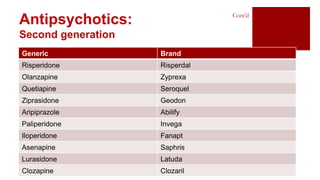
- Treatment involves antipsychotic drugs to reduce positive symptoms as well as managing side effects and preventing relapse.
























![schizophrenia_-final[1]psychiatry courses.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/schizophrenia-final1-241125165758-037ddbda-thumbnail.jpg?width=640&height=640&fit=bounds)






























