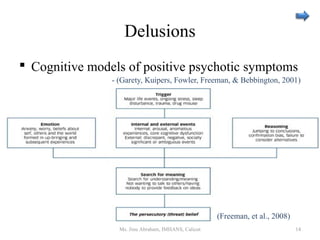
The document provides an overview of recent updates in schizophrenia research from 2008-2014. It summarizes changes in diagnostic classifications like the DSM-V, research on phenomenology such as delusions and hallucinations, epidemiological aspects including global burden and treatment gaps, neurobiological factors like genetics and imaging research, and interventions including early phase treatments and prevention strategies. The presentation outline indicates it will cover these topics in further depth across multiple slides.

![Hallucinations…contd
International Consortium on Hallucination
Research [InCoHR]
– Contribution of disease-related process
– Novel theoretical cognitive framework
– Neurobiological substrates
– Hallucination-related alterations in
neurophysiology
– Review of different treatment options
– (Waters, 2012)
Ms. Jinu Abraham, IMHANS, Calicut 18](https://image.slidesharecdn.com/schizophrenia-150302033832-conversion-gate02/85/Schizophrenia-18-320.jpg)




















































![schizophrenia_-final[1]psychiatry courses.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/schizophrenia-final1-241125165758-037ddbda-thumbnail.jpg?width=640&height=640&fit=bounds)










![Cells and Organs of immune system [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cellsandorgansofimmunesystemautosaved-260123152717-ea0cb261-thumbnail.jpg?width=640&height=640&fit=bounds)













