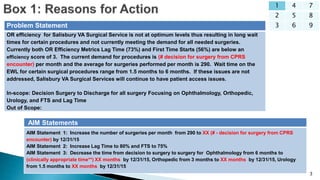
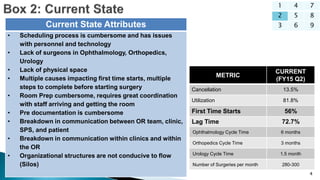
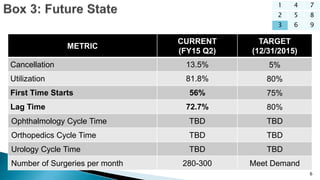
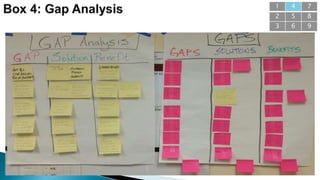
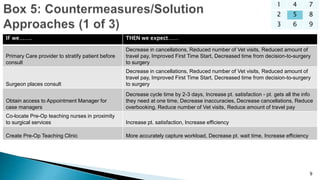
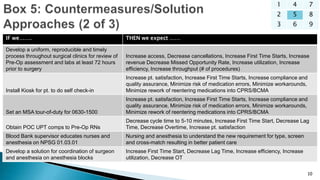
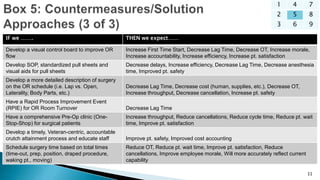
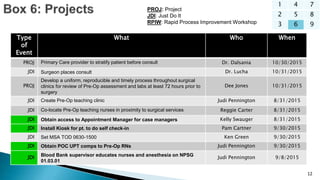
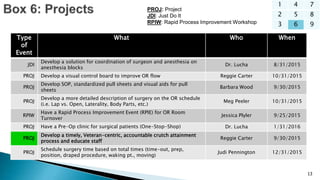
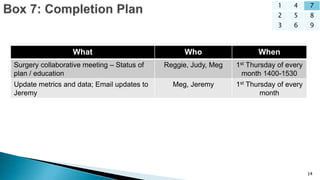
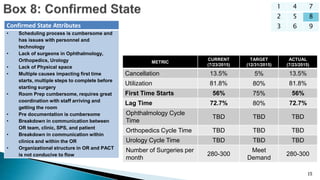
This document outlines a value stream analysis conducted at the Salisbury VA Medical Center from July 21-23, 2015 to improve surgical flow and efficiency. It identifies current metrics, issues, and proposed solutions. The aim is to increase surgeries per month from 290 to meet demand, increase Lag Time to 80% and FTS to 75%, and decrease wait times for select specialties. A series of projects and tests of change are proposed and assigned with target completion dates to address issues like scheduling, pre-op processes, surgeon coordination, and OR flow. Progress will be tracked through monthly meetings and metric updates.

![16
1 4 7
2 5 8
3 6 9
What went well?
• Kept on task.
• Very interactive.
• Good ideas and questions.
• Developed a good vision.
• Saw that it [process] can be better.
• Great team and teamwork.
• Good mix of people, positions and experience.
• Saw leadership being demonstrated.
• Process of VSA and Deep-Dives.
• Mapping identified where major problems / issues were.
• Identified achievable improvements.
• Egos and titles were left at the door.
What could have been
different?
• Use the same room all three days.
• Large enough room.
• Start planning earlier.
• Healthier breakfast options.
• More affected department stakeholders.
• Conduct off-site.
Lessons learned:
• Start planning earlier.
• Get a room reserved for all three days.
• Provide healthier breakfast options.
• Involve more key stakeholders.
• Look into off-site locations for the event.
• Good facilitation is important.
• Staying on track is important.](https://image.slidesharecdn.com/b87f7073-b649-41ab-91f5-608060258299-161209171949/85/Salisbury_VSA_A3_20150721-16-320.jpg)

























































