Download to read offline









![In Indiainthe presenteconomicstatus,itmaynot be practical to establishthe emergencyservicesin
public places and to train the public in the events related to emergency handling by giving related
educationlike insome of the developed countries, but at least in the hospitals which provides the
healthservicesshouldbe readywithall the necessary items in hand to decrease the time between
the onset of emergency and initiation of the treatment to decrease the mortality and morbidity.
Where we can keep these emergency trolleys?
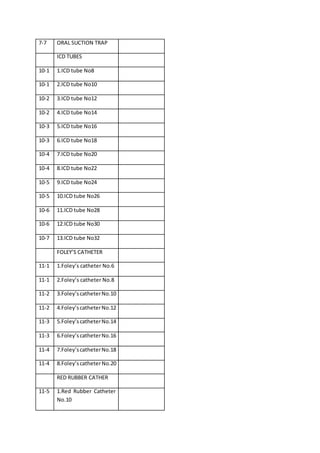
These E trolleys can be maintained in the places like 1.ICU, 2. ICCU, 3.SICU, 4.OT, 5.LABOUR ROOM,
6.PICU, 7.NICU, 8.Emergency ward, 9. Casualty,10. Ambulance.
2.10. Advantages of Emergency Trolley.
What are the advantages of emergency trolley?
The advantages are,
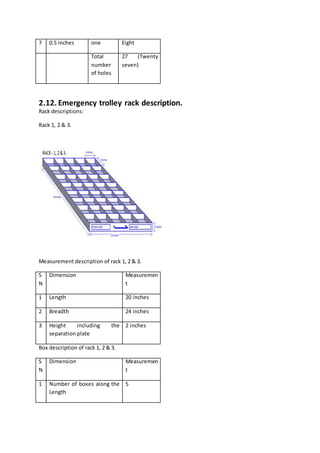
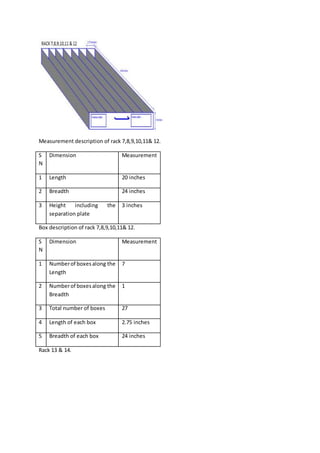
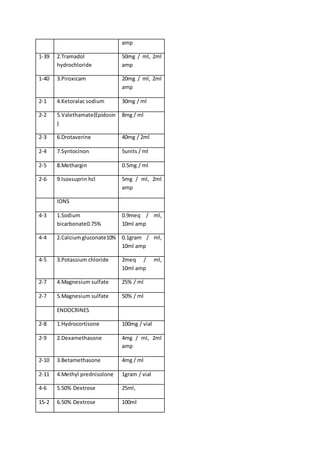
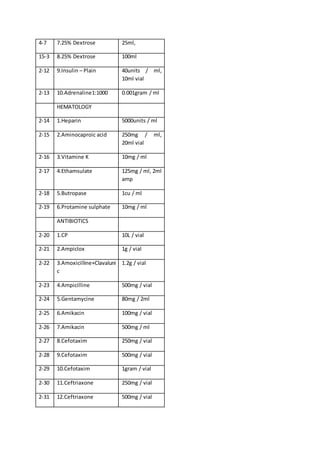
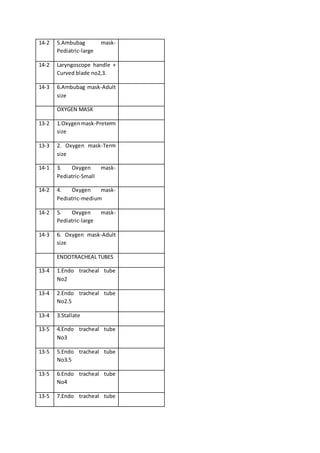
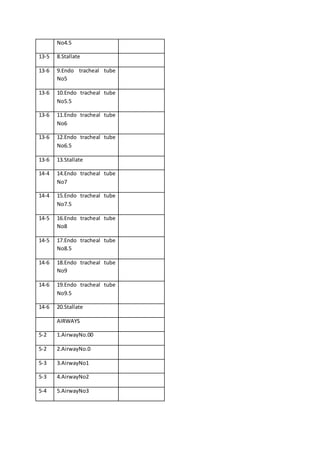
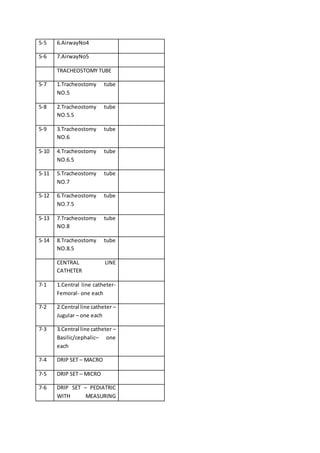
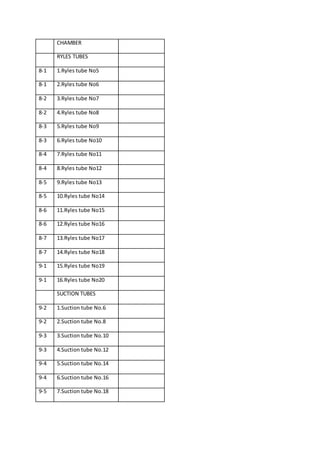
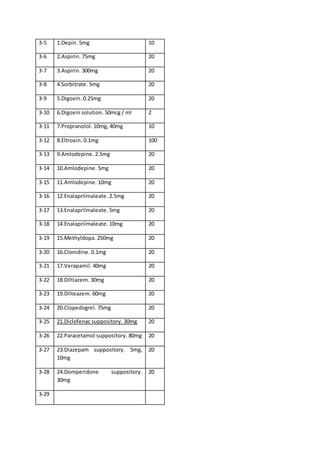
Availability of all the necessary drugs, tubes, monitor, oxygen, defibrillator in one portable small
table measuring 24(Breadth), 42(length), 31(Height) inches;
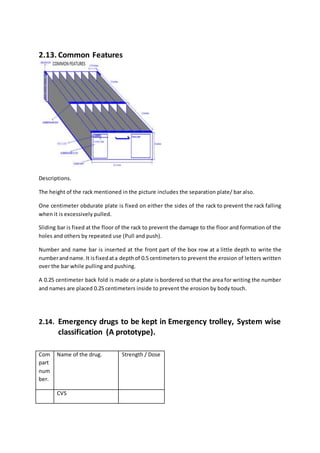
The table can be shifted near the patient and thus it decreases the walking and searching time.
The emptycompartmentwithdesignatedname withoutanymaterial inside will tell the staff to refill
the itemwhichwasutilizedforthe previouspatientandthuswe neednotspendlongtime tolook in
to all the items/ drugs to know what is absent and what is present.
When the administering staff (Doctor/Staff nurse) requests the assisting staff (Staff
nurse/Pharmacist) to load some drug and give, it is easy to search because, we will know which
row/box/compartment has that item and thus it decreases the searching time.
The moneythat we invest to maintain the trolley (towards used items) will decrease the mortality
and the morbidity as it is used in a needy time without writing the prescription to the hospital or
outside pharmacy through the patient attendee. [There may be a delay due to money (some body
may be bringingthe moneyfrom home which may be a far place) or non availability (the pharmacy
might have closed/ stock might have got over)].
At presentall the itemsmaybe presentinthe hospital/drugstore inascatteredway and may not be
available at the needy time due to many reasons like pharmacy time got over, needs permission
fromthe higherofficerforgivingthe stock,the personin charge may be on leave or the key may be
with him and he might have gone for food and thus it leads to the delay. The aim is to get all the
needy items in a composite way at all the time in one table in the places where we handle the
emergencies. If needed, the used items can be replaced by the patient attendee itself at a
convenient time.
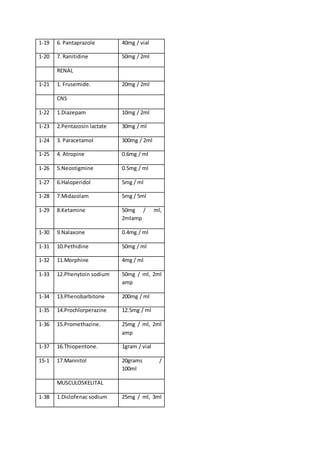
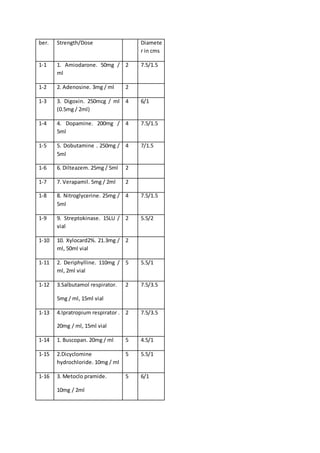
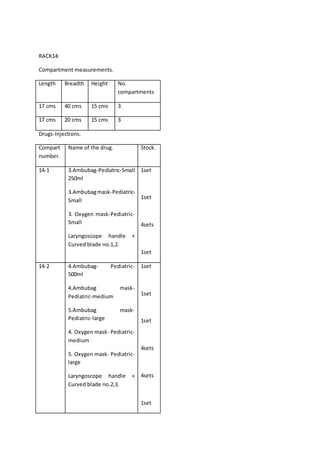
Some time we maynot be maintainingall the itemsatall the places,routinely,like Inj.Streptokinase
inNICU- E – Trolley,where we canputa label like nostockismaintained,butall the necessary drugs
should be replaced immediately.](https://image.slidesharecdn.com/s9c2-chapter2-health-160221075210/85/S9c2-chapter-2-health-12-320.jpg)




























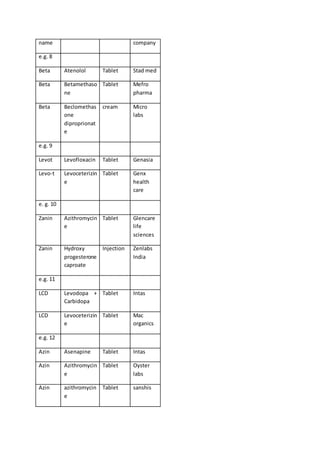



















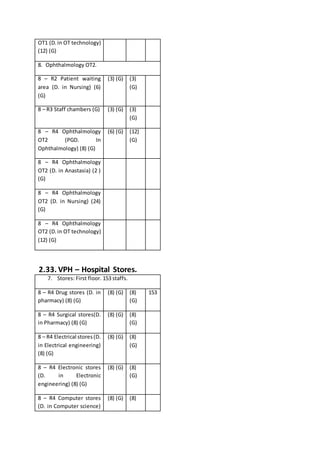
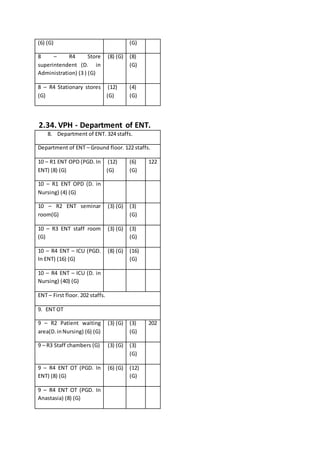
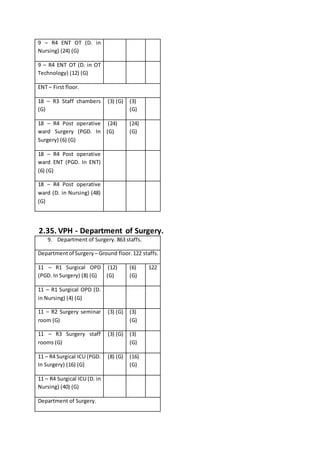
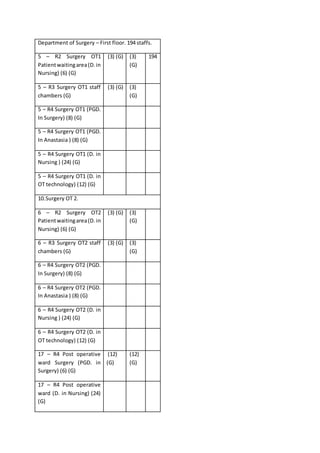






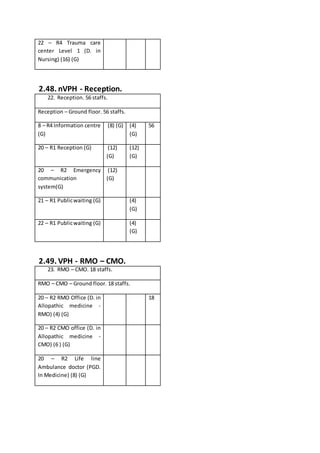




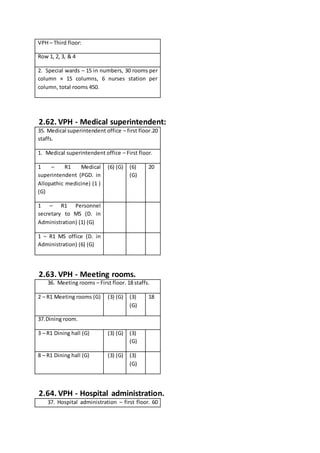





The document discusses various health scenarios, emphasizing the importance of improving healthcare infrastructure, services, and patient management at village health posts (VPH) to ensure better access to care and emergency services. It outlines challenges faced in medical cases, including referrals and availability of specialists and equipment, proposing solutions to streamline healthcare delivery through a coordinated approach. The ultimate goal is to enhance the quality of health services, reduce hospital transfers, and ensure timely treatment for all patients while promoting a healthier society.


















































































