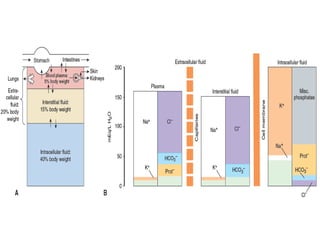
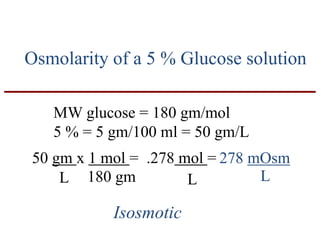
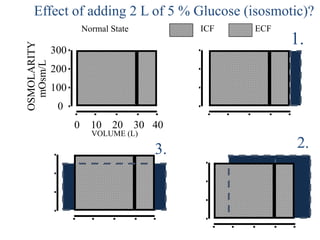
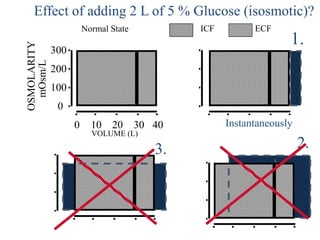
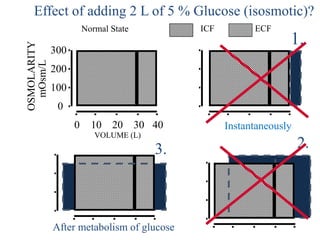
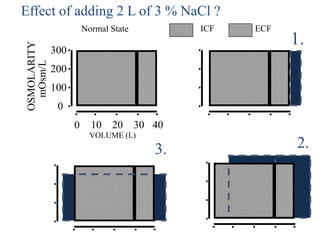
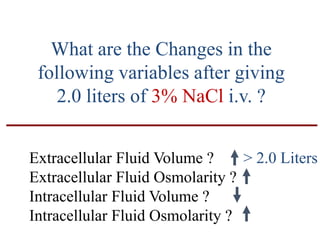
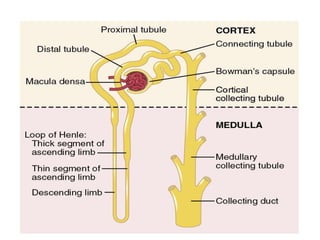
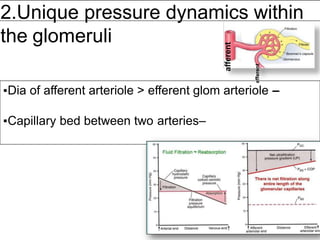
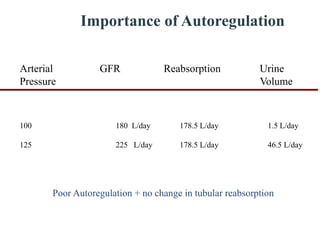
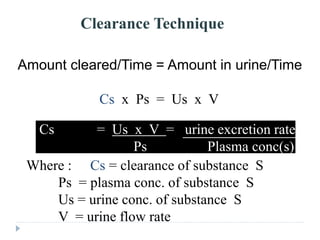
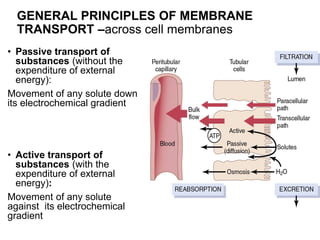
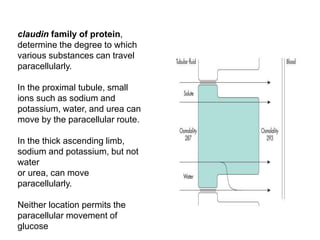
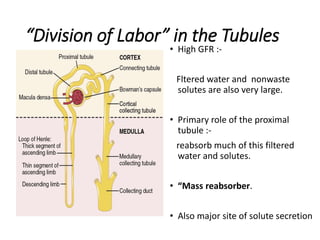
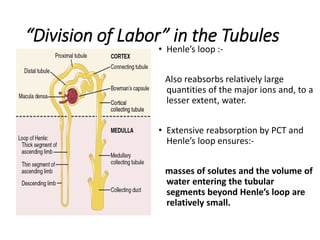
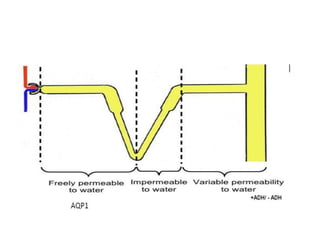
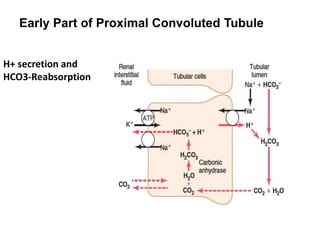
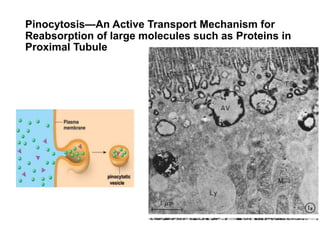
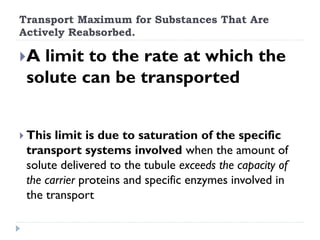
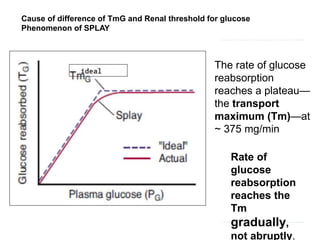
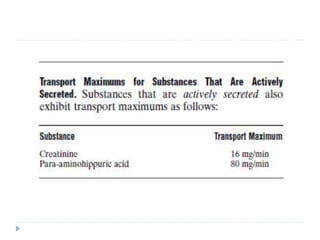
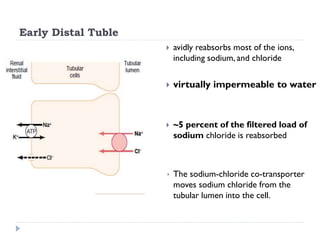
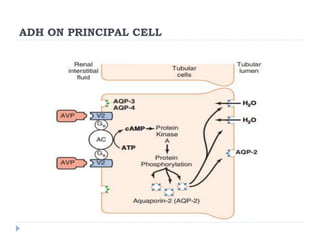
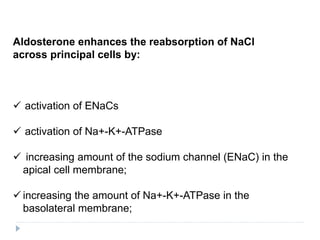
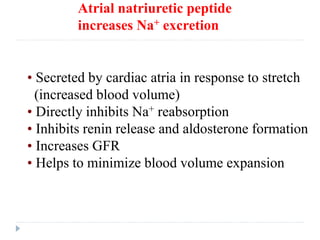
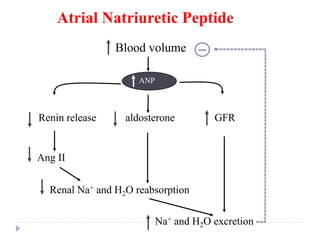
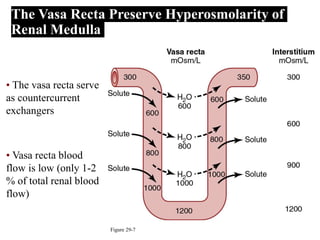
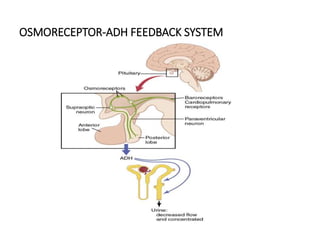
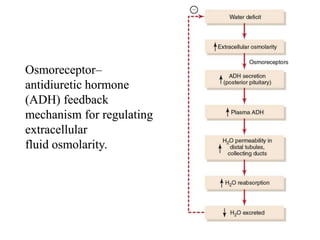
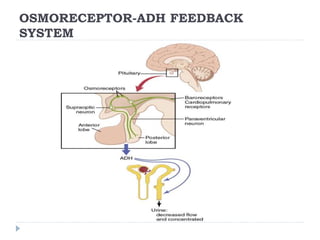
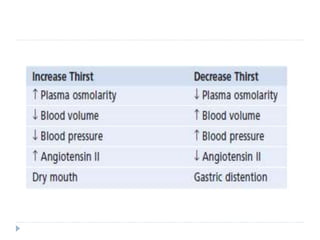
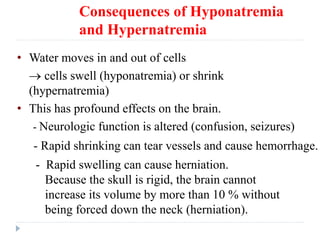
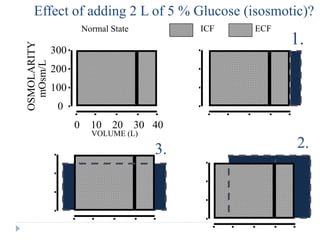
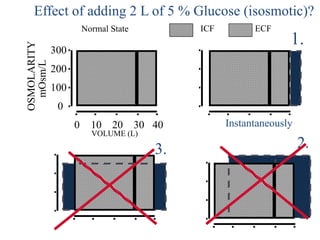
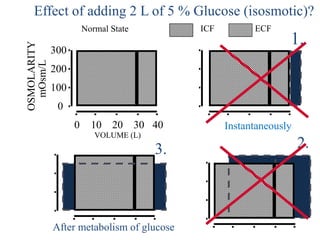
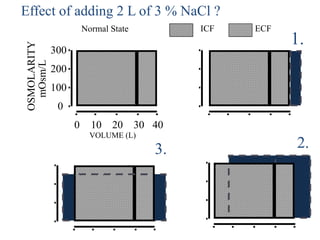
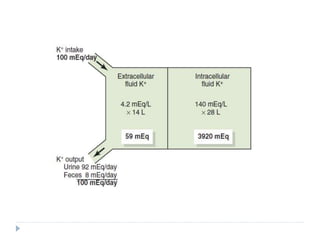
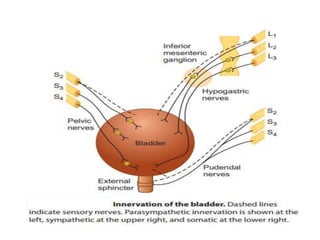
1. The normal osmolality of human plasma is 280-290 mOsm/kg H2O. Osmolality measures the concentration of osmoles per kg of water, while osmolarity measures osmoles per liter of solution.
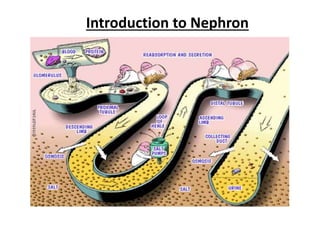
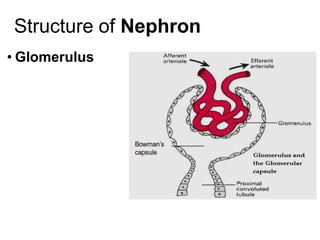
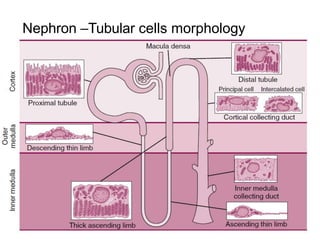
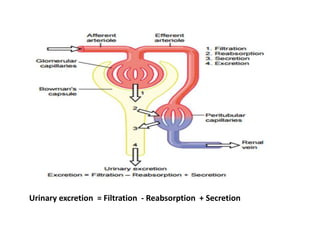
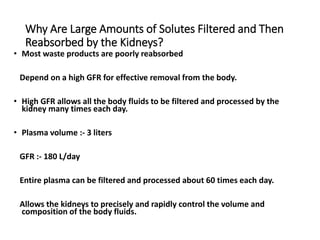
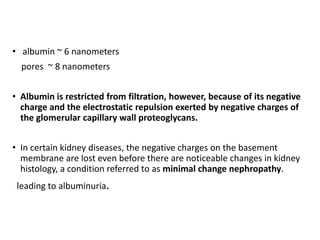
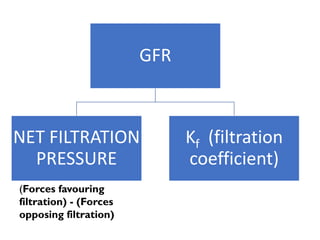
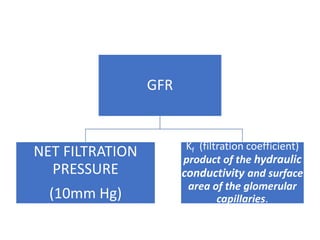
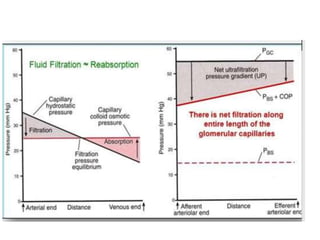
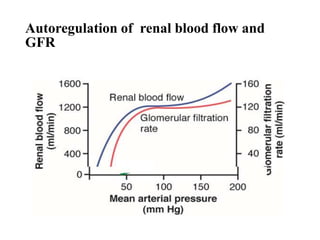
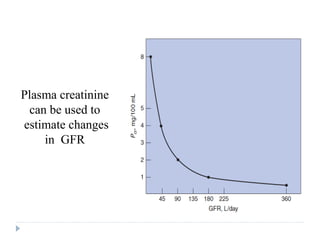
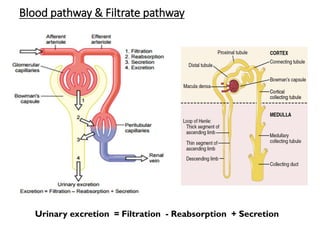
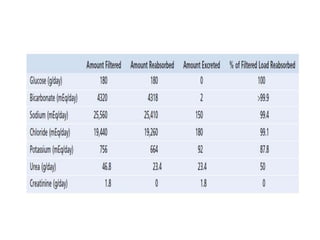
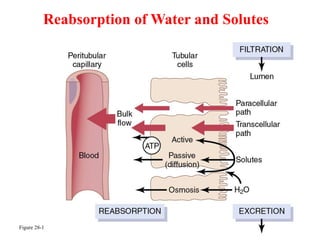
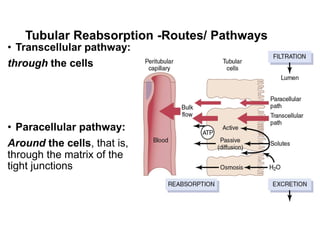
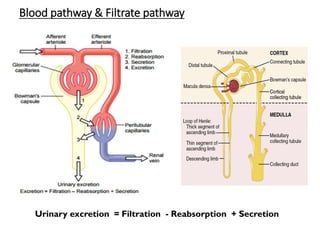
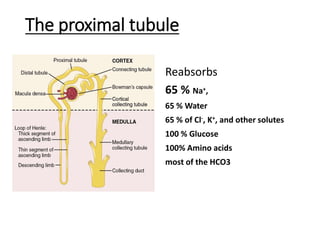
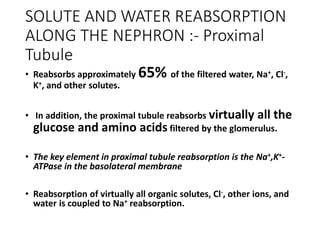
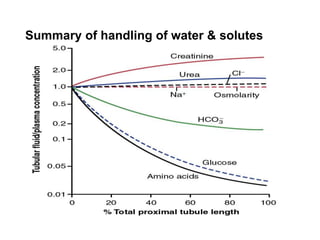
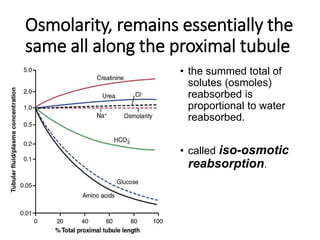
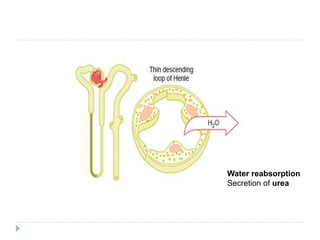
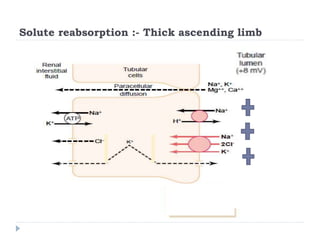
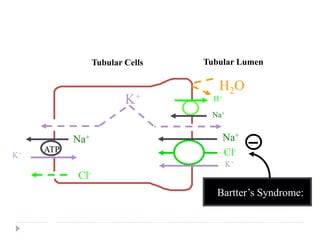
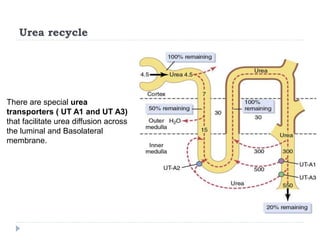
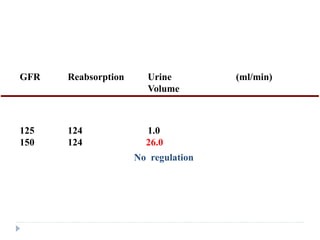
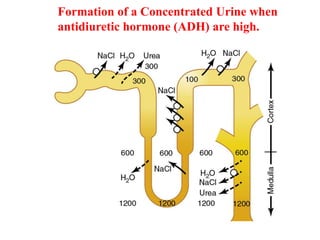
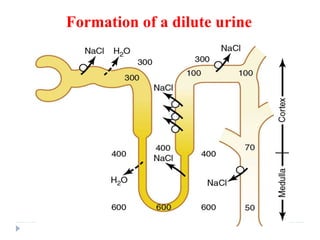
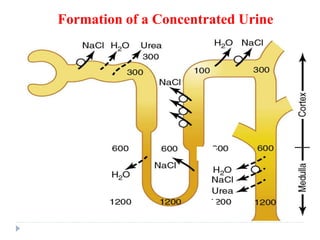
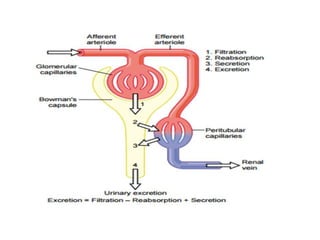
2. Urine formation results from glomerular filtration, tubular reabsorption, and tubular secretion. Most of the fluid, electrolytes, and other substances filtered at the glomerulus are reabsorbed, with only a small amount excreted as urine.
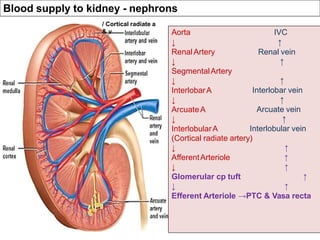
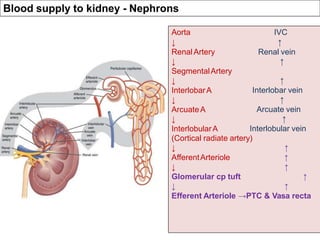
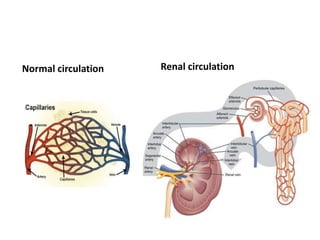
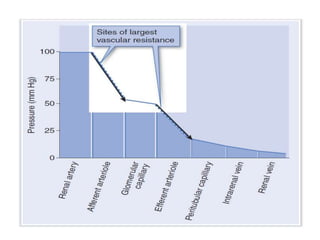
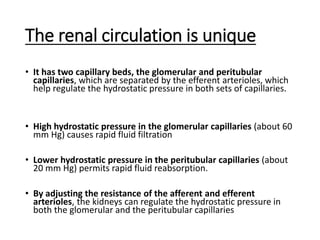
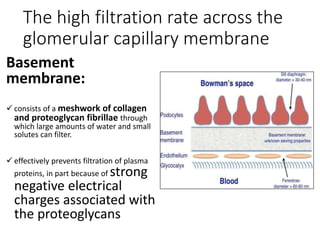
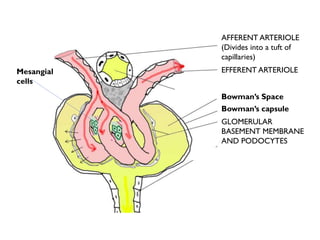
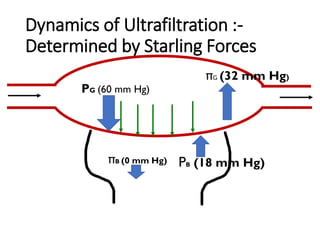
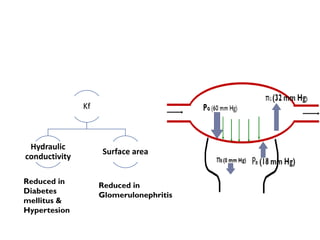
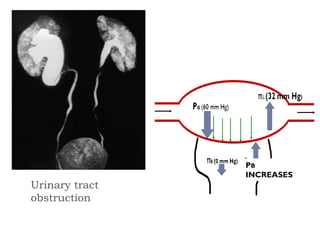
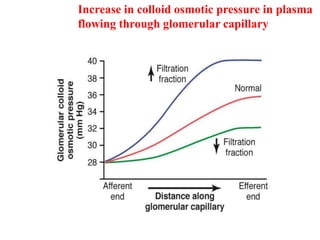
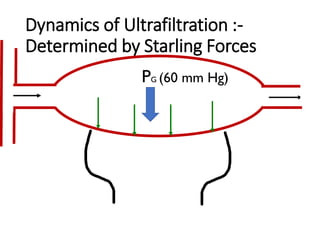
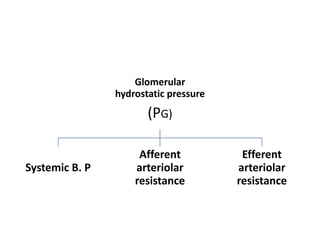
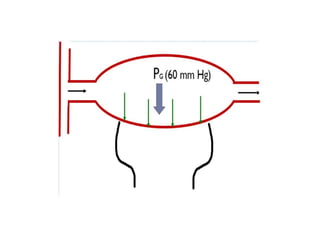
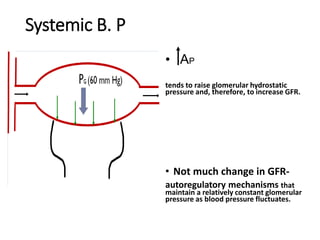
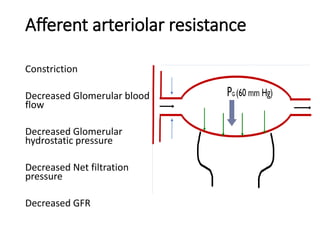
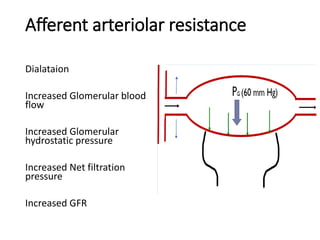
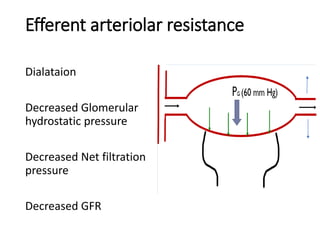
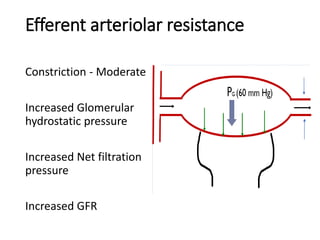
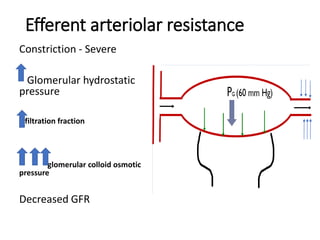
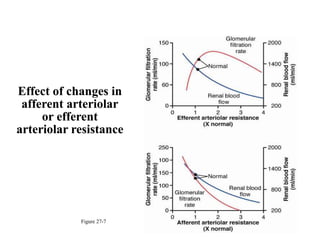
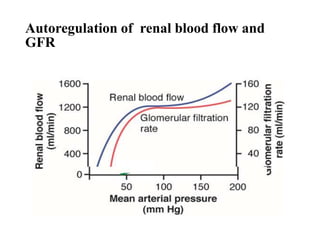
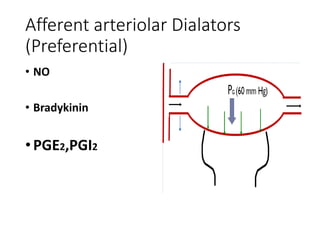
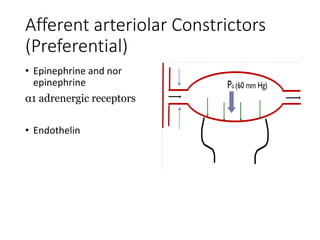
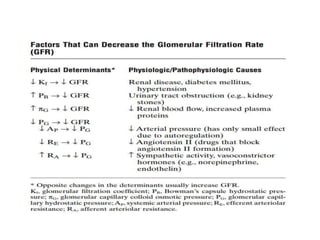
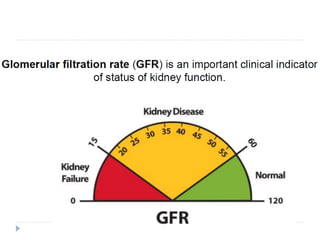
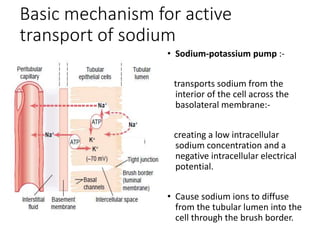
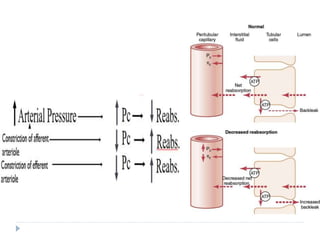
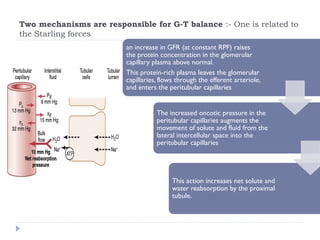
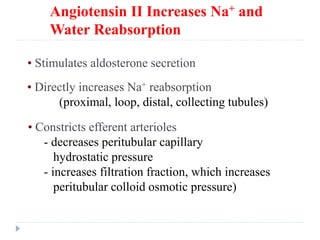
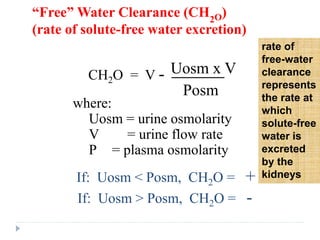
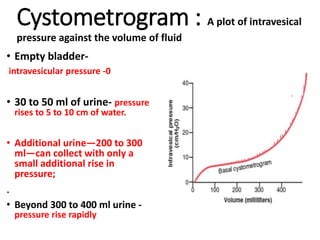
3. The unique renal circulation allows precise regulation of fluid filtration and reabsorption through adjustment of afferent and efferent arteriole resistance and thereby glo
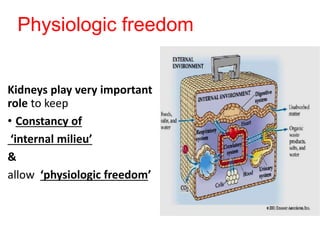

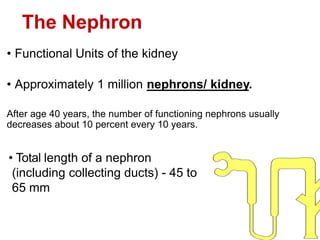
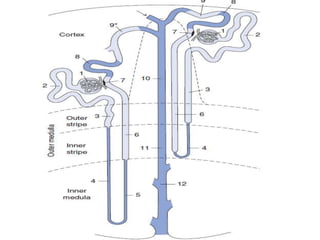

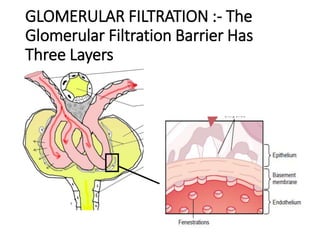
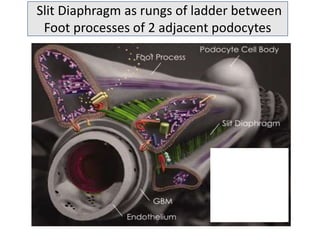
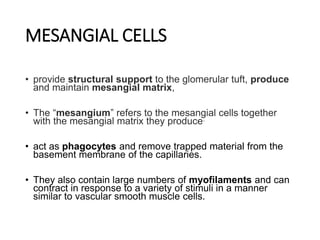
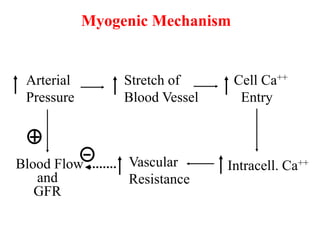
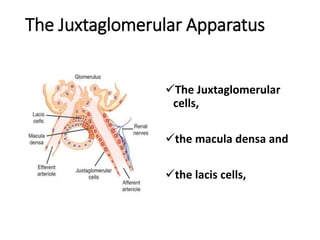

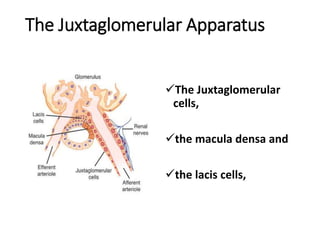
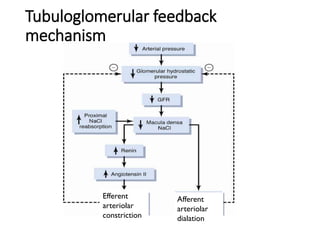
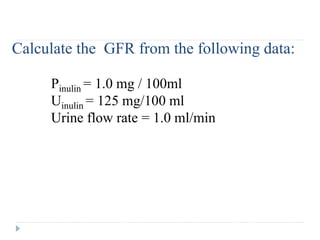
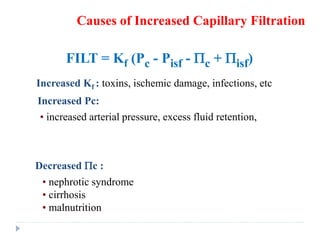
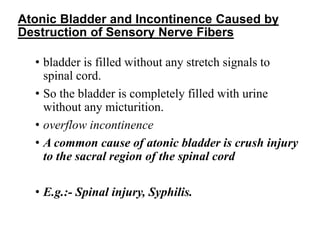
![HOW MACULA DENSA TRIGGERS
CHANGES AFFERENT ARTERIOLAR
RESISTANCE • An increase in the GFR elevates the [NaCl] in
tubule fluid at the macula densa.
• Na+ and Cl– enter the macula densa cells via the Na–
K–2Cl cotransporter
• increased Na, K ATPase activity
• increased ATP hydrolysis causes more adenosine is
formed.
• increase in adenosine triphosphate (ATP) and
adenosine (ADO) release
• ATP and adenosine binds to receptors in the
plasma membrane of smooth muscle cells
surrounding the afferent arteriole
• both of which increase intracellular [Ca++].
• afferent vasoconstriction and a resultant decrease in
GFR.](https://image.slidesharecdn.com/renalphysiolgy-240311050632-89ec092a/85/Renal-Physiolgy-pdf-kidney-and-functions-186-320.jpg)
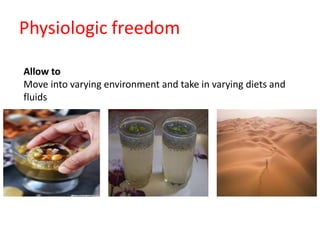
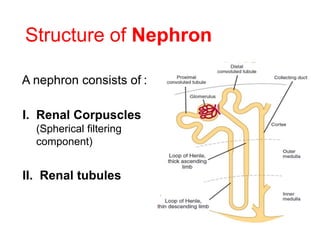
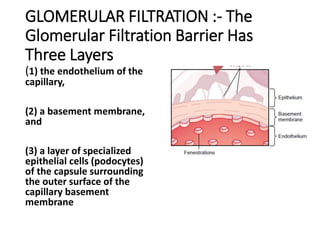
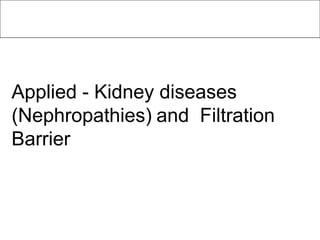
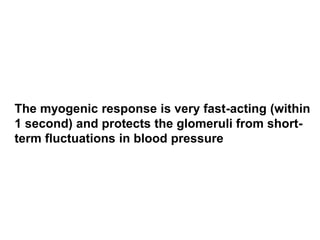
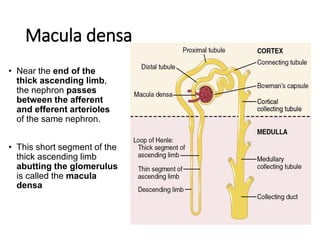
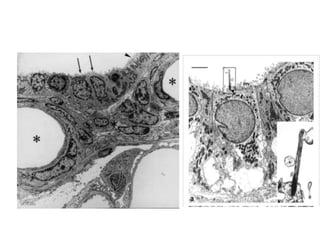
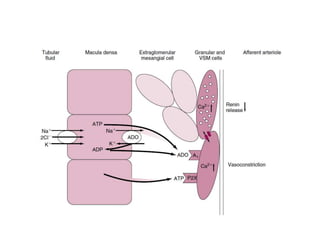
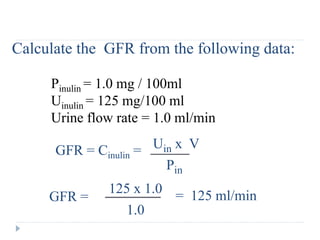
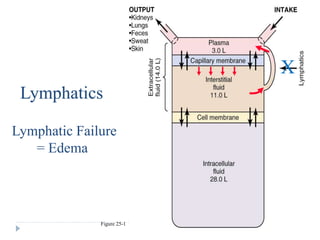
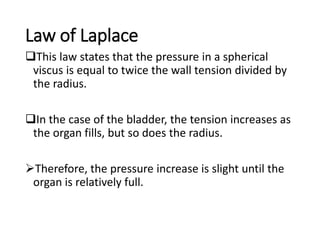
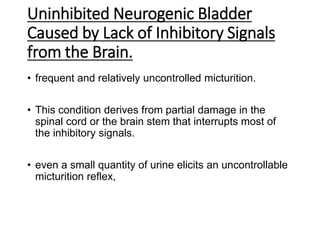
![HOW MACULA DENSA TRIGGERS
CHANGES IN RENIN SECRETION
• that ATP and ADO also inhibit
renin release by granular cells
in the afferent arteriole.
• This action, too, results from
an increase in intracellular
[Ca++], reflecting electrical
coupling of the granular and
vascular smooth muscle
(VSM) cells](https://image.slidesharecdn.com/renalphysiolgy-240311050632-89ec092a/85/Renal-Physiolgy-pdf-kidney-and-functions-187-320.jpg)
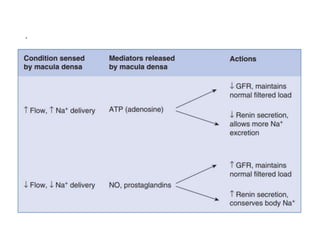
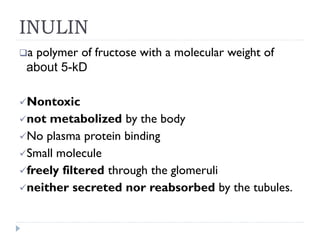
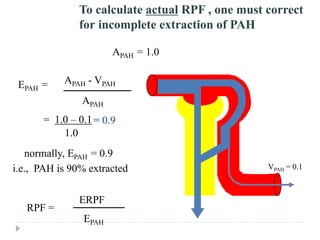
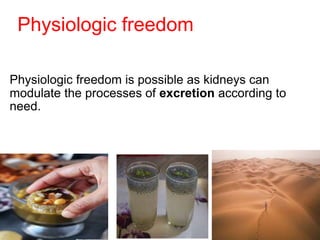
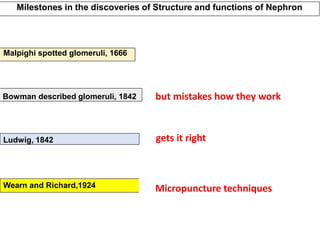
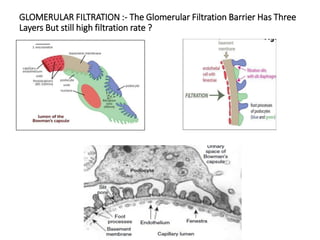
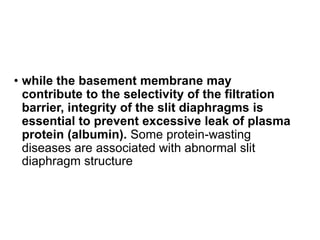
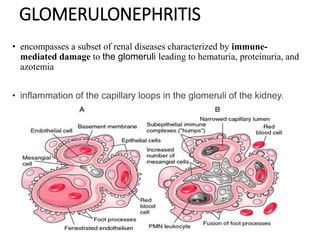
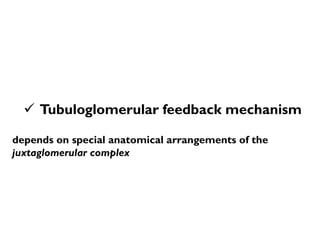
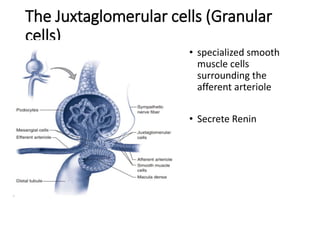
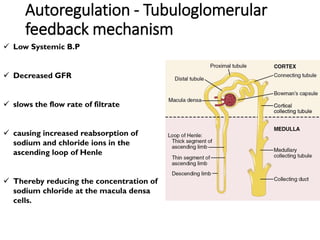
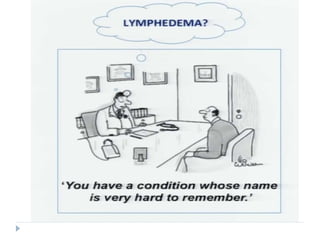
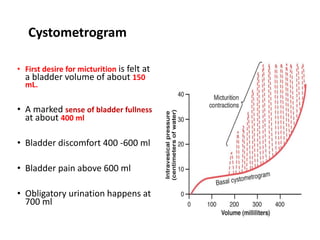
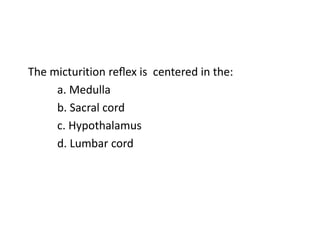
![A patient is infused with paraaminohippuric acid
(PAH) to measure renal blood flow (RBF). She has a
urine flow rate of 1 mL/min, a plasma [PAH] of 1
mg/mL, a urine [PAH] of 600 mg/mL, and a hematocrit
of 45%. What is her “effective” RBF?
(A) 600 mL/min
(B) 660 mL/min
(C) 1091 mL/min
(D) 1333 mL/min](https://image.slidesharecdn.com/renalphysiolgy-240311050632-89ec092a/85/Renal-Physiolgy-pdf-kidney-and-functions-228-320.jpg)
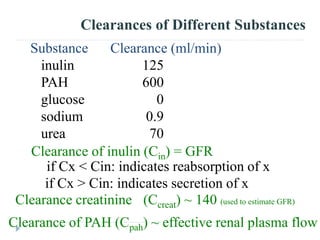
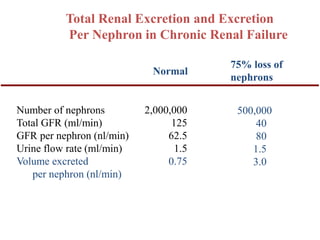
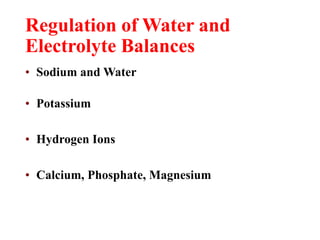
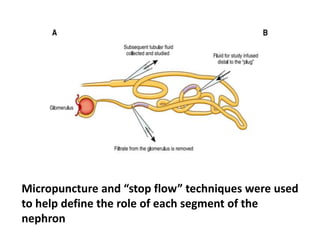
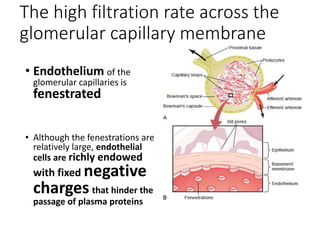
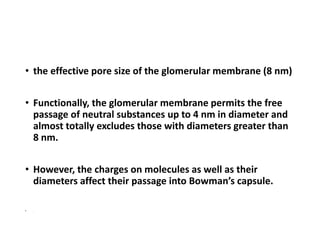
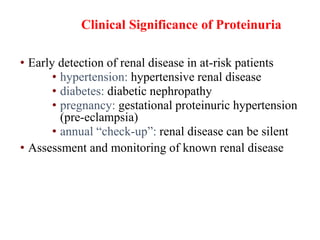
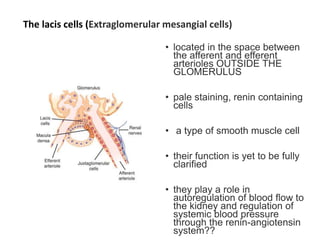
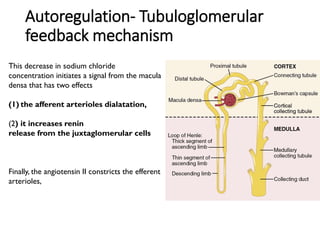
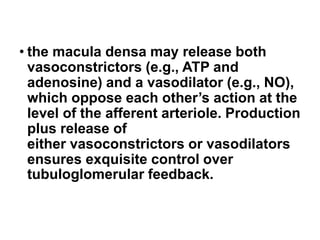
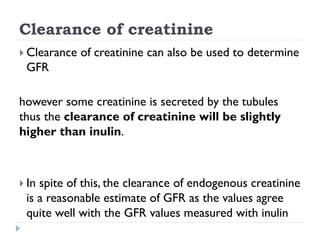
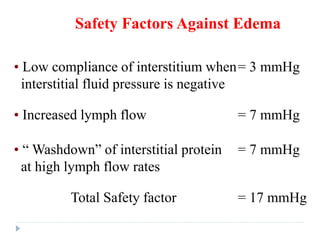
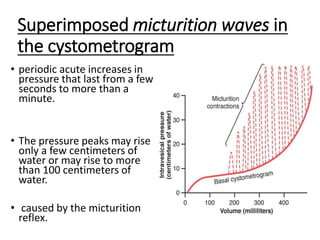
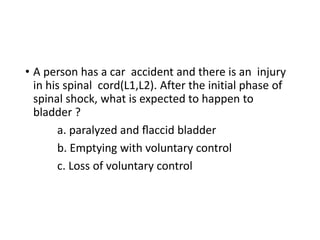
![The following information was obtained in a 20-year-old
college student who was participating in a research study
in the Clinical Research Unit:
Plasma Urine
[Inulin] = 1 mg/mL [Inulin] = 150 mg/mL
[X] = 2 mg/Ml [X] = 100 mg/mL
Urine flow rate = 1
mL/min
Assuming that X is freely filtered, which of the following
statements is most correct?
(A) There is net secretion of X
(B) There is net reabsorption of X
(C) The clearance of X could be used to measure the
glomerular filtration rate (GFR)
(D) The clearance of X is greater than the clearance of](https://image.slidesharecdn.com/renalphysiolgy-240311050632-89ec092a/85/Renal-Physiolgy-pdf-kidney-and-functions-235-320.jpg)
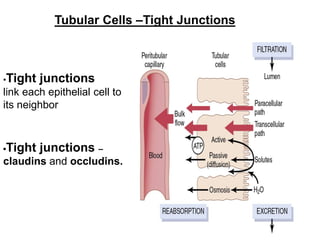



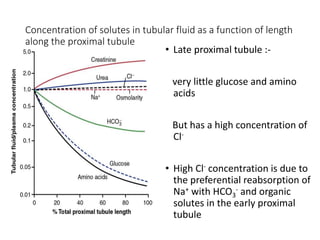
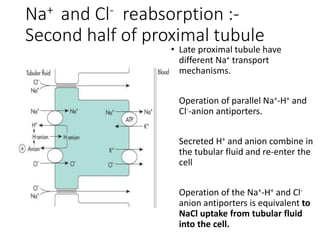
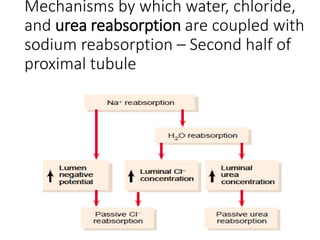
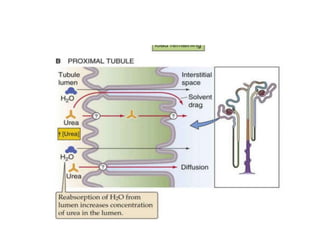
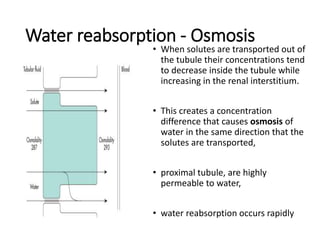
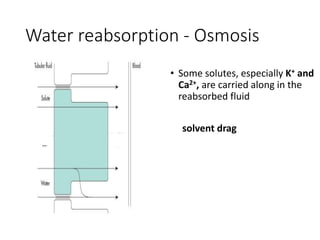
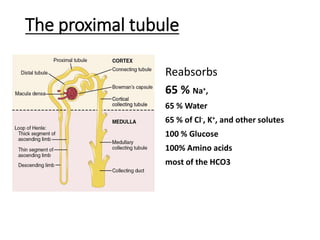
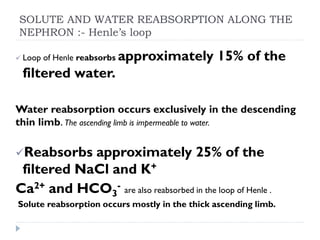
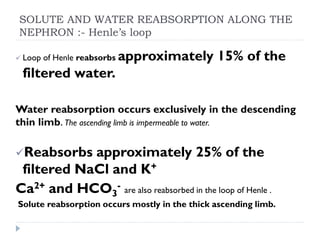
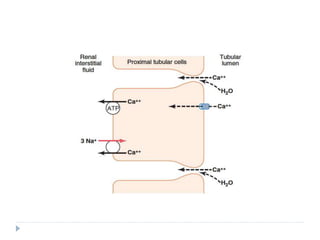
![• Paracellular NaCl reabsorption
Rise in [Cl-] in the tubular fluid in the
early proximal tubule
Diffusion of Cl- from the tubular lumen
across the tight junctions into the
lateral intercellular space.
• Tubular fluid become positively
charged relative to the blood.
• Positive transepithelial voltage causes
the diffusion of Na+ out of the tubular
fluid across the tight junctions.
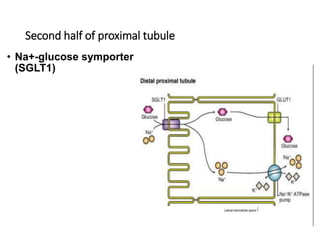
Na+ reabsorption :-Second half of
proximal tubule](https://image.slidesharecdn.com/renalphysiolgy-240311050632-89ec092a/85/Renal-Physiolgy-pdf-kidney-and-functions-273-320.jpg)
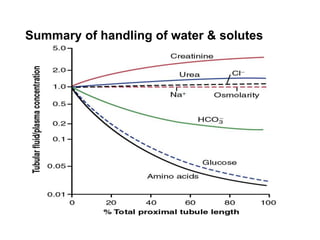
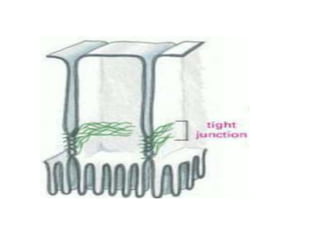
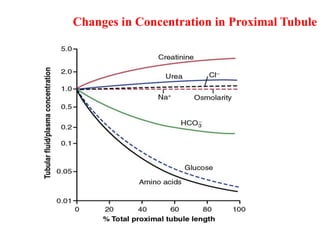
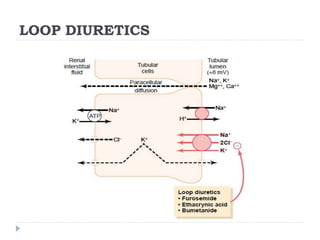
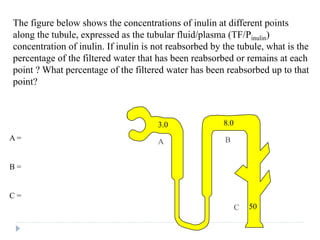
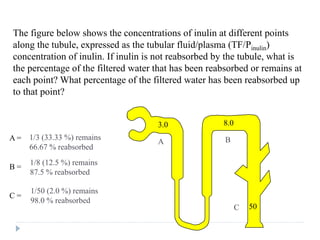
![• [TF/P]x is the concentration of substance X in tubular fluid
relative to the concentration in plasma.](https://image.slidesharecdn.com/renalphysiolgy-240311050632-89ec092a/85/Renal-Physiolgy-pdf-kidney-and-functions-281-320.jpg)
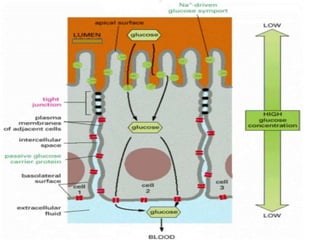
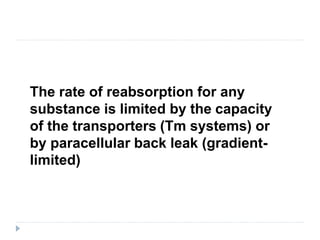
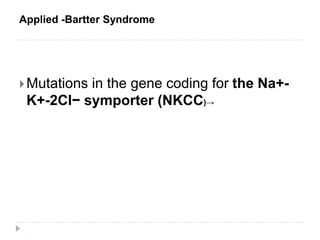
![[TF/P]X = 1.0. X has not been reabsorbed or secreted (all freely
filtered substances in Bowman's space), or X is reabsorbed in
proportion to water (e.g., Na in proximal tubule)
[TF/P]X < 1.0. X is reabsorbed more than water
[TF/P]X > 1.0. X is reabsorbed less than water or X is secreted](https://image.slidesharecdn.com/renalphysiolgy-240311050632-89ec092a/85/Renal-Physiolgy-pdf-kidney-and-functions-282-320.jpg)

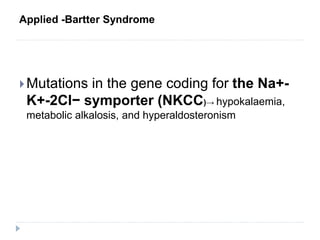
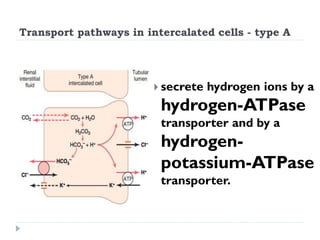
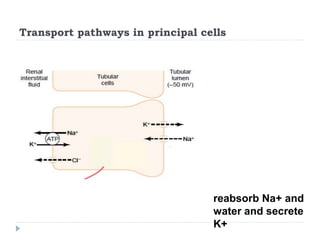
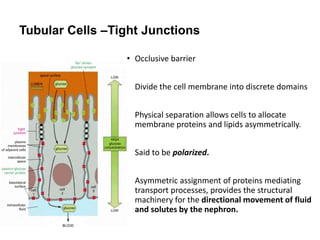
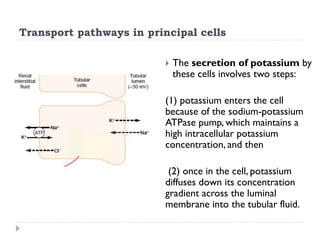
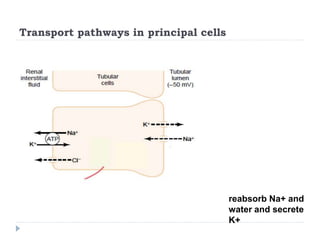
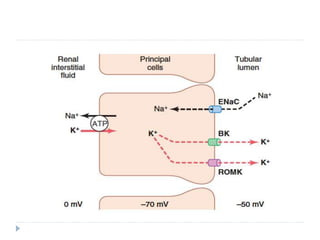
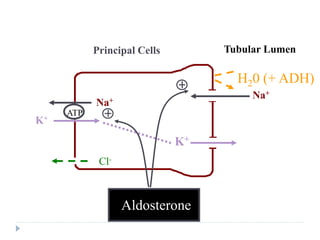
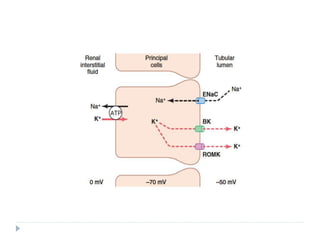
![Transport pathways in principal cells
Sodium reabsorption and
potassium secretion by the
principal cells depend on the
activity of a sodium-
potassium ATPase
pump in each cell’s
basolateral membrane.
This pump maintains a low sodium
concentration inside the cell and,
therefore, favors sodium diffusion
into the cell through special channels
[epithelial Na+-selective
channels (ENaCs)]](https://image.slidesharecdn.com/renalphysiolgy-240311050632-89ec092a/85/Renal-Physiolgy-pdf-kidney-and-functions-345-320.jpg)
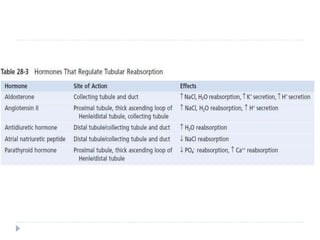
![Control of Ca++ by Parathyroid
Hormone
Extracellular
[Ca++]
PTH
Renal Ca++
Reabsorption
Intestinal Ca++
Reabsorption
Ca++ Release
From Bones
Vitamin D3
Activation](https://image.slidesharecdn.com/renalphysiolgy-240311050632-89ec092a/85/Renal-Physiolgy-pdf-kidney-and-functions-405-320.jpg)
![Estimating Plasma Osmolarity From
Plasma Sodium Concentration
Posm = 2.1 × PNa+ (mmol/L)
Posm = 2 × [PNa+ ,mmol/L] + [Pglucose,mmol/L] + [Purea,mmol/L]](https://image.slidesharecdn.com/renalphysiolgy-240311050632-89ec092a/85/Renal-Physiolgy-pdf-kidney-and-functions-478-320.jpg)




![Swan & Pitts Experiment
Dog received an infusion of 14,000,000
nmoles H+ per litre of body water.
This caused a drop in pH from 7.44 ([H+] = 36
nmoles/l) to a pH of 7.14 ([H+] = 72 nmoles/l)
That is, a rise in [H+] of only 36 nmoles/l.
SO: what had happened to the other 13,999,964
nmoles/l that were infused.
Where did the missing H+ go?
They were hidden on buffers and so these
hydrogen ions were hidden from view.](https://image.slidesharecdn.com/renalphysiolgy-240311050632-89ec092a/85/Renal-Physiolgy-pdf-kidney-and-functions-555-320.jpg)
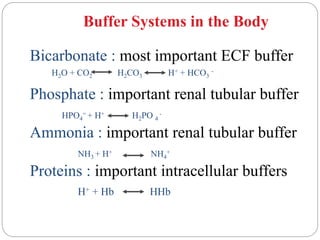
![Mechanisms of Hydrogen Ion
Regulation
[H+] is precisely regulated
(pH range 7.2 - 7.4)
1. Body fluid chemical buffers (rapid but temporary)
- bicarbonate - ammonia
- proteins - phosphate
2. Lungs (rapid, eliminates CO2)
[H+] ventilation CO2 loss
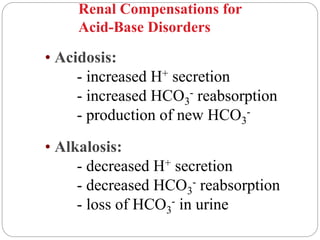
3. Kidneys (slow, powerful); eliminates non-volatile acids
- secretes H+
- reabsorbs HCO3
-
- generates new HCO3
-](https://image.slidesharecdn.com/renalphysiolgy-240311050632-89ec092a/85/Renal-Physiolgy-pdf-kidney-and-functions-557-320.jpg)
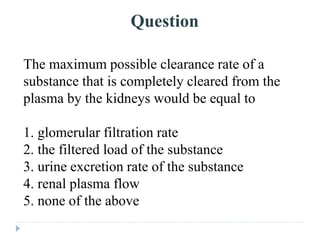
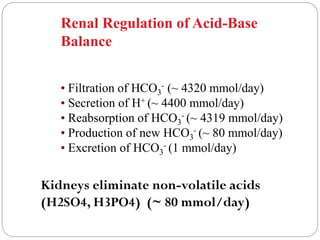
![In a patient with a plasma pH of 7.10, the [HCO3–]/[H2CO3]
ratio in plasma is:
A. 20.
B. 10.
C. 2.
D. 1.
E. 0.1.](https://image.slidesharecdn.com/renalphysiolgy-240311050632-89ec092a/85/Renal-Physiolgy-pdf-kidney-and-functions-562-320.jpg)
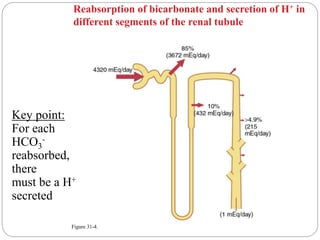
![Mechanisms of Hydrogen Ion
Regulation
[H+] is precisely regulated
(pH range 7.2 - 7.4)
1. Body fluid chemical buffers (rapid but temporary)
- bicarbonate - ammonia
- proteins - phosphate
2. Lungs (rapid, eliminates CO2)
[H+] ventilation CO2 loss
3. Kidneys (slow, powerful); eliminates non-volatile acids
- secretes H+
- reabsorbs HCO3
-
- generates new HCO3
-](https://image.slidesharecdn.com/renalphysiolgy-240311050632-89ec092a/85/Renal-Physiolgy-pdf-kidney-and-functions-563-320.jpg)
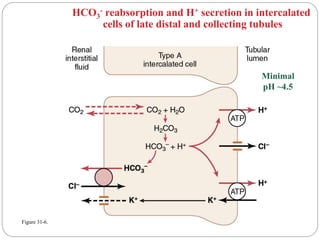
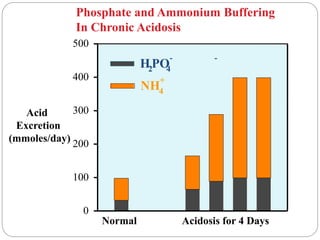
![Minimum urine pH = 4.5
= 10-4.5
= 3 x 10-5 moles/L
i.e., the maximal [H+] of urine is 0.03 mmol/L
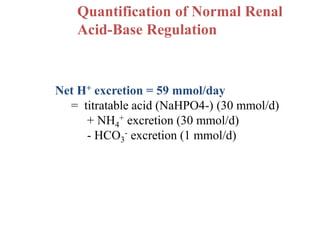
Yet, the kidneys must excrete, under normal
conditions, at least 60 mmol non-volatile acids
each day. To excrete this as free H+ would require:](https://image.slidesharecdn.com/renalphysiolgy-240311050632-89ec092a/85/Renal-Physiolgy-pdf-kidney-and-functions-569-320.jpg)
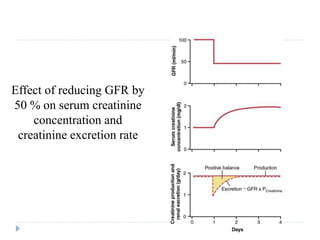
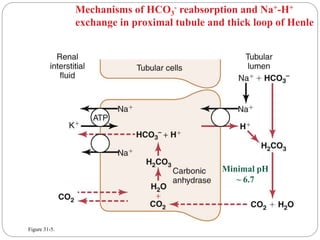
![Minimum urine pH = 4.5
= 10-4.5
= 3 x 10-5 moles/L
i.e., the maximal [H+] of urine is 0.03 mmol/L
Yet, the kidneys must excrete, under normal
conditions, at least 60 mmol non-volatile acids
each day. To excrete this as free H+ would require:
.03mmol/L
= 2000 L per day !!!
60 mmol](https://image.slidesharecdn.com/renalphysiolgy-240311050632-89ec092a/85/Renal-Physiolgy-pdf-kidney-and-functions-570-320.jpg)