Kidney
0 kidneys servemultiple functions, including the following:
1. Excretion of metabolic waste products and foreign chemicals
2. Regulation of water and electrolyte balances
3. Regulation of body electrolyte concentrations
4. Regulation of arterial pressure
5. Regulation of acid-base balance
6. Secretion, metabolism, and excretion of hormones
7. Gluconeogenesis
Lecture notes by Dr. Arham Shabbir
3.
0 Excretion ofMetabolic Waste Products, Foreign
Chemicals, Drugs, and Hormone Metabolites.
0 Eliminate waste products of metabolism that are no longer
needed by the body.
0 Urea (from the metabolism of amino acids)
0 Creatinine (from muscle creatine)
0 Uric acid (from nucleic acids),
0 End products of hemoglobin breakdown (such as bilirubin)
0 Metabolites of various hormones.
0 These waste products must be eliminated from the body as
rapidly as they are produced.
0 Other foreign substances, such as pesticides, drugs, and food
additives etc.
Lecture notes by Dr. Arham Shabbir
4.
Regulation of Waterand Electrolyte Balances:
0 For maintenance of homeostasis, excretion of water and
electrolytes must precisely match intake.
0 If intake exceeds excretion, the amount of that substance in the
body will increase.
0 If intake is less than excretion, the amount of that substance in
the body will decrease.
0 Suppose a sudden 10-fold increase in sodium intake from a low
level of 30 mEq/day to a high level of 300 mEq/day.
0 Within 2 to 3 days after raising the sodium intake, renal
excretion also increases to about 300 mEq/day, so that a balance
between intake and output is re-established.
Lecture notes by Dr. Arham Shabbir
5.
Regulation of ArterialPressure:
0 The kidneys also contribute to short-term arterial pressure
regulation by secreting vasoactive factors or substances, such
as renin, that lead to the formation of vasoactive products
(e.g., angiotensin II).
Regulation of Acid-Base Balance:
0 The kidneys are the only means of eliminating from the body
certain types of acids, such as sulfuric acid and phosphoric
acid, generated by the metabolism of proteins.
Regulation of Erythrocyte Production:
0 The kidneys secrete erythropoietin, which stimulates the
production of red blood cells.
Lecture notes by Dr. Arham Shabbir
6.
0 One importantstimulus for erythropoietin secretion by the
kidneys is hypoxia. The kidneys normally account for almost all
the erythropoietin secreted into the circulation. In people with
severe kidney disease or who have had their kidneys removed
and have been placed on hemodialysis, severe anemia develops
as a result o decreased erythropoietin production.
0 Regulation of 1,25–Dihydroxy vitamin D3 Production
0 The kidneys produce the active form of vitamin D, 1,25-
dihydroxyvitamin, D3 (calcitriol), by hydroxylating this vitamin
at the “number 1” position.
0 Calcitriol is essential for normal calcium deposition in bone.
Lecture notes by Dr. Arham Shabbir
7.
Glucose Synthesis:
0 Thekidneys synthesize glucose from amino acids and other
precursors during prolonged fasting, a process referred to as
gluconeogenesis. The kidneys’ has the capacity to add glucose
to the blood during prolonged periods of fasting.
Lecture notes by Dr. Arham Shabbir
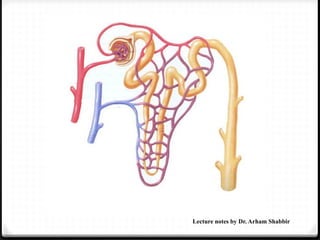
Urine formation
0 Urineformation is a blood cleansing function
0 Normally, about 1300 ml of blood (26% of cardiac output)
enters the kidney.
0 Kidney excretes the unwanted substances along with water
form the blood as urine
0 Normal urinary output is 1L/day to 1.5 L/day
0 Process of urine formation:
0 Urine formation includes processes
0 1- Glomerular filtration
0 2- tubular reabsorption
0 3- Tubular secretion
Lecture notes by Dr. Arham Shabbir
11.
Glomerular filtration
0 Processof glomerular filtration:
0 Urine formation begins when a large amount of fluid is
filtered from the glomerular capillaries into Bowman’s
capsule.
0 Most substances in the plasma, except for proteins, are freely
filtered, so that their concentration in the glomerular filtrate
in Bowman’s capsule is almost the same as in the plasma.
0 Ultrafiltration:
0 Glomerular filtration is called ultrafiltration because even
the minute particles are filtered but plasma proteins are not
filtered due to large molecular size.
0 The protein molecules are larger than the pores present in
endothelium of capillaries.
Lecture notes by Dr. Arham Shabbir
12.
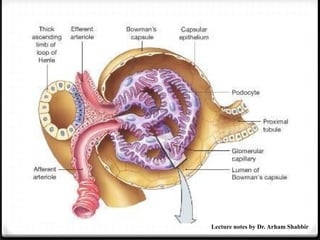
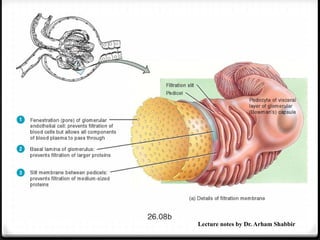
0 Filtration membrane:
0The glomerular capillary membrane is similar to that of other
capillaries, except that it has three (instead of the usual two)
major layers:
0 (1) the endothelium of the capillary,
0 (2) a basement membrane,
0 3) a layer of epithelial cells (podocytes) surrounding the outer
surface of the capillary basement membrane.
0 Together, these layers make up the filtration barrier.
Lecture notes by Dr. Arham Shabbir
13.
0 The capillaryendothelium is perforated by thousands of
small holes called fenestrae. Although the fenestrations are
relatively large, endothelial cells are rich in negative charges
that hinder the passage of plasma proteins.
Lecture notes by Dr. Arham Shabbir
0 GFR
0 Glomerularfiltration rate (GFR) is the volume of fluid filtered
from the renal glomerular capillaries into the Bowman‘s
capsule per unit time.
0 Composition of the Glomerular Filtrate
0 Urine formation begins with filtration of large amounts of
fluid through the glomerular capillaries into Bowman’s
capsule.
0 Like most capillaries, the glomerular capillaries are relatively
impermeable to proteins, so that the filtered fluid (called the
glomerular filtrate) is essentially protein-free and devoid of
cellular elements, including red blood cells.
Lecture notes by Dr. Arham Shabbir
17.
0 The concentrationsof other constituents of the glomerular
filtrate, including most salts and organic molecules, are
similar to the concentrations in the plasma.
0 Exceptions to this generalization include a few low-molecular-
weight substances, such as calcium and fatty acids, that are
not freely filtered because they are partially bound to the
plasma proteins.
0 Almost one half of the plasma calcium and most of the plasma
fatty acids are bound to proteins, and these bound portions
are not filtered through the glomerular capillaries.
0 In the average adult human, the GFR is about 125 ml/min, or
180 L/day.
Lecture notes by Dr. Arham Shabbir
18.
0 Filterability ofSolutes Is Inversely Related to Their Size.
0 A filterability of 1.0 means that the substance is filtered as
freely as water; a filterability of 0.75 means that the substance
is filtered only 75 per cent as rapidly as water. Note that
electrolytes such as sodium and small organic compounds
such as glucose are freely filtered. As the molecular weight of
the molecule approaches that of albumin, the filterability
rapidly decreases, approaching zero.
Lecture notes by Dr. Arham Shabbir
19.
0 Negatively ChargedLarge Molecules Are Filtered Less
Easily Than Positively Charged Molecules of Equal
Molecular Size.
0 The molecular diameter of the plasma protein albumin is
only about 6 nanometers, whereas the pores of the
glomerular membrane are thought to be about 8 nanometers.
Albumin is restricted from filtration, however, because of its
negative charge and the electrostatic repulsion exerted by
negative charges of the glomerular capillary wall
proteoglycans.
Lecture notes by Dr. Arham Shabbir
20.
0 Glomerular capillarypressure:
0 The GFR is determined by (1) the sum of the hydrostatic and
colloid osmotic forces across the glomerular membrane, which
gives the net filtration pressure, and (2) the glomerular capillary
filtration coefficient, Kf.
0 Expressed mathematically, the GFR equals the product of Kf and
the net filtration pressure:
0 GFR = Kf ⨯ Net filtration pressure
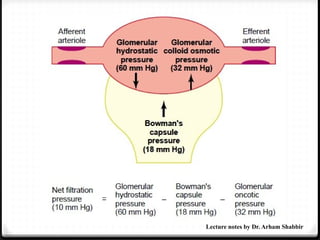
0 Net filtration pressure:
0 The net filtration pressure represents the sum of the hydrostatic
and colloid osmotic forces that either favor or oppose filtration
across the glomerular capillaries.
0 These forces include (1) hydrostatic pressure inside the
glomerular capillaries (glomerular hydrostatic pressure, PG),
which promotes filtration.
Lecture notes by Dr. Arham Shabbir
21.
0 (2) thehydrostatic pressure in Bowman’s capsule (PB)
outside the capillaries, which opposes filtration
0 (3) The colloid osmotic pressure of the glomerular capillary
plasma proteins (πG), which opposes filtration.
0 (4) the colloid osmotic pressure of the proteins in Bowman’s
capsule (πB), which promotes filtration. (Under normal
conditions, the concentration of protein in the glomerular
filtrate is so low that the colloid osmotic pressure of the
Bowman’s capsule fluid is considered to be zero.
Lecture notes by Dr. Arham Shabbir
0 Filtration coefficient:
0The GFR can therefore be expressed as
0 GFR = Kf (P
⨯ G – PB – πG + πB)
0 Kf = GFR/Net filtration pressure
0 125 / 10 = 12.5 ml/min/mm (normal Kf value).
Lecture notes by Dr. Arham Shabbir
24.
0 Physiological controlof GFR:
0 Sympathetic Nervous System activation Decreases GFR
0 Strong activation of the renal sympathetic nerves can constrict
the renal arterioles and decrease renal blood flow and GFR.
0 The renal sympathetic nerves seem to be most important in
reducing GFR during severe, acute disturbances lasting for a
few minutes to a few hours, such as brain ischemia, or severe
hemorrhage.
0 In the healthy resting person, sympathetic tone appears to
have little influence on renal blood flow.
Lecture notes by Dr. Arham Shabbir
25.
Hormonal and AutacoidControl of Renal Circulation:
0 Epinephrine, and Endothelin Constrict Renal Blood
Vessels and Decrease GFR.
0 Hormones that constrict afferent and efferent arterioles,
causing reductions in GFR and renal blood flow, include
norepinephrine and epinephrine released from the adrenal
medulla.
0 Another vasoconstrictor, endothelin, is a peptide that can be
released by damaged vascular endothelial cells of the kidneys
as well as by other tissues. The physiologic role of this
autacoid is not completely understood. However, endothelin
may contribute to hemostasis (minimizing blood loss) when a
blood vessel is severed,
Lecture notes by Dr. Arham Shabbir
26.
0 Angiotensin IIConstricts Efferent Arterioles.
0 A powerful renal vasoconstrictor, angiotensin II, Because
angiotensin II preferentially constricts efferent arterioles, increased
angiotensin II levels raise glomerular hydrostatic pressure.
0 If blood pressure drops then GFR also drops, due to reduced blood
flow through the kidneys. To restore homeostasis, contraction of the
efferent arteriole occurs in response to angiotensin II and the
pressure difference between the afferent and efferent arterioles
increases, creating greater filtration pressure.
0 Therefore, when blood pressure falls, there is minimum alteration of
GFR.
Lecture notes by Dr. Arham Shabbir
27.
0 Endothelial-Derived NitricOxide Decreases Renal
Vascular Resistance and Increases GFR:
0 A basal level of nitric oxide production appears to be
important for maintaining vasodilation of the kidneys. This
allows the kidneys to excrete normal amounts of sodium and
water.
0 Therefore, administration of drugs that inhibit this normal
formation of nitric oxide increases renal vascular resistance
and decreases GFR and urinary sodium excretion, eventually
causing high blood pressure.
Lecture notes by Dr. Arham Shabbir
28.
0 Prostaglandins andBradykinin Tend to Increase GFR.
Hormones and autacoids that cause vasodilation and increased
renal blood flow and GFR include the prostaglandins (PGE2 and
PGI2) and bradykinin.
0 Although these vasodilators do not appear to be of major
importance in regulating renal blood flow or GFR in normal
conditions, they may dampen the renal vasoconstrictor effects
of the sympathetic nerves, especially their effects to constrict
the afferent arterioles.
0 By opposing vasoconstriction of afferent arterioles, the
prostaglandins may help prevent excessive reductions in GFR
and renal blood flow. Under stressful conditions, such as
volume depletion or after surgery, the administration of
nonsteroidal anti-inflammatory agents, such as aspirin, that
inhibit prostaglandin synthesis may cause significant
reductions in GFR Lecture notes by Dr. Arham Shabbir
29.
0 High ProteinIntake and Increased Blood Glucose:
0 A high protein intake is known to increase both renal blood
flow and GFR.
0 A high-protein meal increases the release of amino acids into
the blood, which are reabsorbed in the proximal tubule.
Because amino acids and sodium are reabsorbed together by
the proximal tubules, increased amino acid reabsorption also
stimulates sodium reabsorption in the proximal tubules. This
decreases sodium delivery to the macula densa. Thus body
senses that sodium is more conserved in the body and it
increases GFR by decreasing afferent arteriolar resistance and
raising renal blood flow to excrete more sodium.
Lecture notes by Dr. Arham Shabbir
30.
0 A similarmechanism may also explain the marked increases
in renal blood flow and GFR that occur with large increases in
blood glucose levels in uncontrolled diabetes mellitus.
Lecture notes by Dr. Arham Shabbir
31.
0 Micturition:
0 Micturitionis the process by which the urinary bladder
empties when it becomes filled.
0 This involves two main steps: First, the bladder fills
progressively until the tension in its walls rises above a
threshold level.
0 This elicits the second step, which is a nervous reflex called
the micturition reflex that empties the bladder or, if this fails,
at least causes a conscious desire to urinate.
0 Although the micturition reflex is an autonomic spinal cord
reflex, it can also be inhibited or facilitated by centers in the
cerebral cortex or brain stem
Lecture notes by Dr. Arham Shabbir
32.
Tubular Reabsorption
0 Itis the process by which water and other substances are
transported from renal tubules back to the blood.
0 Selective reabsorption:
0 Tubular reabsorption is known as selective reabsorption
because the tubular cells reabsorb only the substances
necessary for the body
0 Essential substances such as amino acids and vitamins are
completely reabsorbed from renal tubules.
0 Whereas, the unwanted substances like metabolic waste
products are not reabsorbed and excreted through urine.
Lecture notes by Dr. Arham Shabbir
33.
Mechanism of reabsorption
0Active reabsorption
0 Passive reabsorption
0 Active reabsorption:
0 Movement of molecules against concentration gradient
0 It requires energy (ATP)
0 Substances which reabsorb actively from renal tubule are:
0 Sodium, calcium, potassium, phosphates, sulphates,
bicarbonates, glucose, amino acids, uric acid, ascorbic acid etc.
Lecture notes by Dr. Arham Shabbir
34.
0 Passive reabsorption:
0Water, chloride, and urea are reabsorbed passively.
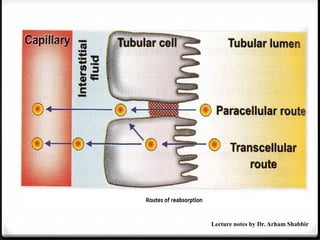
0 Routes of reabsorption:
0 Reabsorption occurs by two routes
0 1- Trancellular route
0 2- Paracellular route
1- Trancellular route:
It includes the transport of substances from:
A- Tubular lumen into tubular cells through apical surface of the cell
membrane.
B- Tubular cell into intestinal fluid
C- Interstitial fluid into capillary
Lecture notes by Dr. Arham Shabbir
0 Paracellular route:
Thesubstances move through intercellular space
It includes transport of substance from:
A- Tubular lumen into intestinal fluid through the tight
junctions between the cells
B- From interstitial fluid into the capillary
Sites of reabsorption:
1. Proximal convoluted tubules
2. Loop of Henle
3. Distal convoluted tubule
Lecture notes by Dr. Arham Shabbir
37.
0 Regulation oftubular reabsorption:
0 Three factors are involved
0 1- Glomerulotubular balance
0 2- Hormonal factors
0 3- Nervous factors
0 Glomerulotubular balance:
0 It is the balance between the filtration and reabsorption of
solutes and water in kidney.
0 When GFR increases, the tubular load of solutes and water in
the proximal convoluted tubules is increased. It is followed
by increase in the reabsorption of solutes and water.
Lecture notes by Dr. Arham Shabbir
38.
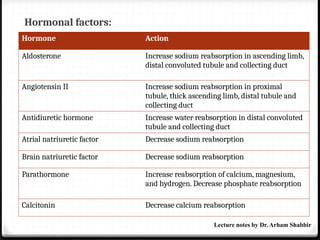
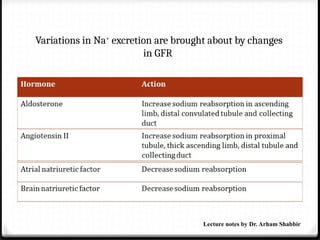
Hormonal factors:
Hormone Action
AldosteroneIncrease sodium reabsorption in ascending limb,
distal convoluted tubule and collecting duct
Angiotensin II Increase sodium reabsorption in proximal
tubule, thick ascending limb, distal tubule and
collecting duct
Antidiuretic hormone Increase water reabsorption in distal convoluted
tubule and collecting duct
Atrial natriuretic factor Decrease sodium reabsorption
Brain natriuretic factor Decrease sodium reabsorption
Parathormone Increase reabsorption of calcium, magnesium,
and hydrogen. Decrease phosphate reabsorption
Calcitonin Decrease calcium reabsorption
Lecture notes by Dr. Arham Shabbir
39.
0 Nervous factors:
0Activation of sympathetic nervous system increases the
tubular re absorption (particularly of sodium) from renal
tubules.
0 Sympathetic system also increases renin release which in
turn releases angiotensin-II
0 Angiotensin –II causes increase in sodium reabsorption
Lecture notes by Dr. Arham Shabbir
40.
Reabsorption of sodium
099% sodium of glomerular filtrate is reabsorbed.
0 Two third of sodium is reabosrbed in proximal convoluted
tubule and remaining one third in other segments except
descending limb.
0 3 steps are involved
0 1- Transport from lumen of tubules into the tubular
epithelial cells
0 In exchange for hydrogen ion by antiport (sodium counterport
protein) in proximal convoluted tubule
0 Along with other substances like glucose and aminoacids by
symport (sodium co-transport protein) in other segments
Lecture notes by Dr. Arham Shabbir
41.
0 2- Transportfrom tubular cells into the interstitial fluid
0 Sodium is pumped outside the cells by sodium potassium
pump.
0 This pump moves three sodium ions from the cells into the
interstitium and two potassium ions from interstitium into
the cells.
0 Tubular epithelial cells are connected with their neighboring
cells by tight junction, a small space is left between the
adjoining cells along their lateral borders. This space is called
lateral intracellular space. The interstitium extends into this
space.
0 Most of the sodium ions are pumped into the lateral
intracellular space
Lecture notes by Dr. Arham Shabbir
42.
0 Transport ofsodium out of the tubular cells decreases the
sodium concentration within the cells. This develops an
electrochemical gradient between the lumen and tubular cells
resulting in diffusion of sodium into the cells
0 3- Transport from interstitial fluid to the blood
0 From the interstitial fluid, sodium ions enter the peritubular
capillaries by concentration gradient.
0 In distal convoluted tubule, the sodium reabsorption is
stimulated by the hormone aldosterone secreted by adrenal
cortex
Lecture notes by Dr. Arham Shabbir
43.
Tubular secretion
0 Itis the process by which the substances are transported from blood
into renal tubules.
0 In addition to reabsorption, some substances are also secreted into
the lumen from the peritubular capillaries through the tubular
epithelial cells.
0 Examples:
0 Penicillin
0 Amino derivatives
0 Para-aminohippuric acid
Lecture notes by Dr. Arham Shabbir
44.
0 Substances secretedin different segments of renal
tubules:
0 Potassium is secreted actively by sodium-potassium pump in
proximal and distal convoluted tubules and collecting duct
0 Ammonia is secreted in the proximal convoluted tubules
0 Hydrogen ions are secreted in proximal and distal convoluted
tubules. Maximum hydrogen ion secretoin occurs in proximal
tubule
0 Urea is secreted in loop of Henle
Lecture notes by Dr. Arham Shabbir
45.
Concentration and dilutionof Urine /
Renal process for water
0 When the glomerular filtrate passes through the renal tubule, its osmolarity
(concentration of solute expressed as number of solute particles per liter) is
altered in different segments.
0 1- Bowman Capsule:
0 Glomerular filtrate collected at the Bowman capsule contains all the
substances of plasma except proteins. Osmolarity of filtrate in Bowman
capsule is 300 mOsm/L
0 2- Proximal convoluted tubules:
0 Obligatory reabsorption is the type of water reabsorption in proximal
convoluted tubule, which is secondary to sodium reabsorption.
0 When sodium is reabsorbed from the tubule, the osmotic pressure decreases. It
causes osmosis of water from renal tubule.
0 When the filtrate flows through proximal convoluted tubules, there is active
reabsorption of sodium and chloride followed by obligatory reabsorption of
water. So the osmolarity remains the same as in Bowman capsule.
Lecture notes by Dr. Arham Shabbir
47.
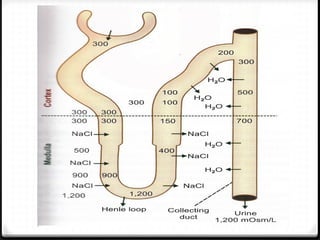
0 3- Thickdescending segment:
0 When the fluid passes into the thick descending segment, water is
reabsorbed from lumen into outer medullary interstitium by means
of osmosis.
0 The fluid becomes slightly hypertonic to plasma i.e. 450-600 mOsm/L
0 4- Thin descending segment:
0 This segment is highly permeable to water so more water is
reabsorbed.
0 So osmolarity of the tubular fluid becomes equal to that of the
sorrounding medullary interstitium
0 Thus in this segment fluid is hypertonic to plasma
Lecture notes by Dr. Arham Shabbir
48.
5-Thin ascending segmentof Henle Loop:
When the thin ascending segment of the loop ascends upwards
through the medullary region, osmolarity gradually decreases.
Due to concentration gradient, sodium chloride diffuses out of
tubular fluid and osmolarity decreases to 400 mOsm/L. the fluid
in this segment is slightly hypertonic to plasma
6-Thick ascending segment of Henle Loop:
This segment is impermeable to water but sodium and chloride
are actively absorbed from this site.
Reabsorption of sodium decreases the osmolarity of tubular
fluid to a greater extent.
The osmolarity is between 150-200 mOsm/L. The fluid becomes
hypotonic to plasma.
Lecture notes by Dr. Arham Shabbir
49.
0 7- Distalconvoluted tubule and collecting duct:
0 Facultative water reabsorption is a type of water reabsorption that occurs by
the activity of anti diuretic hormone.
0 Normally the distal convoluted tubule and collecting duct are not permeable
to water. But in the presence of ADH, distal convoluted tubule and collecting
duct becomes permeable to water resulting in water reabsorption and final
concentration of urine.
0 MOA of ADH-aquaporins
0 ADH increases water reabsorption by stimulating the water channels called
aquaporins
0 Aquaporins are the membrane proteins, which functions as water channels.
0 ADH acts on aquaporins which increases cyclic AMP production, which in
turn increase the water re absorption.
0 Reabsorption of large quantity of water increases the osmolarity to 1,200
mOSm/L. The urine becomes hypertonic to plasma
Lecture notes by Dr. Arham Shabbir
50.
Lecture notes byDr. Arham Shabbir
Acidification of urine and buffering of
H+
0 1. Biocarbonate mechanism:
0 About 4,320 mEq of HCO3
-
is filtered by the glomeruli every
day and called as filtered load of HCO3
-.
0 Excretion of much HCO3
-
effect the acid-base balance of the
body fluids. So HCO3
-
must be taken back by reabsorption
0 Reabsorption of HCO3
-
by secretion of H+
in the renal tubules.
0 About 4,380 mEq of H+
appear every day in renal tubule but
not all is excreted.
0 Out of this, 4,280 to 4, 330 mEq is utilized for the reabsorption
of HCO3
-
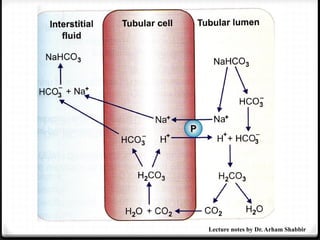
0 H+
secreted intothe renal tubule combines with filtered
HCO3
-
forming H2CO3 (Also called bicarbonate buffer system).
0 Carbonic acid dissociated into carbon dioxide and water by
carbonic anhydrase
0 Carbon dioxide enters the tubular cell and combines with
water to for carbonic acid
0 It immediately dissociates into HCO3
-
and H+
.
0 HCO3
-
enters the interstitium and combines with sodium ion
to form sodium bicarbonate
0 Sodium ion is reabsorbed from the lumen into tubular cell
under the influence of aldosterone
0 H+
is secreted in the lumen from the cell in exchange for
sodium ion.
Lecture notes by Dr. Arham Shabbir
53.
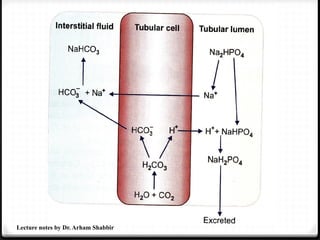
0 2- Phosphatemechanism:
0 In tubular cell carbon dioxide combines with water to form
carbonic acid.
0 It immediately dissociates into HCO3
-
and H+
.
0 HCO3
-
enters the interstitium and combines with sodium ion
to form sodium bicarbonate.
0 Sodium ion is reabsorbed from the lumen into tubular cell
under the influence of aldosterone
0 H+
is secreted in the lumen from the cell in exchange for
sodium ion.
0 H+
in the lumen reacts with phosphate buffer system and
combines with sodium hydrogen phosphate (also called
phosphate buffer system).
Lecture notes by Dr. Arham Shabbir
0 Sodium dihydrogenphosphate is excreted in the urine.
0 The H+
which is added to the urine in the form of
sodium dihydrogen makes the urine acidic.
0 It happens mainly in distal tubule and collecting duct
because large quantities of sodium hydrogen phosphate
in these segments.
Lecture notes by Dr. Arham Shabbir
56.
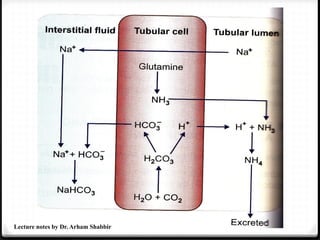
0 3- Ammoniamechanism:
0 In tubular cells ammonia is formed when the amino acid glutamine
is converted to glutamic acid in the presence of enzyme glutaminase.
0 Ammonia is also formed by the deamination of some of the amino
aids such as glycine and alanine.
0 Ammonia (NH3) formed in tubular cells secreted into lumen in
exchange for sodium ion.
0 In lumen, it combines with H+ to form ammonium (NH4) (Also
called as ammonia buffer system).
0 The tubular cell is not permeable to ammonium, hence excreted in
the urine.
0 The H+
ion is added to the urine in the form of ammonium
compounds resulting in acidification of the urine.
0 For each ammonium excreted one HCO3
-
is added to the interstitial
fluid
Lecture notes by Dr. Arham Shabbir
0 This processtakes place mostly in proximal convoluted
tubules because glutamine is converted to ammonia in the
cells of this segment.
Lecture notes by Dr. Arham Shabbir
59.
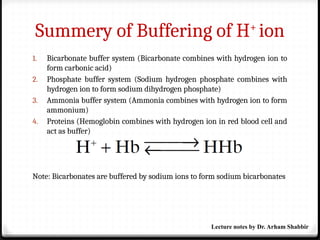
Summery of Bufferingof H+
ion
1. Bicarbonate buffer system (Bicarbonate combines with hydrogen ion to
form carbonic acid)
2. Phosphate buffer system (Sodium hydrogen phosphate combines with
hydrogen ion to form sodium dihydrogen phosphate)
3. Ammonia buffer system (Ammonia combines with hydrogen ion to form
ammonium)
4. Proteins (Hemoglobin combines with hydrogen ion in red blood cell and
act as buffer)
Note: Bicarbonates are buffered by sodium ions to form sodium bicarbonates
Lecture notes by Dr. Arham Shabbir
60.
Renal sodium regulation
0Normally, 96% to well over 99% of the filtered Na+
is
reabsorbed.
0 Na+
is the most abundant cation in ECF and because Na+
salts account for over 90% of the osmotically active solute in
the plasma and interstitial fluid.
0 Therefore, it is not surprising that multiple regulatory
mechanisms have evolved to control the excretion of this ion.
Lecture notes by Dr. Arham Shabbir
61.
Renal sodium regulation
0Through the operation of these regulatory mechanisms, the amount
of Na+
excreted is adjusted to equal the amount ingested over a wide
range of dietary intakes, and the individual stays in Na+
balance.
0 Thus, urinary Na+
output ranges from less than 1 mEq/d on a low-
salt diet to 400 mEq/d or more when the dietary Na+
intake is high.
0 In addition, there is a natriuresis when saline is infused
intravenously and a decrease in Na+
excretion when ECF volume is
reduced.
Lecture notes by Dr. Arham Shabbir
Renal sodium regulation
0Reduction of dietary intake of salt increases aldosterone secretion,
producing marked but slowly developing decreases in Na+
excretion.
0 In the collecting ducts, Na+
is generally reabsorbed and K+
is
secreted. There is no rigid one-for-one exchange, and much of the
movement of K+
is passive. However, there is electrical coupling in
the sense that intracellular migration of Na+
from the lumen tends
to lower the potential difference across the tubular cell, and this
favors movement of K+
into the tubular lumen.
0 Because Na+
is also reabsorbed in association with H+
secretion,
there is competition for the Na+
in the tubular fluid. K+
excretion is
decreased when the amount of Na+
reaching the distal tubule is
small, and it is also decreased when H+
secretion is increased.
Lecture notes by Dr. Arham Shabbir
64.
Regulation of potassium
0Much of the filtered K+
is removed from the tubular fluid
by active reabsorption in the proximal tubules, and K+
is
then secreted into the fluid by the distal tubular cells.
0 In the absence of complicating factors, the amount
secreted is approximately equal to the K+
intake, and K+
balance is maintained.
Lecture notes by Dr. Arham Shabbir
65.
Regulation of potassium
0In the collecting ducts, Na+
is generally reabsorbed and
K+
is secreted. There is no rigid one-for-one exchange,
and much of the movement of K+
is passive. However,
there is electrical coupling in the sense that intracellular
migration of Na+
from the lumen tends to lower the
potential difference across the tubular cell, and this
favors movement of K+
into the tubular lumen.
0 Because Na+
is also reabsorbed in association with H+
secretion, there is competition for the Na+
in the tubular
fluid. K+
excretion is decreased when the amount of Na+
reaching the distal tubule is small, and it is also
decreased when H+
secretion is increased.
Lecture notes by Dr. Arham Shabbir
66.
Renal water regulation
ADH/vasopressin
0Increases water reabsorption in distill convoluted tubule and
collecting duct.
Water diuresis
0 It is produced by drinking large amounts of hypotonic fluid begins
about 15 min after ingestion of a water load and reaches its maximum.
0 The act of drinking produces a small decrease in vasopressin secretion
before the water is absorbed.
Lecture notes by Dr. Arham Shabbir
Diuretics
1. Water
2. Carbonicanhydrase inhibitors
Acetazolamide
3. Thiazide diuretics
Hydrochlorothiazide
4. Loop diuretics
Furosemide
5. Potassium sparing diuretics
Spironolactone
6. Osmotic diuretics
Mannitol
Lecture notes by Dr. Arham Shabbir
69.
Kidney diseases (Definitions)
Metabolicacidosis:
0 It occurs when kidney fails to excrete metabolic acids
Metabolic alkalosis:
0 When kidney excrete large quantity of hydrogen
Nephrogenic diabetes insipidus:
0 ADH secretion is normal but renal tubules fail to give
response to ADH resulting in polyuria
Lecture notes by Dr. Arham Shabbir
70.
Kidney diseases (Definitions)
0Severe kidney diseases can be divided into two main
categories:
(1) acute renal failure, in which the kidneys abruptly stop
working entirely or almost entirely but may eventually
recover nearly normal function.
(2) chronic renal failure, in which there is progressive loss
of function of more and more nephrons that gradually
decreases overall kidney function.
Lecture notes by Dr. Arham Shabbir














![Renal_Phsyiology_2021_INTRODUCTION[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/renalphsyiology2021introduction1-240913164449-bc60bf41-thumbnail.jpg?width=640&height=640&fit=bounds)
































