Rabies is aserious and deadly disease
with a nearly 100% fatality rate if left
untreated.This presentation will delve
into the epidemiology of rabies, focusing
on its global burden, transmission
patterns, and risk factors.
3.
• Rabies lyssavirus,is a neurotropic virus that causes rabies in
animals, including humans.
• Rabies transmission can occur through the saliva of animals and
less commonly through contact with human saliva.
• Rabies lyssavirus, like many rhabdoviruses, has an extremely wide
host range. In the wild it has been found infecting many
mammalian species, while in the laboratory it has been found that
birds can be infected, as well as cell cultures from mammals, birds,
reptiles and insects.
5.
Global Burden
•Rabies isendemic in over 150 countries and
territories.
•Highest burden in Africa and Asia, with an
estimated 59,000 deaths annually.
•Canine rabies remains a significant problem in
many developing countries.
•Wildlife rabies is increasingly prevalent in
developed countries.
7.
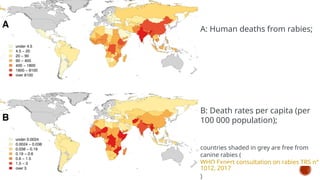
A: Human deathsfrom rabies;
B: Death rates per capita (per
100 000 population);
countries shaded in grey are free from
canine rabies (
WHO Expert consultation on rabies TRS n°
1012, 2017
)
• India isendemic for rabies, and accounts for 36% of the world’s
rabies deaths.
• True burden of rabies in India is not fully known; although as per
available information, it causes 18 000-20 000 deaths every year.
• About 30-60% of reported rabies cases and deaths in India occur
in children under the age of 15 years as bites that occur in
children often go unrecognized and unreported.
• India has the highest rate of human rabies in the world, primarily
because of stray dogs, whose number has greatly increased since
a 2001 law forbade the killing of dogs
RABIES IN INDIA
11.
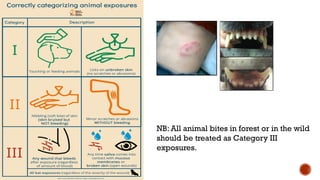
RESERVOIR HOSTS OFRABIES
Different animal species serve as reservoirs for rabies in various regions.
Dogs are the primary reservoir in many developing countries.
Wildlife, such as raccoons, skunks, foxes, and bats, are the main reservoirs in
developed countries.
12.
TRANSMISSION OF RABIES
•Rabies is primarily transmitted through the saliva of
infected animals.
• Bites are the most common route of transmission.
• Non-bite exposures, such as scratches or contact with
mucous membranes, are less frequent but possible.
• Human-to-human transmission is extremely rare.
13.
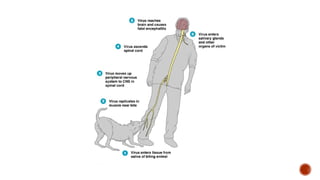
INFECTION
From thewound of entry, Rabies lyssavirus travels quickly along the
neural pathways of the peripheral nervous system.The retrograde
axonal transport of Rabies lyssavirus to the central nervous system
(CNS) is the key step of pathogenesis during natural infection.The
exact molecular mechanism of this transport is unknown.
From the CNS, the virus further spreads to other organs.The salivary
glands located in the tissues of the mouth and cheeks receive high
concentrations of the virus, thus allowing it to be further transmitted
due to projectile salivation.
15.
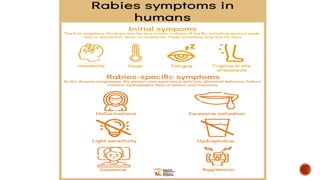
SIGNS AND SYMPTOMS
Thefirst symptoms of rabies may be very similar to those of the flu,
including general weakness or discomfort, fever, or headache. These
symptoms may last for days. There may be also discomfort or a
prickling or itching sensation at the site of bite.
As rabies progresses and causes inflammation of the brain and
meninges, symptoms can include slight or partial paralysis, anxiety,
insomnia, confusion, agitation, abnormal behavior, paranoia, terror,
and hallucinations. The person may also have fear of water.
The symptoms eventually progress to delirium, and coma. Death
usually occurs two to ten days after first symptoms. Survival is
almost unknown once symptoms have presented, even with
intensive care.
17.
DIAGNOSIS
The reference methodfor diagnosing rabies is the
fluorescent antibody test (FAT), an
immunohistochemistry procedure, which is recommended
by the World Health Organization (WHO).
The diagnosis can be reliably made from brain samples
taken after death.The diagnosis can also be made from
saliva, urine, and cerebrospinal fluid samples, but this is not
as sensitive or reliable as brain samples.
Cerebral inclusion bodies called Negri bodies are 100%
diagnostic for rabies infection but are found in only about
80% of cases.
18.
RISK FACTORS FORRABIES
• Living in an area with high rabies endemicity.
• Working with animals, particularly those at risk of rabies
exposure (e.g., veterinarians, wildlife rehabilitators).
• Traveling to rabies-endemic countries.
• Engaging in activities that increase the risk of animal
encounters (e.g., hiking, camping).
• Lack of rabies vaccination in pets or oneself (in high-risk
areas).
19.
PREVENTION
Rabies ispreventable. Keeping pets safe and staying away from wild
animals will help prevent from being exposed to rabies. If exposed, One
can get a vaccine to prevent rabies before symptoms start.
• Make sure pets’ vaccinations are up-to-date. This includes dogs, cats and
ferrets.
• Don’t let pets roam free without supervision.
• Leave wildlife alone. Don’t touch injured animals or try to capture animals
yourself.
• If bitten or scratched by a wild animal or have been exposed to rabies in
some other way, contact a healthcare provider as soon as possible.
• If you’re at high risk for being exposed to rabies, it’s recommended that
you get vaccinated on a regular basis (pre-exposure prophylaxis/PREP).
20.
ANIMAL BITE MANAGEMENTAND POST
EXPOSURE PROPHYLAXIS OF RABIES
Decision to treat:
Rabies is endemic in India; so management of animal bites is essential
Suspect all animal bites, even scratches
Treat as per merit of the bite
Post Exposure Prophylaxis (PEP) should be started as soon as possible
after the bite.
Start treatment and observe the animal for 10 days (applicable only for dog
and cat)
If the animal (dog and cat) remains healthy throughout the observation then
modify the Post-Exposure Prophylaxis (PEP) to Pre-Exposure Prophylaxis
(PrEP).
22.
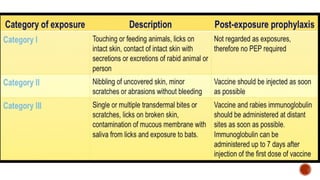
NB: All animalbites in forest or in the wild
should be treated as Category III
exposures.
23.
Principles of treatment:
A.Woundmanagement
B. Passive immunization (inj. of immunoglobulin/anti-sera)
C. Active immunization i.e. inj. of anti-rabies vaccine (ARV)
24.
A. Wound management:
Wash the wound immediately (as early as possible) under running tap water for at least
10 minutes.
Use soap or detergent to wash the wound (if soap is not available then use water only to
wash the wound).
After thorough washing and drying the wound apply disinfectant – e.g. povidone iodine,
spirit etc.
Don’t apply irritants viz. chilli, soil, oils, turmeric, lime, salt, plant juice etc.
Don’t touch the wound with bare hands.
Wound washing must be performed even if the patient reports late.
Postpone suturing if possible; if suturing is at all necessary, it should be performed after
cleaning and infiltrating RIG at the depth of wound and only minimum number of loose
suture should be applied.
Don’t cauterize.
Administer systemic antimicrobial and tetanus toxoid if necessary (follow usual norm of
wound management in this regard)
25.
B. Passive immunization(immunoglobulin/anti-sera):
Human Rabies Immunoglobulin (HRIG): 20 IU/kg body wt, maximum 1500 IU
Equine Rabies Immunoglobulin (ERIG) : 40 IU/kg body wt, maximum 3000 IU
Local infiltration of rabies immunoglobulin: RIG should be infiltrated in the depth and
around each of the wounds to inactivate the locally present rabies viruses.
Infiltrate as much as possible in the depth and around the wounds; remaining quantity,
if any, is to be administered intramuscularly at a site away from the site where vaccine is
administered.
If RIG is insufficient (by volume) for infiltration into all the wounds, dilute it with sterile
normal saline (up to twice or thrice the volume).
Infiltrate into all Category III wounds.
26.
C.Vaccination:
Route ofinoculation: Intramuscular or Intradermal.
Site of inoculation: Deltoid muscle or anterolateral part of thigh. Not
recommended in gluteal region, since there is chance of low absorption due to
presence of fatty tissue.
Post exposure Vaccine schedule:
The vaccination schedule may be either of the following. However, in healthcare
institutions, the latter (Intradermal Regimen) is more cost effective and is
mandatory in State Government set-ups except in documented exceptional cases.
27.
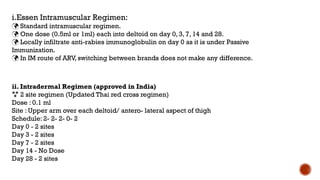
i.Essen Intramuscular Regimen:
Standard intramuscular regimen.
One dose (0.5ml or 1ml) each into deltoid on day 0, 3, 7, 14 and 28.
Locally infiltrate anti-rabies immunoglobulin on day 0 as it is under Passive
Immunization.
In IM route of ARV, switching between brands does not make any difference.
ii. Intradermal Regimen (approved in India)
2 site regimen (Updated Thai red cross regimen)
Dose : 0.1 ml
Site : Upper arm over each deltoid/ antero- lateral aspect of thigh
Schedule: 2- 2- 2- 0- 2
Day 0 - 2 sites
Day 3 - 2 sites
Day 7 - 2 sites
Day 14 - No Dose
Day 28 - 2 sites
30.
• India’s NAPREby 2030 was released during the coronavirus disease
2019 (COVID-19) period of 2020, and it came into operation in 2021.
• The veterinary public health components include estimating the
population of dogs, mapping risk zones for rabies, program for mass
dog vaccination, effective management and disposal of solid waste,
operational research, and promotion of responsible dog ownership.
• The program components for human public health components
include postexposure prophylaxis (PEP), trained human resources,
enhancing surveillance of dog bites and clinical rabies in humans,
appropriate communication strategies, and public–private
partnerships.