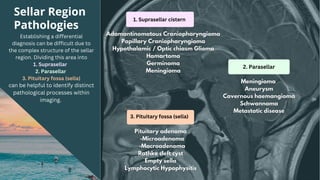
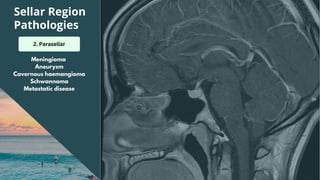
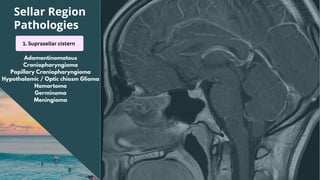
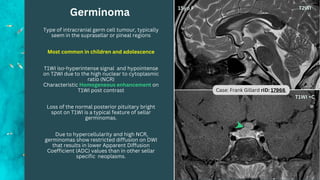
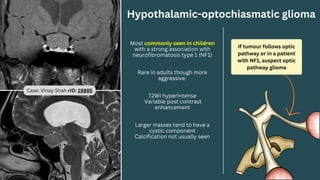
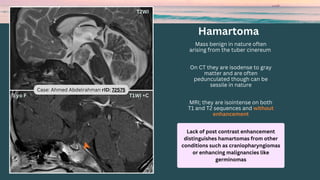
1. The document provides an overview of common pathologies that can occur in the sellar region, which is divided into the suprasellar, parasellar, and pituitary fossa.
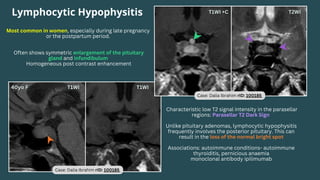
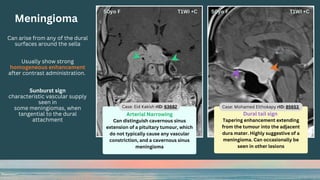
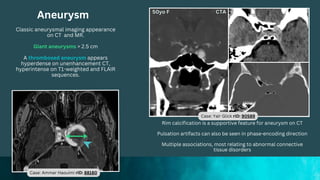
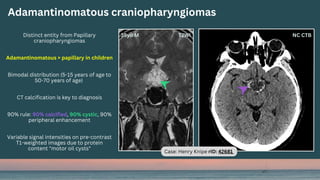
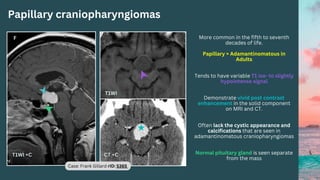
2. Key pathologies discussed include pituitary adenomas, craniopharyngiomas, meningiomas, aneurysms, and lymphocytic hypophysitis. Imaging features on MRI and CT that are useful for diagnosis are presented.
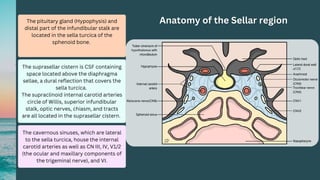
3. The importance of understanding the anatomy of the sellar region and correlating imaging findings with clinical information is emphasized for accurate diagnosis of sellar pathologies.