Case Presentation OnMgt Of chronic Ectopic Px
YIRGALEM HOSPITAL MEDICAL COLLEGE
Presenter: Dr. Awgichew (OBGYN-RI)
Consultant: Dr. Anbese (Ass’t Pro.of obstetrics & gynecology ,RH subspecialist)
Dr. Diba (OBGYN- RII)
June- 19,2023
Case - Identification
Name –A.T
Age- 22 yrs
Sex - Female
Adress – Sidama –dale woreda
Admitted on -29/09/15 E.C
Discharged on – 03/10/15 E.C
5.
Case…History
C/c- Vaginal bleedingof 3wks duration
o This 22 yr old primigravida lady ,she didn’t remember her
date, amenoric for last 3mths.
o Presented with spotting vaginal bleeding of 3wks
duration ,associated with intermittent lower abdominal
pain which get worse in the last 3 days prior to
presentation.
6.
Case…History
o she ismarried since last 7mths and live with him ,but she
had another boy friend for 3yrs prior to current husband.
o she had been using post pills repeatedly while she was
with her prior boy friend and once after recent marriage.
o Otherwise no hx of
o DM/HTN, Rx for STI ,surgery
o smoking, ABM or fainting
7.
Case…PE
Physical examination
o GA---healthy looking
o V/s –BP= 130/70 PR= 78 RR= 20 T= ATT
o HEENT – pink conjectiva ,NIS
o Abdomen – flat move with respiration
- No organomegaly or mass
- No sign of fluid collection
o GUS - no active Vx bleeding
- Cx is closed with motion tenderness
- blood stained examining finger
o CNS - COTPP
Case…Investigations
Pelvic ultrasound
o emptyuterine cavity
o No free fluid in the paracolic gutter and morison
pouch
o There is 7*7 cm complex Lt adnexal hyperechoic mass
with minimal cul-de-sac collection
Index - ? Chronic ectopic pregnancy
11.
Case…Ass’t and plan
Ass’t– Primigravida
_ ? Chronic ectopic pregnancy
Plan
o admited to Gyn-side
o Prepare 2-x-matched blood
o Prepare for next day laparaomy
12.
Case…Done (Mgt)
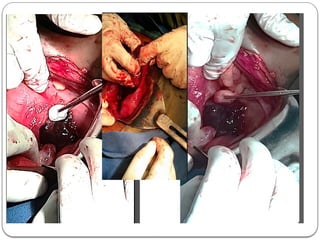
Laparotomy –Lt Salphingo-ophorectomy
o SA ,then to GA
o Pfannensiel Incision
o IOF
Health looking non-gravid Ux
Healthy looking Rt tube and ovary
Lt ovary and tubes distorted and form a mass and
adhesion to sigmoid colon
200ml heamoperitonium
14.
Case…Done (Mgt)
Laparotomy –Lt Salphingo-ophorectomy
oDone
heamo-peritonium sucked out
Adhesion between mass and bowel released until it
resist and strongly adhere mass capsule left
Lt Salphingo-opheroctomy
Lavaged with 1000ml warn saline
After haemostasis secured and checked ,and correct
count reported abdominal layers closed layer by
layer.
15.
Case…Done (Mgt)
Immediate postop- after Lt salphingo-opheroctomy was done
for the indication of Lt-side chronic EP.
o Post op order
o 3 bag over 24hrs
o ceftriaxone 1gm iv bid
o Metronidazole 500mg iv tid for 48hrs
o Diclofenac 75mg im bid
o keep catheter for 24hrs
o NPO for 12 hrs
o post op Hct after 24hrs
o V/s q15’ for 2hrs, q30’ for 2hrs then q4hrs
o send sample for histopathology
o Doxycycline 100mg po bid
o Metronidazole 500mg po bid for 2wks at discharge
16.
Case…Post-op condition
Smooth 1st
post-opdays
o started ambulation
o started SIPs
o Post-op HCT—30% (Hgb-12.9gm/dl)
o Advise on F/P (took Implanon ) and recurrence
o Closely follow V/s
17.
Case…Post-op condition
Smooth 2nd
post-opday (2/10/15 E.C)
o ambulating
o started regular diet
o serial HCT (repeat)
o Base line B-HCG
o Bought po medications (doxy,metro and iron)
o consider discharge tomorrow after collecting Ixs
18.
Case…Post-op condition
Smooth 3rd
post-opday (3/10/15 E.C)
o ambulating
o started regular diet
o HCT (repeated-Hgb = 8.9gm/dl , Hct =27.9%)
o B-HCG (216.4 IU/ml)
o Bought po medications (doxy,metro and iron)
o discharged with appointment
19.
Comments
strength
- high indexof suspicion and diagnosis
- senior consulted
- blood prepared (2 unit)
- took contraceptive (documented)
Pitfall
- baseline- B-HCG was not done
- Anaemia not included post-op
Introduction
Ectopic pregnancy(EP)
2% of all pregnancies (9% of pregnancy-related deaths)
o African countries 0.5 - 2.3%
o In Ethiopia - 0.82%
leading cause of death in the 1st
tmp (4%)
6–16 % of ER patient with vaginal bleeding and/or
abdominal pain ( index of suspicion needs to be high)
23.
Introduction…con’t
Ectopic pregnancy(EP)
We can have lists of risk factors, but exact aetiology not known
Etio-pathologic theories are generally distinguished between
maternal and embryonic factors (maternal –infection, tubal
surgery ,IUD and p-only pills ,and embryonic factors-
chromosomal and structural anomalies-high incidence of Ep )
24.
Introduction…con’t
Ectopic pregnancy(EP)
Has risk factors ,but up to 50 % of cases without risk factors
one of important risk is prior hx - 8–15% will repeat EP.
one-half -diagnosed at initial presentation
one-half - diagnosed only after further medical surveillance
two hypothetical natural histories of ectopic pregnancy
o acute presentation (type I)
o chronic presentation (type II)
25.
Chronic ectopic pregnancy(CEP)
CEP
Asymptomatic / protracted clinical presentation
HCG level -low or absent and resistance for MTX.
Rupture late/ not at all
variable and non-specific clinical signs and symptoms and there
remains no universal agreement about the definition of CEP.
it is retrospective dx considering c/f & intra operative finding
develops when the trophoblastic tissue gradually invades
implantation site leading to repeated rupture and continued minor
bleeding over time develop haematocele and appear a pelvic mass
Chronic ectopic pregnancy(CEP)
CEP
exact incidence is difficult due to varied criteria for definition.
o 6- 20% of EP
final dx often made with histology findings of haemorrhage and
blood clots, disintegration of the tubal wall, multiple minor
ruptures, areas of dense fibrosis and necrosis embedded within
degenerated and/or a vital chorionic villi.
28.
Chronic ectopic pregnancy(CEP)
CEP
its atypical symptom (complicate patients & difficult to
diagnose)
incidence - difficult to assess due to rarity and varying
definitions used
a more unusual situation, resulting from minor ruptures that
develop into a haematocele (typically surrounded by adhesions
and induces an inflammatory response)
30.
Chronic ectopic pregnancy(CEP)
A study to compare acute vs chronic presentation of EP to look for
differences in the patient characteristics and short-term sequelae.
University of Pennsylvania, Philadelphia, Pennsylvania
retrospective cohort study
Department OBGYN has developed its own electronic data
management systems since 1989
452 patients diagnosed with EP in the years 1993–1998.
total of 37 parameters were analysed.
31.
Chronic ectopic pregnancy(CEP)
analysed based on 37 parameters
o age, race, gravity, parity
o Hx of EP, number of prior miscarriages, number of prior
elective terminations, number of prior cesarean sections
o Prior pelvic surgery, tubal ligation, PID
o IUD placement
o outpatient treatment for gonorrhoea and Chlamydia
o fertility medications
o blood type and Rh status.
32.
Chronic ectopic pregnancy(CEP)
Result (452)
249 (55%) dxsed at initial visit and 203 (45%) required >1vist
Hx of EP, prior miscarriages, prior pelvic surgery, tubal
ligation, PID and IUD placement has similar effect.
About 30% had >=1 STDs in both group
primary presentation for delayed one was
• bleeding than pain
• less likely to be hypotensive
• has non-diagnostic Ultrasound
33.
Chronic ectopic pregnancy(CEP)
Result (452)
primary presentation for delayed one was
• More likely to be managed medically
• less likely to be ruptured (usually on ampulla)
• Lower EBL and shorter hospital stay
35.
Chronic ectopic pregnancy(CEP)
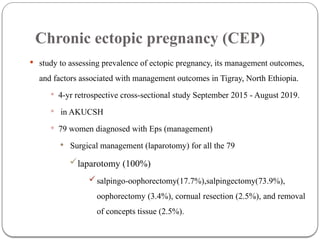
study to assessing prevalence of ectopic pregnancy, its management outcomes,
and factors associated with management outcomes in Tigray, North Ethiopia.
4-yr retrospective cross-sectional study September 2015 - August 2019.
in AKUCSH
79 women diagnosed with Eps (management)
Surgical management (laparotomy) for all the 79
laparotomy (100%)
salpingo-oophorectomy(17.7%),salpingectomy(73.9%),
oophorectomy (3.4%), cornual resection (2.5%), and removal
of concepts tissue (2.5%).
36.
OBGY Department,Royal Derbyhospital,Derby,UK,2022
1st
impression wasTOA latter CEP for whom Rt salpingectomy was done
37.
27yrs old,G-2 ,P-1 (with c/s) ,came for evaluation with a complain of
rt lower abdominal pain and intermittent vx-bleeding of 12 days
stable vital sign
6*6cm mass at rt iliac fossa with rebound tenderness
on speculum – 8*6cm tender mass in posterior fornix
Ultrasound 8.7*8cm mixed lt ovarian mass with suspicious of lt
ovarian teratoma (empty ux)
38.
Pelvic CT—10*8cmrt tubo-ovarian mass (sugestive of CEP)
Exploratory laparotomy done
small bowel adhesion to cystic mass in rt FT along with rt
ovary,that densely adher to posterior surface of Ux
entire complet with tube and ovary removed with Rt
salphingoophorectomy
Histo-pathologic result showed a dilated FT containing blood clot and
trophoblast along with fibrin rich infarcted and viable chorionic villi,
confirming the diagnosis of ectopic pregnancy.
Management of CEP
main stay of management is surgery
Salpingectomy
salphingostomy
Diagnosis confirmed by
surgery and histopathology
medical
MTX
41.
Persistent ectopic pregnancy
following surgery
Rare following Salpingectomy
5-15% (5-20%) of salphingostomy
laparotomy less than laparoscopy
Factor increase rate
small px (<2cm)
early therapy (before 42menstrual days)
serum hcg >3000miu/ml
implantation to salphingostomy site
Take-home message
Eventhough it is rare, bilateral ectopic pregnancy should be
considered in all patients with ectopic pregnancy, and
contralateral adnexa has to be examined during sonographic
evaluation, laparoscopy or laparotomy
The diagnosis of CEP could be quite challenging as a result
of the protracted symptoms, often negative/low serum B-
HCG and ultrasound features mimicking a pelvic mass.A high
index of suspicion is needed, and an MRI scan and diagnostic
laparoscopy often aid in diagnosis and management
44.
Reference
D. Abebe,D. Tukue, A. Aregay, and L. Gebremariam,
“Magnitude and Associated Factors with Ectopic Pregnancy
Treated in Adigrat Hospital, Tigray Region, Northern
Ethiopia,” International Journal of Pharmaceutical Sciences
and Research, vol. 7, no. 1, pp. 30–39, 2017.
Elsa Tesfa Berhe , Kalayu Kiros ,Merhawit Gebremeskel
Hagos and eta’l, ‘‘Ectopic Pregnancy Management
Outcomes, and Associated Factor in Tigray, Ethiopia,
Hindawi Journal of Pregnancy, ID 4443117, 8 pagesVolume
2021.