CASE SCENARIO
• Name:R.A.W
• Age : 35yrs
• Para: 2 + 1 Gravida 4
• LNMP: 18/05/23
• GBD: 3/52
• DOA : 08/06/23
• C/c: LAP for 1/7
PV bleeding for 1/7
4.
HPI
Pt is presentingwith severe LAP radiating to the back increasing in frequency and intensity
worse on the left side.
Reports to be having minimal pv bleeding
O/E
Pt is sick looking
P++, no J, OT, Ly, Fc
Bp 100/60, Pulse 120mg, Temp 37.2, SPO2 98
5.
P/A
• Not distended
•No scars
• Marked tenderness worse on the left iliac fossa
Dx:Acute abdomen/ ?? Raptured Ectopic Pregnancy
6.
RESULTS
• PDT: POSITIVE
•CBC:WBC 12.9, Platelets 150, Hb 12.4mg/dl
• Abdominopelvic U/S
Ascites, No sonographic signs of pregnancy seen.
Solitary intramural fibroid
Left ovarian hemorrhagic cyst
7.
PLAN
• GXM
• NS1L IV stat then 2L slow infusion
• Ceftriaxone 2g IV stat
• Emergency Ex-LAP
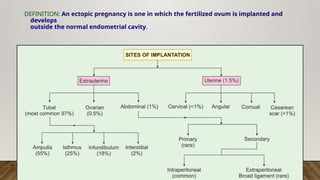
DEFINITION: An ectopicpregnancy is one in which the fertilized ovum is implanted and
develops
outside the normal endometrial cavity.
10.
SITES OF ECTOPICPREGNANCY
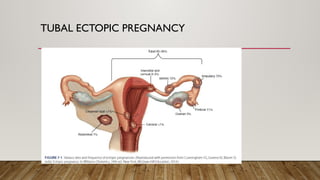
1. Tubal ectopic Pregnancy
2. Ovarian Ectopic Pregnancy
3. Cervical
4. C/S site
5. Abdominal
11.
TYPES OF ECTOPICPREGNANCIES
Acute ectopic pregnancy [30%]
• Acute ectopic pregnancies are more common, produce a high serum β-hCG level, and grow rapidly,
leading to a timely diagnosis.
• These carry a greater risk of rupture.
• Mostly presents as raptured ectopic pregnancy with massive hemoperitoneum
Chronic Ectopic Pregnancy
• With chronic ectopic pregnancy, abnormal trophoblasts die early, and thus serum β-hCG levels are
negative or are low and static.
• Chronic ectopic pregnancies typically rupture late, at all, but commonly form a persistent complex
pelvic mass.
• This sonographic finding, rather than patient symptoms, often is the reason that prompts
diagnostic surgery
RISK FACTORS
• Historyof PID
• History of tubal ligation
• Contraception failure eg Progestin only pill {reduce cilia motility}
• Previous ectopic pregnancy
• Tubal reconstructive surgery
• History of infertility
• ART particularly if the tubes are patent but damaged
• IUD use
• Previous induced abortion
• Tubal endometriosis
• Smoking
14.
• The reasonsfor rising incidence of ectopic pregnancies are—
• (i) Rise in the incidence of STIs andsalpingitis.
• (ii) Rise in the incidence of pregnancy following ART procedures.
• (iii) Increased tubal surgery (either sterilization or tuboplasty procedure).
• (iv) Early detection of cases that were otherwise destined to undergo spontaneous
absorption.
15.
CHANGES IN THETUBE
(i) Implantation in the tube occurs more commonly in intercolumnar fashion,i.e. in between two mucosal folds.
(ii) Decidual change at the site of implantation is minimal. The muscles undergo limited hyperplasia and
hypertrophy but more stretching. Blood vessels are engorged.
(iii) The blastocyst burrows through the mucous membrane and lies between the lumen and the
peritoneal covering—so-called intramuscular implantation.
(iv) A pseudocapsule is formed consisting of fibrin, lining epithelium and few muscle fibers.
(v) Blood vessels are eroded by the chorionic villi and blood accumulates in between the blastocyst and the serous
coat.
(vi) The tube on the implantation site is distended and the wall is thinned out.
(vii) Blood may spill from the fimbriated end and may cause hemoperitoneum.
(viii) The stretching of the peritoneum over the site of implantation results in episodic pain. Finally, tubal rupture occurs
when the muscles and the serosa are maximally stretched and undergo necrosis.
(ix) Hemoperitoneum is found in all cases of ruptured tubal ectopic pregnancy.
(x) The trophoblasts of ectopic pregnancy do not usually grow as that of a normal pregnancy. As a result, hCG production
is inadequate compared to a normal pregnancy.
16.
CHANGES IN THEUTERUS:
• Under the influence of estrogen, progesterone from corpus luteum and chorionic
gonadotropin, there is varying amount of enlargement of the uterus with increased
vascularity.
• The decidua develops all the characteristics of intrauterine pregnancy except that it
contains no
• evidence of chorionic villi.
• When progesterone level falls due to fall in the level of hCG, endometrial growth is no longer
maintained.
• Endometrium sloughs out causing uterine bleeding.
• Sometimes entire decidua is expelled as a single piece through the cervix. This is known as
decidual cast that may be confused with a spontaneous abortion.
CLINICAL PRESENTATION… INACUTE ECTOPIC PREGNANCY
• The classic triad of symptomsof disturbed tubal pregnancy are:
• Abdominal pain (100%)
• Amenorrhea (75%)
• Vaginal bleeding (70%).
• Amenorrhea: Short period of 6–8 weeks (usually); there may be delayed period or history of vaginal
spotting. Amenorrhea may be absent even.
• Abdominal pain is the most constant feature. It is acute, agonizing or colicky. Otherwise it may be a
vague soreness. Pain is located at lower abdomen: unilateral, bilateral or may be generalized.
• Shoulder tip pain (25%) (referred pain due to diaphragmatic irritation from hemoperitoneum) may be
present.
• Vaginal bleeding may be slight and continuous. Expulsion of decidual cast (5%) may be there
• Vomiting, fainting attack. Syncopal attack (10%) is due to reflex vasomotor disturbances following
peritoneal irritation from hemoperitoneum.
19.
SIGNS/ CLINICAL FINDINGS
•General look (diagnostic): The patient lies quiet and conscious, perspires and looks blanched.
• Pallor: Severe and proportionate to the amount of internal hemorrhage.
• Features of shock: Pulse—rapid and feeble, hypotension, extremities—cold clammy.
• Abdominal examination: Abdomen (lower abdomen)—tense, tumid, tender. No mass is usually
• felt, shifting dullness present, bowels may be distended. Muscle guard—usually absent.
• Pelvic examination is less informative due to extreme tenderness and it may precipitate more intraperitoneal hemorrhage
due to manipulation.
• The findings are:
• (i) Vaginal mucosa—blanched white.
• (ii) Uterus seems normal in size or slightly bulky.
• (iii) Extreme tenderness on fornix palpation or on movement of the cervix(75%)
• (iv) No mass is usually felt through the fornix.
• (v) The uterus floats as if in water.
• Caution: Vaginal examination may precipitate more hemorrhage
due to manipulation.
20.
UNRAPTURED ECTOPIC PREGNANCY
•Symptoms:
• Presence of delayed period or spotting with features suggestive of pregnancy.
• Uneasiness on one side of the flank which is continuous or at times colicky in nature.
• Signs: Bimanual examination:
• (i) Uterus is usually soft showing evidence of early pregnancy.
• (ii) A pulsatile small, well-circumscribed tender mass may be felt through one fornix
separated from
the uterus.
• The palpation should be gentle, else rupture may precipitate and massive intraperitoneal
hemorrhage when shock and collapse may occur dramatically.
21.
CHRONIC OR OLDECTOPIC
• Onset: The onset is insidious. The patient had previous attacks of acute pain from which she had recovered
or she had chronic features from the beginning.
• Symptoms:
• Amenorrhea: Short period of 6-8 weeks is usually present.
• Lower abdominal pain is present with varying degrees.
• It starts as an acute one and gradually becomes dull or colickyin nature.
• Vaginal bleeding appears sooner or later following the pain.
• It is scanty, sanguinous or dark-colored and continuous in nature. Expulsion of decidual cast may be present
• Other symptoms:
• Bladder irritation—dysuria, frequency or even retention of urine.
• Rectal tenesmus may appear especially following infected hematocele
• Rise of temperature may be due to infection or due to absorption of the products of degenerated blood
accumulated in the abdomen.
22.
CONTINUATION….
• On examination(signs):
• The patient looks ill.
• Pallor varying degree is present.
• Pulse persistently high even during rest—a conspicuous finding.
• Features of shock are absent.
• Temperature may be slightly elevated to 38°C.
• Abdominal examination:
• (i) Tenderness and muscle guard on the lower abdomen especially on the affected side are a
striking feature.
• (ii) A mass in the lower abdomen may be felt which is irregular and tender.
• (iii) Cullen‘s sign—Dark bluish discoloration around the umbilicus, if found, suggests
intraperitoneal hemorrhage.
23.
INVESTIGATIONS FOR THEDIAGNOSIS OF TUBAL ECTOPIC PREGNANCY
• Blood examination: (i) CBC. (ii) ABO and Rh grouping.
• Culdocentesis
• Estimation of β-hCG: Urine pregnancy test—ELISA is sensitive to 10-50 mIU/mL and is positive in 95% of ectopic
pregnancies. A single estimation of β-hCG level either in the serum or in urine confirms pregnancy but
cannot determine its location. The suspicious findings are:
(1) Lower concentration of β-hCG compared to normal intrauterine pregnancy
(2) Doubling time in plasma fails to occur in 2 days.
• Sonography: Transvaginal sonography (TVS) is more informative. The diagnostic features are:
(1) Absence of intrauterine pregnancy with a positive pregnancy test.
(2) Fluid (echogenic) in the pouch of Douglas.
(3) Adnexal mass clearly separated from the ovary.
(4) Rarely cardiac motion may be seen in an unruptured tubal ectopic pregnancy.
Color Doppler Sonography: (TV-CDS)—can identify the placental shape (ring-of-fire pattern) and enhanced blood
flow pattern outside the uterine cavity.
24.
CONTINUATION…
• Laparoscopy
• D& C—Identification of decidua without villi structure is very much suggestive. Chorionic villi
that float in normal saline as lacy fronds are diagnostic of intrauterine pregnancy.
• Serum progesterone—Level greater than 25 ng/mL is suggestive of viable intrauterine
pregnancy whereas level less than 5 ng/mL suggests an ectopic or abnormal intrauterine
pregnancy.
• Laparotomy offers benefit when in doubt. The old axiom, “open and see” holds good
especially when the patient is hemodynamically unstable. “One should not be ashamed of
having a negative abdominal exploration, rather to be disgraced for the mistake in
diagnosis with the eventual fatality.”
25.
DIFFERENTIAL DIAGNOSIS OFSUBACUTE ECTOPIC PREGNANCY:
• Incomplete abortion
• Salpingitis
• Appendicitis
• Twisted ovarian tumor
• Ruptured chocolate cyst of the ovary.
• Ruptured corpus luteum:Clinical presentation is similar to tubal rupture but pregnancy test is
negative.
26.
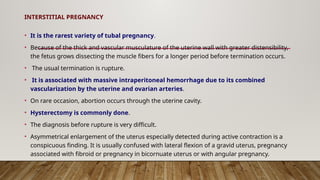
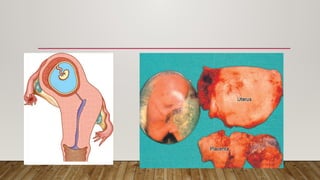
INTERSTITIAL PREGNANCY
• Itis the rarest variety of tubal pregnancy.
• Because of the thick and vascular musculature of the uterine wall with greater distensibility,
the fetus grows dissecting the muscle fibers for a longer period before termination occurs.
• The usual termination is rupture.
• It is associated with massive intraperitoneal hemorrhage due to its combined
vascularization by the uterine and ovarian arteries.
• On rare occasion, abortion occurs through the uterine cavity.
• Hysterectomy is commonly done.
• The diagnosis before rupture is very difficult.
• Asymmetrical enlargement of the uterus especially detected during active contraction is a
conspicuous finding. It is usually confused with lateral flexion of a gravid uterus, pregnancy
associated with fibroid or pregnancy in bicornuate uterus or with angular pregnancy.
28.
MANAGEMENT OF RAPTUREDECTOPIC PREGNANCY
• The principle in the management of acute ectopic is resuscitation and laparotomy and not resuscitation followed
by laparotomy.
• Antishock treatment: Antishock measures are to be taken energetically with simultaneous preparation for urgent
laparotomy.
• Ringer’s solution (crystalloid) is started
• Arrangement is made for blood transfusion. Even if blood is not available, laparotomy is to be done desperately.
• When the blood is available, it is better to be transfused after the clamps are placed to occlude the bleeding vessels on
laparotomy, as it is of little help to transfuse when the vessels are open.
• After drawing the blood samples for grouping and cross matching, volume replacement with colloids (hemaccel) is to
be done.
• Laparotomy: Indications of laparotomy are—
• (i) Patient hemodynamically unstable.
• (ii) Laparoscopycontraindicated.
• (iii) Evidence of rupture.
• The principle in laparotomy is “quick in quick out”
29.
MANAGEMENT OF UNRUPTUREDTUBAL PREGNANCY
• Expectant
• Medical
• Surgical
• Conservative
• Ablative
30.
CONTINUATION….
• Expectant management:Where only observation is done hoping spontaneous resolution.
• Indications are:
• (i) Initial serum hCG level less than 1,000 IU/L and the subsequent levels are falling.
• (ii) Gestation sac size less than 4 cm.
• (iii) No fetal heart beat on TVS.
• (v) No evidence of bleeding or rupture on TVS.
• Conservative management may be either medical or surgical. Otherwise salpingectomy is done.
• The advantages of conservative management are:
• (1) Significant reduction in operative morbidity, hospital stay as well as cost.
• (2) Improved chance of subsequent intrauterine pregnancy
• (3) Less risk of recurrence.
31.
MEDICAL MX…
• Numberof chemotherapeutic agents have been used either systemic or direct local (under
sonographic or laparoscopic guidance) as medical management of ectopic pregnancy.
• The drugs commonly used for salpingocentesis are: methotrexate, potassium chloride,
prostaglandin
• (PGF2), hyperosmolar glucose or actinomycin.
Requirements For Medical Mx
• (i) Hemodynamically stable.
• (ii) Serum hCG level should be less than 3,000 IU/L.
• (iii) Tubal diameter should be less than 4 cm without any fetal cardiac activity.
• (iv) There should be no intra-abdominal hemorrhage.
32.
CONTINUATION…
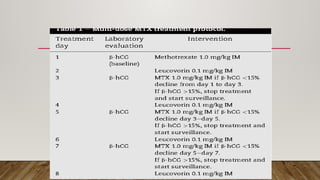
• For systemictherapy, a single dose of methotrexate (MTX) 50 mg/M2 is given intramuscularly.
• Monitoring is done by measuring serum b-hCG on D4 and D7.
• When the decline in hCG between D4 and D7 is greater than or equal to 15%, patient is
followed up weekly with serum hCG until hCG less than 10 mIU/mL. If the decline is less than
15%, a second dose of MTX 50 mg/M2 is given on D7.
• Variable dose methotrexate (MTX) includes: MTX – 1 mg/kg IM on D1,3,5,7 and Leucovorin
0.1 mg/kg IM on D2,4,6,8.
• Serum b-hCG is monitored weekly until less than 5.0 mIU/mL.
34.
CONTRAINDICATIONS OF METHOTREXATE
•MTX sensitivity
• Tubal rupture
• Breastfeeding
• Intrauterine pregnancy
• Peptic ulcer disease
• Active pulmonary disease
• Immunodeficiency
• Hepatic, renal, or hematologic dysfunction
• N/B: MTX is highly effective against rapidly proliferating trophoblast. However, gastrointestinal
mucosa, bone marrow, and respiratory epithelium also can be harmed.
• Baseline tests ie CBC, U/E/Cs, LFTS and Rh have to be done prior to administration of MTX
35.
CONSERVATIVE SURGERY
• Theprocedure can be done either laparoscopically or by microsurgical laparotomy.
• Indications:
• (a) Cases not fulfilling the criteria of medical therapy.
• (b) Cases where b-hCG levels are not decreasing despite medical therapy.
• (c) persistent fetal cardiac activity
36.
TYPES OF CONSERVATIVESURGERIES
• 1. Linear Salpingostomy: A longitudinal incision is made on the antimesenteric border directly over the site
of ectopic pregnancy. After removing the products, the incision line is kept open to be healed later on by
secondary intention. Hemostasis is achieved by electrocautery or laser.
• 2. Linear Salpingotomy: The procedures are the same as those of salpingostomy. But the incision line is
closed in two layers with 7-0 interrupted vicryl sutures. This is not commonly done.
• 3. Segmental Resection: This is of choice in isthmic pregnancy. End-to-end anastomosis can be done
immediately or at a later date after appropriate counseling of the patient.
• 4. Fimbrial Expression: This is ideal in cases of distal ampullary (fimbrial) pregnancy and is done digitally.
• Following conservative surgery or medical treatment, estimation of b-hCG should be done weekly till the
value becomes less than 5.0 mlU/mL. Additional monitoring by TVS is preferred.
• Following laparoscopic salpingostomy, persistent ectopic pregnancy ranges between 4% and 20%.
PERSISTENT ECTOPIC PREGNANCY
•This is due to incomplete removal of trophoblast.
• It is high after fimbrial expression and in cases where initial serum b-hCG level is greater than 3,000 IU/L.
• Prophylactic single dose MTX (1 mg/kg) IM is effective to resolve the problem.
N/B :Rh-NEGATIVE WOMEN: In Rh-negative women not yet sensitized to Rh antigen, anti-D gamma
globulin— 50 μg (if gestation < 12 weeks) or 300 μg (if > 12 weeks) intramuscularly is administered soon
following operation to prevent isoimmunization.
• PROGNOSIS OF TUBAL PREGNANCY:
• Immediate prognosis so far as maternal mortality is concerned has been markedly reduced (0.05%) due to
early diagnosis, adequate blood replacement and surgery even in desperately ill patient.
• An ectopic mother has got every chance of a viable birth in 1 in 3 and a chance of recurrence of ectopic in 1 in
10.
• Patient is asked to report after she misses her period to confirm and to locate the new pregnancy.
39.
PREVENTION OF RECURRENCEOF TUBAL PREGNANCY
• Incidence of subsequent intrauterine pregnancy (IUP) is 60–70%, in women with unruptured
tubal ectopic pregnancy treated by conservative surgery.
• The incidence of subsequent ectopic pregnancy is about 10–20% and successful conception is
about 60%.
• Salpingostomy done for unruptured tubal ectopic pregnancy does not increase the risk of
ectopic pregnancy compared to salpingectomy.
• Conservative surgery for unruptured tubal ectopic pregnancy is beneficial.
• Future advice: Main concern is the risk of recurrence. Whenever there is amenorrhea,
pregnancy test is done and if positive, high resolution TVS is done to know the site of
pregnancy.
40.
MEDICAL VERSUS SURGICALTHERAPY
• Medical or surgical management offer similar outcomes in women who are hemodynamically
stable, have
serum β-hCG concentrations <5000 mIU/mL, and have a small pregnancy with no cardiac
activity.
• Despite lower success rates with medical therapy for women with larger tubal size, higher
serum β-hCG
levels, and fetal cardiac activity, medical management can be offered to the motivated
woman who
understands the risks of emergency surgery in the event of treatment failure.
• For single-dose MTX, its efficacy compared with laparoscopic salpingostomy shows conflicting
results.
41.
ABDOMINAL PREGNANCY
• PRIMARY:Primary implantation of the fertilized ovum on the peritoneum is so rare that its existence
• is questionable.
• Studdiford criteria to diagnose primary abdominal pregnancy are:
(1) Both the tubes and ovaries are normal without evidence of recent injury.
(2) Absence of uteroperitoneal fistula.
(3) Presence of a pregnancy related exclusively to the peritoneal surface and young enough to eliminate
the possibility of secondary implantation following primary nidation in the tube.
• SECONDARY: Abdominal pregnancy is almost always secondary, the primary sites being tube, ovary or
even the uterus.
• The conceptus escapes out through the rent in the uterine scar
• The average incidence is about 1 in 3,000 pregnancies.
• With the use of ART incidence is found rising.
42.
FATE OF SECONDARYABDOMINAL PREGNANCY
• Fate of Secondary Abdominal Pregnancy
• Death of the blastocyst with complete absorption
• Massive intraperitoneal hemorrhage due to placental separation
• Infection with fistulous communication with intestine, bladder, umbilicus
• Fetal death :mummification, suppuration, adipocere formation, calcification (lithopedion)
• Continue to term pregnancy (rare—1.0%) (risk of fetal malformation and deformation)
43.
CONTINUATION…
• Symptoms:
(1) Historysuggestive of disturbed tubal pregnancy during early months (pain lower abdomen and vaginal
bleeding) is often present.
(2) Minor ailments of normal uterine pregnancy are often exaggerated such as nausea, vomiting, constipation,
pain abdomen and increased fetal movements.
• Signs in advanced pregnancy:
• (1) Uterine contour is not well defined even by massaging the abdominal wall, as the Braxton-Hicks
contraction is absent in abdominal pregnancy.
• (2) Fetal parts are felt easily and persistent abnormal attitude and position of the fetus on repeated
examination is quite common.
• While abnormal high position of the fetus is commonly found in intraperitoneal pregnancy, the fetus is lying
low in intraligamentary pregnancy.
• Internal examination:
• The uterus is difficult to separate from the abdominal mass. If it does, it is enlarged (12–16 weeks) but the
cervix is not typically soft and is usually displaced depending upon the position of the sac.
44.
IMAGING STUDIES FORABDOMINAL PREGNANCY
• Sonography: Suggestive features are—
• Absence of uterine wall around the fetus
• Abnormally high position of fetus with abnormal attitude
• Fetal parts with close approximation to maternal abdominal wall and visualization of the uterus separately.
• Diagnostic error could be even up to 40%.
• Magnetic resonance imaging (MRI) can confirm the diagnosis and may be very accurate.
• Computed tomography is diagnostic and is superior to MRI. CT has the risk of radiation.
• X-ray examination:
• (a) Abnormally high position of the fetus with absence of outline of uterine shadow.
• (b) Superimposition of gas shadow on the fetal skeleton.
• (c) Lateral X-ray on standing position shows superimposition of fetal skeleton shadow with the maternal spinal shadow.
• Diagnosis: Its rarity, variegated clinical pictures and not keeping in mind the possibility lead to
• confusion in diagnosis. To give a positive diagnosis, the clinician should be conscious of the entity.
• Highly suggestive features:
• (1) Repeated failure of induction for intrauterine fetal death.
• (2) During induction of labor by oxytocin, uterine contraction could not be excited. Surest evidence is on laparotomy.
45.
MANAGEMENT
• Once thediagnosis is made, the opinion is almost crystallized in favor of urgent laparotomy
irrespective of period of gestation.
• The risks of continuation of pregnancy are:
• (1) Catastrophic hemorrhage.
• (2) Fetal death
• (3) Increased fetal malformation.
• (4) Increased neonatal loss (50%).
• Continuation of pregnancy for few weeks hoping the baby to become mature enough to
survive can only be justified in exceptional circumstances.
During the period, the patient should be in the hospital.
46.
CONTINUATION….
• Laparotomy:
• Theideal surgery is to remove the entire sac-fetus, the placenta and the membranes.
• This may be achieved if the placenta is attached to a removable organ like uterus or broad ligament.
• If, however, the placenta is attached to vital organs, it is better to take out the fetus and leave behind the
• placenta and the sac, after tying and cutting the cord flushed with its placental attachment.
• In such a situation, placental activity is to be monitored by quantitative serum b-hCG level and ultrasound.
• Complete absorption of the left behind placenta occurs through aseptic autolysis.
• Complications include: secondary hemorrhage, intestinal obstruction and infection.
• Prognosis: Because of the risk mentioned before maternal mortality is less than 5% but morbidity is high.
• Perinatal mortality approximates 90%.
• Fetal malformation could be as high as 50%.
• Normal infants have been reported in 10% of cases.
47.
OVARIAN PREGNANCY
• Spiegelberg‘scriteria in diagnosis of ovarian pregnancy are:
• (1) Tube on the affected side must be intact.
• (2) The gestation sac must be in the position of the ovary.
• (3) The gestation sac is connected to the uterus by the ovarian ligament.
• (4) The ovarian tissue must be found on its wall on histological examination.
• The embedding may occur intrafollicular or extrafollicular. In either types, rupture is an
inevitable
• phenomenon and salpingo-oophorectomy is the definite surgery.
• Ovarian resection could be done when the diagnosis is made early.
CONTINUATION…
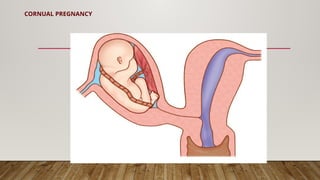
• Cornual Pregnancyis pregnancy occurring in rudimentary horn of a bicornuate uterus.
• The horn does not usually communicate with the uterine cavity.
• The impregnation is presumed to occur by a spermatozoa which passes through the normal
half of the uterus and tube.
• It then fertilizes an ovum either in the peritoneal cavity or in the tube connected to the
rudimentary horn by transperitoneal migration.
• The concerned ovum is usually shed from the ovary on the same side of the rudimentary
horn.
• The general and local reactions are similar to those in the tubal pregnancy. But these are
intensified and pregnancy may continue for longer time.
• Termination by rupture is inevitable between 12 and 20 weeks with massive
intraperitoneal hemorrhage.
50.
CONTINUATION…
• The diagnosisis seldom done before the catastrophe.
• The condition is commonly diagnosed as fibroid or ovarian tumor with pregnancy.
• Even on laparotomy, the exact position is confused with interstitial pregnancy.
• Position of the round ligament which is attached to the sac and the long pedicle by
which it is attached to the uterus are the diagnostic points.
• Surgery includes removal of the rudimentary horn.
• If the pedicle is short and the attachment is wide, hysterectomy may have to be done.
51.
CERVICAL PREGNANCY
• Thisis a rare (1 in 16,000 pregnancies) variant of ectopic pregnancy when the implantation occurs in the
cervical canal at or below the internal os.
• Erosion of the walls by the trophoblasts occurs resulting in thinning and distension of the canal. The
• condition is commonly confused with cervical abortion.
• In cervical pregnancy, the bleeding is painless and the uterine body lies above the distended cervix.
• Intractable bleeding following evacuation or expulsion of the products brings about suspicion.
• The morbidity and mortality is high because of profuse hemorrhage.
• Clinical diagnostic criteria (Rubin–1983) for cervical pregnancy :—
• (a) Soft, enlarged cervix equal to or larger than the fundus.
• (b) Uterine bleeding following amenorrhea, without cramping pain.
• (c) Products of conception entirely confined within and firmly attached to endocervix.
• (d) A closed internal cervical os and a partially opened external os.
52.
CONTINUATION…
• Sonography:
• Revealsthe pregnancy in the cervical canal and an empty uterine cavity.
• Hysterectomy is often required to stop bleeding.
• An attempt to preserve the uterus may be made by intracervical plugging.
• Methotrexate therapy has been considered both systemic and direct local as an alternative or
adjunct to hysterectomy.
• Uterine artery embolization with gelfoam can control hemorrhage.
• Confirmation is done by histological evidence of the presence of villi inside the cervical
stroma.
54.
• Pregnancy ofunknown location:
• No sign of either intra- or extrauterine pregnancy or retained products of conception in a
woman with a positive pregnancy test.
• Pregnancy of uncertain viability: Intrauterine gestation sac (<20 mm mean diameter) with
no obvious yolk
• sac or fetus or fetal echo less than 6 mm crown-rump length with no obvious fetal heart
activity.
• In order to confirm or refute viability, a repeat scan at a minimal interval of 1 week is
necessary.
55.
HETEROTOPIC PREGNANCY
• Incidenceis about 1 in 8,000 pregnancies at present.
• It is more common following ART procedures.
• Intrauterine pregnancy may be coexistent with tubal or rarely with cervical or ovarian
pregnancy.
• Diagnosis is difficult.
• Absence of vaginal bleeding in the presence of signs and symptoms of an ectopic pregnancy
is suspicious.
• Abnormally rising hCG level and ultrasonography may be helpful.
56.
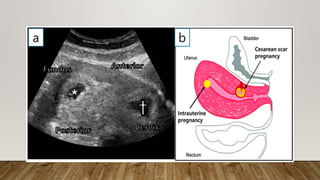
CESAREAN SCAR PREGNANCY[CSP]
• Tis term describes implantation within the myometrium of a prior cesarean delivery scar.
• Its incidence approximates 1 case in 2000 normal pregnancies and has increased along with
the cesarean delivery rate.
• Women with symptomatic cesarean scar pregnancy (CSP) usually present early, and pain and
bleeding are common.
• 40 percent of women are asymptomatic, and the diagnosis is made during routine
sonographic examination.
TYPES OF CSPs
1. Endogenic CSPs implant on the scar and expand toward the uterine cavity
2. Exogenic CSPs implant deeply within the scar niche and grow toward the bladder or
abdominal cavity
57.
INVESTIGATION AND DX
•Sonographically, differentiating between an IUP implanted at the cervicoisthmic junction and
a CSP can be difficult.
• Investigators in one study marked the midpoint of the uterine length (cervix to fundus) in
sagittal views. If the center of the gestational sac lay distal to this midpoint, a CSP was
diagnosed.
59.
CONTINUATION
• Growing evidencesuggests that some of these pregnancies will not behave as a typical ectopic
pregnancy and rupture rates are lower.
• CSPs are thought by some to be a precursor of PAS (Placenta Accreta Syndrome).
• A significant percentage of affected pregnancies will progress to a viable-aged neonate, albeit with the
complications associated with PAS
• Patients may prefer to avoid rupture and PAS risks and seek
• pregnancy termination.
• The most successful operations include:
• (1) Laparoscopic uterine isthmic resection
• (2) Transvaginal isthmic resection through an anterior colpotomy, created similarly to anterior entry
during vaginal hysterectomy.
• (3) UAE, followed by D & C with or without hysteroscopy;
• (4) Hysteroscopic resection
60.
CONTINUATION…
• The SocietyFor Maternal-Fetal Medicine (SMFM) (2020) considers sonography-guided vacuum
aspiration alone, but not sharp curettage, to be suitable.
• In some instances, hysterectomy is required or may be elected in those not desiring future fertility.
Medical Management
• Medical management is an option for those hoping to avoid surgery.
• However, compared with surgery, pregnancy resolution rates are more varied and lengthier.
• In one review, local MTX injection into the gestational sac alone provided a success rate of 60
percent, and systemic plus local MTX raised the rate to nearly 80 percent.
• Following conservative treatment, subsequent pregnancies have good outcomes, but PAS and
recurrent CSP are risks.
• Uterine arteriovenous malformations are a potential long-term complication
61.
CONTINUATION…
• Women acceptingexpectant care are ideally well counseled on the potential obstetric
complications.
• If not prompted by earlier complications, repeat cesarean delivery is recommendedat 34 0/7
and 35 6/7
• weeks’ gestation, and this timing recognizes the PAS and uterine rupture risks associated with
CSP.
• Betamethasone to hasten lung maturity is recommended prior to delivery.

![TYPES OF ECTOPIC PREGNANCIES
Acute ectopic pregnancy [30%]
• Acute ectopic pregnancies are more common, produce a high serum β-hCG level, and grow rapidly,
leading to a timely diagnosis.
• These carry a greater risk of rupture.
• Mostly presents as raptured ectopic pregnancy with massive hemoperitoneum
Chronic Ectopic Pregnancy
• With chronic ectopic pregnancy, abnormal trophoblasts die early, and thus serum β-hCG levels are
negative or are low and static.
• Chronic ectopic pregnancies typically rupture late, at all, but commonly form a persistent complex
pelvic mass.
• This sonographic finding, rather than patient symptoms, often is the reason that prompts
diagnostic surgery](https://image.slidesharecdn.com/ectopicpregnancy-250802092738-4004b57f/85/ECTOPIC-PREGNANCY-PowerPoint-Presentation-pptx-11-320.jpg)

![CESAREAN SCAR PREGNANCY [CSP]
• Tis term describes implantation within the myometrium of a prior cesarean delivery scar.
• Its incidence approximates 1 case in 2000 normal pregnancies and has increased along with
the cesarean delivery rate.
• Women with symptomatic cesarean scar pregnancy (CSP) usually present early, and pain and
bleeding are common.
• 40 percent of women are asymptomatic, and the diagnosis is made during routine
sonographic examination.
TYPES OF CSPs
1. Endogenic CSPs implant on the scar and expand toward the uterine cavity
2. Exogenic CSPs implant deeply within the scar niche and grow toward the bladder or
abdominal cavity](https://image.slidesharecdn.com/ectopicpregnancy-250802092738-4004b57f/85/ECTOPIC-PREGNANCY-PowerPoint-Presentation-pptx-56-320.jpg)




























![ECHO Presentation DM in Pregnancy [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/echopresentationdminpregnancyautosaved-250802092504-6298dc81-thumbnail.jpg?width=640&height=640&fit=bounds)






































