The document provides an overview of Alzheimer's disease (AD), including:
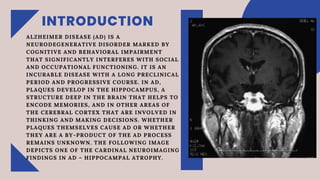
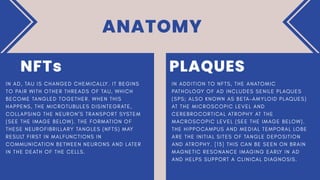
- AD is a neurodegenerative disorder marked by cognitive and behavioral impairment. It develops plaques in the hippocampus and other brain areas involved in thinking and memory.
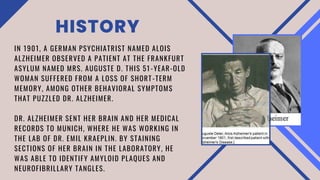
- Alois Alzheimer first observed the hallmark plaques and tangles in the brain of a patient in 1901. AD causes the death of brain cells and leads to atrophy in areas like the hippocampus.
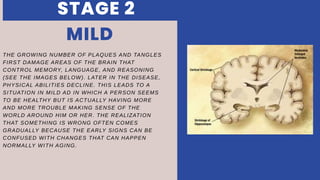
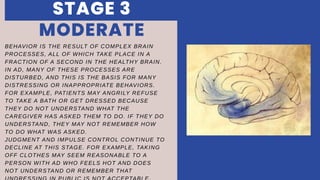
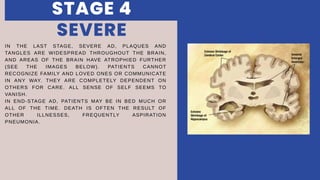
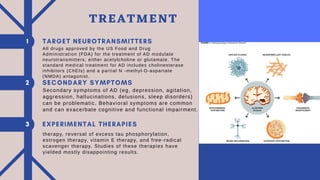
- AD progresses through preclinical, mild, moderate, and severe stages as plaques and tangles spread and damage more brain regions. Symptoms worsen from memory loss to complete dependence. Approved medications can temporarily slow symptoms.
- Counseling patients