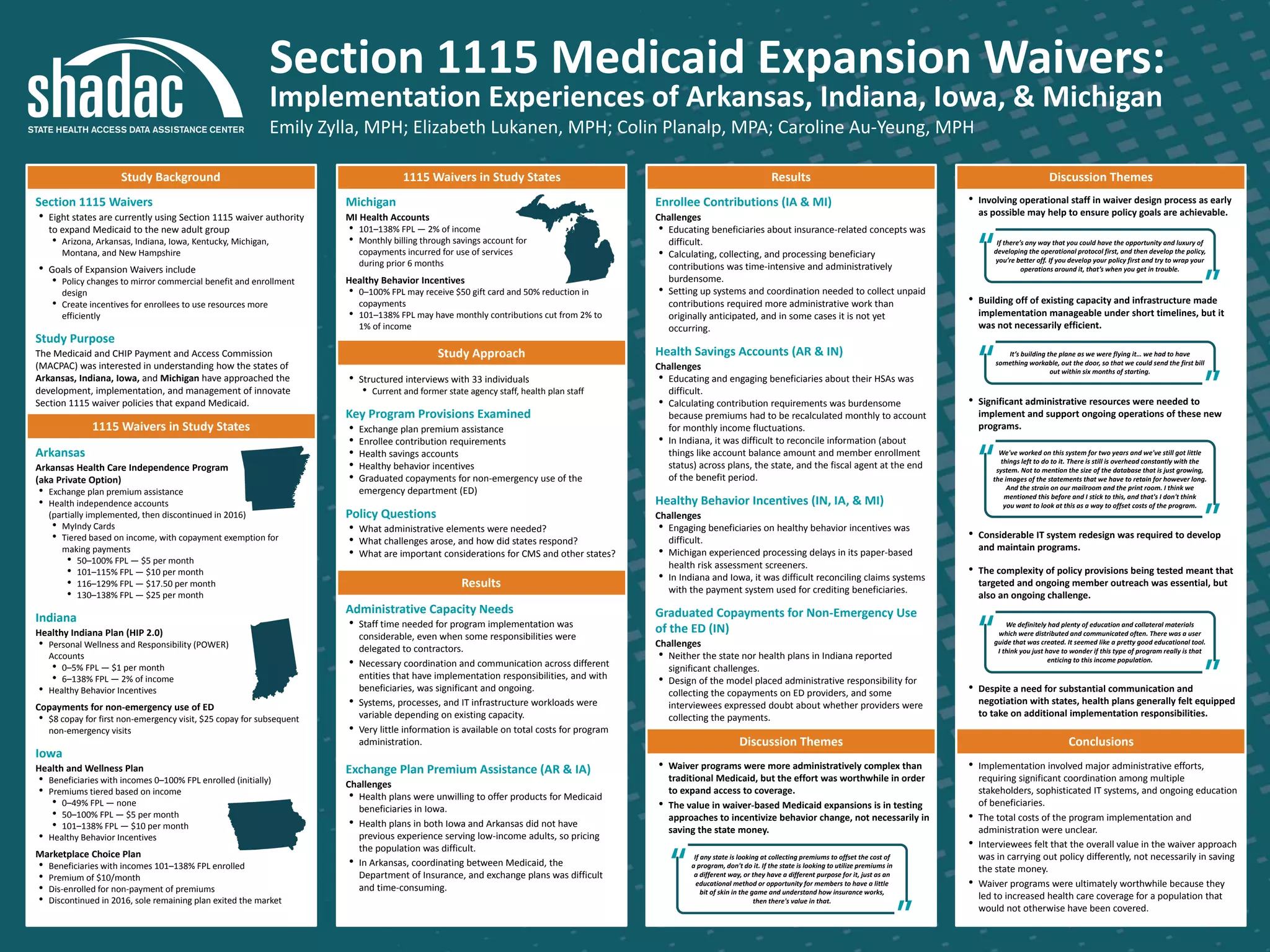
- Structured interviews were conducted with 33 current and former state agency and health plan staff across 4 states to understand challenges implementing Section 1115 Medicaid expansion waiver programs.
- Key challenges included the significant administrative resources and coordination required across entities, educating enrollees, and reconciling complex program rules across systems.
- While waiver programs allowed for innovative policy testing, the administrative complexity was substantial and ongoing. Implementation involved major efforts to develop new IT systems and operational protocols within tight timelines.








































































![ict_presentation_final_final_final[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/ictpresentationfinalfinalfinal1-251230145259-2b4839bd-thumbnail.jpg?width=640&height=640&fit=bounds)














