POST OPERATIVE COMPLICATIONS
Student:Maj Adil A Kalam
Guide: Lt Col SK Dey
“A surgeon who has no complications is
either not operating or is being economical
with the truth”
4.
INTRODUCTION
• The cost
•Lost work productivity
• Disruption of family life
• Stress to employers and society in general.
• Functional results -compromised
(preoperative level of function.)
• Anticipating an uneventful operation but
compromised by the complication
Avoiding complications- Preop
•Careful preoperative screening.
• Nutritional status
• Health of the heart and lungs.
• Appropriate operation
• Timing of the operation-elective vs urgent
• Weight
• Preoperative consultation from a cardiologist
or pulmonary specialist
7.
• Handle tissuesgently, dissect meticulously,
and honor tissue planes.
• Avoid the temptation to rush, cut corners, or
accept marginal technical results.
• Judicious use of antibiotics and other
preoperative medications
Avoiding complications- Intraop
8.
• Compulsive postoperativesurveillance
• Be vigilant and seek postoperative complications at an
early stage,
– checks all wounds
– evaluates intake and output
– checks temperature profiles,
– ascertains what the patient’s activity levels have been,
– Evaluates nutritional status
– checks pain levels.
• Deviations from the normal course- Experience
Avoiding complications- Postop
SEROMA
• Collection-liquefied fat,serum,& lymphatic fluid
• Most benign complication
• Large skin flaps
– Mastectomy
– Axillary Dissection
– Groin Dissection
– Large ventral Hernia repairs
• Swelling/discomfort/drainage
• Prevention- suction drain under flaps
12.
• Treatment
– Aspiration+Pressurebandage
– Recumilating after 2 aspirations- Open and pack
– Synthetic mesh- Open and suction drain
– Infected seroma- Open
– Mesh Explantation?
SEROMA
13.
“The most importantclotting factor is the
surgeon”-Moshe schein
“Operative atlases never bleed”
HEMATOMA
14.
HEMATOMA
• Abnormal collectionof blood
• More potential for secondary infection
• Causes
inadequate hemostasis
depletion of clotting factors
presence of coagulopathy
Diseases and medications that contribute to
coagulopathy
15.
HEMATOMA
• PRESENTATION
Varieswith size, location, presence of infection
Expanding, unsightly swelling or pain in area of surgical
incision
Neck- compromise of airway
Retroperitonium- paralytic ileus, anaemia, ongoing
bleeding
Extremity and abdominal cavity- compartment syndrome
• Physical examination- localized swelling with
purplish blue discolouration, may be tender.
16.
HEMATOMA
• PREVENTION
– correctingclotting abnormalities
– Discontinuing medications that alter coagulation
• Risk of bleeding vs Thromboembolic events
• Discontinue VKA 4-5 days before surgery -INR to be
<1.5
• If INR>1.5- low dose Vit K orally(1-2mg)
• Bridging anticoagulation
– IV UFH-discontinued 4 hrs before surgery
– Therapeutic dose LMWH S/C- 16-24 hrs before surgery
• VKA- resumed 12-24 hrs after surgery(2-3 days for
17.
• Acetyl salicylicacid/Clopid-withhold 6-7 d
begore surgery
• Antiplatelet therapy resumed approximately
24 hrs after surgery
• Emergency setting!
– VKA-FFP, Low dose iv or oralVit K
HEMATOMA
18.
HEMATOMA
• Evaluation- assessmentof risk factors and
coagulation parameters
• Small hematoma- eventually resorbs
• Retroperitoneal hematoma-expectant waiting
after associated coagulopathy
• Expanding hematoma in neck- evacuated in
the operating room after securing airway if
there is any respiratory compromise.
ACUTE WOUND FAILURE(DEHISCENCE)
•Postoperative separation of the abdominal
musculoaponeurotic layers
• Risk of evisceration, repeat dehiscence, surgical
wound infection, incisional hernia formation.
• 1-3% patients undergoing abdominal operations
• Can be predisposed by hematoma and infection
21.
Factors associated withwound dehiscence
• Technical error in fascial closure
• Emergency surgery
• Intra-abdominal infection
• Advanced age
• Wound infection, hematoma, and seroma
• Elevated intra-abdominal pressure
• Obesity
• Long-term corticosteroid use
• Previous wound dehiscence
• Malnutrition
• Radiation therapy and chemotherapy
• Systemic disease (uremia, diabetes mellitus)
22.
ACUTE WOUND FAILURE(DEHISCENCE
•PRESENTATION
Sudden dramatic drainage of large volume of clear, salmon
coloured fluid preceeds dehiscence in 25%patients
Ripping sensation
• PREVENTION- good fascial closure
• TREATMENT
Small dehiscence- conservatively with saline moistened gauze
packing, use of abdominal binder.
Large segment of wound that is open to the omentum and
intestines, if there is peritonitis or interstitial leak-Explore
Management of infection
23.
ACUTE WOUND FAILURE(DEHISCENCE)
•Management of incision
Fascia strong and intact- primary closure
Fascia Infected and necrotic-debridement
Can be Closed with retention sutures, use of
prosthetic material may be preferred
Closure with an absorbable mesh- associated with
fistula formation and hernia formation repair.
Skin graft applied after granulation of wound
Hernia-removal of skin graft and permanent
prosthesis or dermabration of skin graft followed by
facial closure using component separation
24.
SURGICAL SITE INFECTION
(WOUNDINFECTION)
• The surgical wound encompasses the area of
the body, internally and externally, that
involves the entire operative site.
• Wounds are generally categorized as follows:
1. Superficial-skin and subcutaneous tissue
2. Deep-fascia and muscle
3. Organ space-internal organs included in operation
27.
SURGICAL SITE INFECTION
(WOUNDINFECTION)
• PRESENTATION
5-6 days post operatively, may vary
Approximately 80-90%of all post operative infections
occur within 30 days after surgery.
• SSIs are accompanied by
Erythema
Tenderness
Occassionally discharge
Leucocytosis
Low grade fever
SURGICAL SITE INFECTION
(WOUNDINFECTION)
• Prevention
Stop smoking at least 30 days before surgery
Blood glucose levels maintained
Malnourished patients given nutritional
supplements
Obese patients encouraged to lose weight
Bowel preparation for major abdominal surgeries
Perioperative antibiotiics
30.
SURGICAL SITE INFECTION
(WOUNDINFECTION)
•preoperative dose, intraoperative doses approximately 4 hours apart, and two
postoperative doses appropriately spaced.
•prophylactic -intravenously within 30 minutes before the incision-therapeutic
tissue levels -when the wound exposed to bacterial contamination
31.
SURGICAL SITE INFECTION
(WOUNDINFECTION)
1. Careful handling of tissues
2. Meticulous dissection, hemostasis, and débridement
of devitalized tissue
3. Compulsive control of all intraluminal contents
4. Preservation of blood supply of the operated organs
5. Elimination of any foreign body from the wound
6. Maintenance of strict asepsis
7. Thorough drainage and irrigation with warm saline of
any pockets of purulence in the wound
8. Patient kept in euthermic state and fluid-resuscitated
9. Expressing a decision about closing the skin or packing
the wound at the end of the procedure
32.
SURGICAL SITE INFECTION
(WOUNDINFECTION)
• TREATMENT
Depends on depth of infection
Skin staples removed and a cotton tip applicator easily
passed into the wound, with efflux of purulent material
and puss. Wound explored.
If fascia intact- debridement of any non viable tissue-
irrigated-packed
If widespread cellulitis and significant signs of infection-
IV antibiotics.
Wound cultures are controversial.
Doubtful about amount of contamination- close
observation of wound followed by closure of skin or
HYPOTHERMIA
• CAUSES
Preoperatively, intraoperativelyor postoperatively
Trauma patient with injuries in a cold environment
Paralysis-because of loss of shiver mechanism
In patients undergoing rapid resuscitation with cool IV fluids,
transfusions, or inracavitary irrigation with cold irrigant.
Patients undergoing prolonged surgical procedures.
Almost all anesthetics impair thermoregulation.
Propofol- vasodilation- redistribution hypothermia
Postoperatively
o Cool ambient room temperature
o Rapid administration of IV fluids or blood
o Failure to keep patients covered
35.
HYPOTHERMIA
• PRESENTATION
Intense coldsensation and shivering.
Associated with profound affects on CVS, coagulation, wound
healing, and infection.
Core temperature <35 degree Celsius
o Increased norepinephrine level, vasoconstriction and elevated blood
pressure.
o Increases incidence of postoperative ischemia and ventricular
tachyarrhythmia.
Poor perfusion of peripheral organs and tissues.
Increased risk of bleeding
Poor wound healing and infection.
Relative diuresis, compromised hepatic function
Severe cases- significant cardiac slowing and may be comatose, with
low blood pressure, bradycardia, and a very low respiratory rate.
36.
HYPOTHERMIA
• PREVENTION
Monitoring coretemperature
Sites
o Pulmonary artery blood
o Tympanic membrane
o Esophagus and pharynx
o Rectum
o Urinary bladder
Keeping patient warm by increasing the ambient
temperature and using heated humidifiers and warmed
IV fluids.
37.
HYPOTHERMIA
• TREATMENT
Attention mustbe directed toward rewarming by the
following methods:
1. Immediate placement of warm blankets as well as
currently available forced-air warming devices
2. Infusion of blood and IV fluids through a warming device
3. Heating and humidifying inhalational gases
4. Peritoneal lavage with warmed fluids
5. Rewarming infusion devices with an arteriovenous system
6. In rare cases, cardiopulmonary bypass
Special attention must be paid to cardiac monitoring during
the rewarming process.
38.
MALIGNANT HYPERTHERMIA
• Life-threateninghypermetabolic crisis
manifested during or after exposure to a
triggering general anesthetic in susceptible
individuals.
• Autosomal dominant disease with variable
penetrance
• Mutation resulting in altered calcium
regulation in skeletal muscle
39.
MALIGNANT HYPERTHERMIA
Halogenated inhalationalanesthetic agents (e.g., halothane, enflurane, isoflurane,
desflurane, and sevoflurane) and depolarizing muscle relaxants (e.g., succinylcholine,
suxamethonium) cause an increase in the myoplasmic Ca2+ concentration.
Exposed to
triggering
anesthetic
Abnormal release
of calcium
Prolonged activation of
muscle filaments
culminating in rigidity
and hyper metabolism
Uncontrolled
glycolysis and
aerobic metabolism
Cellular hypoxia,
progressive lactic
acidosis, and
hypercapnia
Continuous muscle
activation with ATP
Excessive
generation of
heat
Myocyte death and
rhabdomyolisis result in
hyperkalemia and
myoglobinuria
40.
MALIGNANT HYERTHERMIA
• PREVENTION
–Identify risked individuals before surgery- history,
tendency to develop fever, muscular disease,
intolerance to caffeine.
– Caffeine and halothane contraction test
– Trigger free anaesthetic-barbiturate,
benzodiazepine, opiod, propofol, ketamine, non
depolarizing neuromuscular blocker.
41.
MALIGNANT HYERTHERMIA
• PRESENTATION
–Abortive form of MH (e.g., tachycardia, arrhythmia,
increased temperature, acidosis).
– Other patients, after intubation with succinylcholine-- loss
of twitches on neuromuscular stimulation and develop
muscle rigidity.
– An inability to open the mouth-masseter spasm
pathognomonic early sign-indicates susceptibility to MH.
– Tachypnea, hypercapnia, skin flushing, hypoxemia,
hypotension, electrolyte abnormalities, rhabdomyolysis,
and hyperthermia.
42.
MALIGNANT HYPERTHERMIA
• MANAGEMENT
DISCONTINUE
TRIGGERING
ANAESTHETIC
HYPERVENTILATE
WITH100
PERCENT OXYGEN
ADMINISTER
ALTERNATIVE
ANAESTHESIA
TERMINATE
SURGERY
DANTROLENE,
2.5MG/KG, AS A
BOLUS AND REPEAT
EVERY 5 MINUTES
1-2MG/KG UNTIL
NORMALISATION OR
DISSAPEARANCE OF
SYMPTOMS
CHECK AND MONITOR
ARTERIAL BLOOD GAS AND
CREATINE KINASE,
ELECTROLYTE, LACTATE AND
MYOGLOBIN LEVELS.
MONITOR ECG,
VITAL SIGNS AND
URINE OUTPUT
ADJUNCTIVE AND
SUPPORTIVE
MEASURES ARE
CARRIED OUT
43.
DANTROLENE!
• DANTROLENE isa muscle relaxant.
– In the solution form- highly irritating to the vein- administered in a large
vein.
– IV dantrolene blocks up to 75% of skeletal muscle contraction and never
causes paralysis.
– Plasma elimination half-life is 12 hours.
– Metabolized in the liver to 5-hydroxydantrolene-also acts as a muscle
relaxant.
– Side effectsmuscle weakness, phlebitis, respiratory failure, GI
discomfort, hepatotoxicity, dizziness, confusion, and drowsiness.
• AZUMOLENE, is 30 times more water-soluble than and equipotent
to dantrolene in the treatment of MH; similar to dantrolene, it does
not affect the heart. Its main side effect is marked pulmonary
hypertension. However, azumolene is not in clinical use at this time.
44.
MALIGNANT HYPERTHERMIA
ADJUNCTIVE ANDSUPPORTIVE MEASURES
Volatile vaporizers are removed from the anesthesia machine.
Carbon dioxide canisters, bellows, and gas hoses are changed.
Surface cooling is achieved with ice packs and core cooling with cool
parenteral fluids.
Acidosis is monitored and treated with sodium bicarbonate.
Arrhythmias are controlled with beta blockers or lidocaine.
Urine output more than 2 mL/kg/hr is promoted; furosemide (Lasix) or
mannitol and an infusion of insulin and glucose (0.2 U/kg in a 50% glucose
solution) are given for hyperkalemia, hypercalcemia, and myoglobulinuria.
Patient transferred to ICU to monitor for recurrence
45.
POST OPERATIVE FEVER
•Fever is an increase in core temperature, the
modulation of which is managed by the
anterior hypothalamus.
• Stimulation of production of cytokines.
• The inflammatory responseproduction of
various mediators induce a febrile
inflammatory response, also known as
systemic inflammatory response syndrome.
POST OPERATIVE FEVER
•The most common infections are health care–associated
infections—SSI, urinary tract infection (UTI), intravascular
catheter–related bloodstream infection (CR-BSI), and
pneumonia.
• UTI
– A major predisposing factor-presence of a urinary catheter-
increased duration of catheterization (>2 days).
– Endogenous bacteria (colonic flora, most common E. coli) are the
most common source.
– Candiduria accounts for approximately 10% of nosocomial UTIs.
– The presence of an indwelling catheter, diabetes mellitus, use of
antibiotics, advanced age, and underlying anatomic urologic
abnormalities are risk factors for candiduria.
48.
POST OPERATIVE FEVER-CR-BSI
•The use of central venous catheters
• Microorganisms that colonize t he hubs or from
contamination of the injection site of the CVC(intraluminal
source) or skin (extraluminal source).
• Coagulase- staphylococci, hospital acquired bacteria (e.g.,
MRSA, multidrug-resistant gram-bacilli, fungal species
[Candida albicans]) –mc organisms .
• Metastatic infections (endocarditis)-rre but serious
complication
• Risk factors -duration of CVC, patient location (outpatient
versus inpatient), type of catheter, number of lumens and
manipulations daily, emergent placement, need for TPN,
presence of unnecessary connectors.
49.
POST OPERATIVE FEVER
PRESENTATION
•High fever that fluctuates or is sustained and
that occurs 5 to 8 days after surgery is more
worrisome.
• In the first 48 to 72 hours after abdominal
surgery-atelectasis-the cause of the fever.
• Clostridial or streptococcal SSIs-fever within
the first 72 hours of surgery.
50.
POST OPERATIVE FEVER
EVALUATION
•Six “W”’s
o Wind(lungs)
o Wound
o Water(urinary tract)
o Waste(lower GI tract)
o Wonder drugs(eg. Antibiotics)
o Walker(eg. Thrombosis)
• Symptoms indicate organ system involved
o Sputum-pneumonia
o Frequency, dysuria- UTI
o Watery foul smelling diarrhea-infection with C.difficile
o Pain in the calf- DVT
51.
Wind –POD 1 to 3 Atelectasis & Pneumonia
Water – POD 3 to 5 CA- UTI
Walking- POD 4 to 8 DVT & PE
Wound-POD 5 to 7 SSI
Wonder drugs- anytime Drug fever
Physical examination- SSI, phlebitis; tenderness
on palpation of the abdomen, flank, or calf; or
cellulitis at the site of a central venous catheter.
CBC, Urinalysis and culture, CXR, Blood culture.
POST OPERATIVE FEVER
52.
POSTOPERATIVE FEVER
• Urinalysisshowing more than 105
CFU/mL
(noncatheterized) more than 103
CFU/mL
(catheterized) UTI.
• Diagnosis of CR-BSI.
– Two simultaneous blood cultures or paired blood cultures
(i.e., simultaneous peripheral and central blood cultures)
– Peripheral blood cultures--bacteremia and isolation of 15
CFUs or 102 CFUs from an IV catheter presence of CR-BSI.
– In tunneled catheters, a quantitative colony count that is 5-
fold to 10-fold higher in cultures drawn through the central
venous catheter is predictive of CR-BSI
– If paired cultures are obtained, positive culture more than 2
hours before peripheral culture (+)
53.
• After removalof the catheter, the tip may be sent for
quantitative culture.
• Serial blood cultures and a transesophageal
echocardiogram are obtained in patients with S.
aureus bacteremia and valvular heart disease,
prosthetic valve, or new onset of heart murmur.
• Patients who continue to have fever, slow clinical
progress, and no discernible external source may
require CT to r/o intra abdominal source of
infection.
54.
POST OPERATIVE FEVER
•PREVENTION-UTI
– Minimize duration of catheterization
– Maintenance of closed drainage system
– Changing catheter before blockage occurs if
prolongation required
– Use of silver alloy or impregnated catheters
– Use of protamine sulfate and chlorhexidine
55.
POST OPERATIVE FEVER
•PREVENTION-CR-BSIs
– Maximal barrier precautions and infection control
practice during insertion.
– Educational programs- use and removal of catheter-
hand hygiene, skin antisepsis, full barrier precaution,
and stopping insertion when breaks in sterile
technique occur.
– Subclavian preferred over jugular and femoral veins
– Antiseptic-impregnated and antibiotic impregnated
catheters, routine use not recommended.
56.
POST OPERATIVE FEVER
•TREATMENT
• Antipyretics
• Pneumonia suspect- empirical antibiotic therapy altered by culture results
• UTI
– Removal/replacement of catheter
– Broad spectrum antibiotics
• CR-BSI
– Removal of catheter with adjunctive antibiotic therapy,
– Alternative venous access.
– Single agent therapy- vancomycin, linezolid,emperical coveragof gram negative
bacilli and candida species.
– Catheter salvage- antibiotic lock therapy(catheter filled with antibiotic solution
for several hours)
57.
RESPIRATORY COMPLICATIONS
• GeneralConsiderations
• Atelectasis and Pneumonia
• Aspiration Pneumonitis and Pneumonia
• Pulmonary Edema, Acute Lung Injury, and
Adult Respiratory Distress Syndrome
• Pulmonary Embolism and Venous
Thromboembolism
58.
RESPIRATORY -General Considerations
•Factors -abnormal pulmonary physiology
– loss of functional residual capacity
• Abdominal distention
• Painful upper abdominal incision
• Obesity
• strong smoking history with associated COPD,
• Prolonged supine positioning
• fluid overload leading to pulmonary edema.
– Breathing pattern
– Vital Capacity reduced
59.
– 2 typesof respiratory failure
• Type 1.hypoxic-abnormal gas exchange at
alveolar level
– Ventilation perfusion mismatching and shunting
– Clinical conditions associated with- edema and sepsis
• Type 2.associated with hypercapnia and is
associated with low PaO2and high PaCO2
– Unable to eliminate Co2 adequately
– Associated with-excessive narcotic use, ARDS, altered
respiratory dynamics
RESPIRATORY -General Considerations
60.
GENERAL CONSIDERATIONS
• History,patents with increased riskposteoanterior and
lateral CXR-baseline
• Polycythemia, chronic respiratory acidosisarterial blood gas
analysis
– PaCO2 <60mmHg-increased risk
– PaCO2 >45-50mmHg- perioperative morbidity high
• Spirometry- high risk patients before surgery
– FEV1 >2 liters-unlikely to have serious pulmonary
problems.
– FEV1 < 50% of the predicted value - likely to have
exertional dyspnea.
– If bronchodilator therapy demonstrates an improvement
in breathing patterns by >15%,consider bronchodilation.
61.
ATELECTASIS AND PNEUMONIA
•Atelectasis- most common post op complication
• Pneumonia-most common nosocomial infection
• Anesthetic/abdominal incision/ postoperative
narcotics alveoli in the periphery
collapsepulmonary shunt may occurif
aggressive pulmonary toilet not donealveoli
remain collapsed buildup of secretions
secondarily infected with bacteria,
Pneumonia
62.
PNEUMONIA
• Hospital acquiredpneumonia-Pneumonia occurring more
than 48 hours after admission and without antecedent
signs of infection.
• Ventilator-associated pneumonia—pneumonia occurring
48 hours after but within 72 hours of the initiation of
ventilation.
• Health care–associated pneumonia - pneumonia
occurring in patients who were hospitalized in the last 90
days; patients in nursing facilities or frequenting a
hemodialysis unit; and patients who have received recent
antibiotics, chemotherapy, or wound care.
63.
PNEUMONIA
• FACTORS ASSOCIATEDWITH INCREASED RISK FOR PNEUMONIA
– Depressed immune status
– Concomitant disease
– Poor nutritional status
– Increased length of hospital stay
– Smoking
– Advanced age
– Uremia
– Alcohol consumption
– Prior antibiotic therapy
– Presence of an endotracheal,nasogastric (NG), or enteric tube
– Proton pump inhibitor (PPI) therapy.-Used to prevent stress ulceration,
PPI therapy increases colonization of the stomach with pathogenic
bacteria that can increase the risk of ventilator-associated pneumonia
64.
• ORGANISMS ASSOCIATEDHOSPITAL ACQUIRED
PNEUMONIA
– Streptococcus pneumoniae (colonizes upper airway)-
most common
– Haemophilus influenzae,
– Enterobacteriaceae spp. (E. coli, Klebsiella spp., and
Enterobacter spp.)
– S. aureus (mostly MRSA).
• Occasionally resistant to first generation
cephalosporins.
65.
PNEUMONIA AND ATELECTASIS
DIAGNOSIS
ATELECTASIS
– low-grade fever
– Malaise
– diminished breath sounds in the lower lung fields.
– With the use of incentive spirometry, deep breathing,
and coughing, most cases resolve without any difficulty
– If aggressive pulmonary toilet is not instituted pneumonia
PNEUMONIA
– high fever
– mental confusion
– thick secretion with coughing
– leukocytosis
– CXR - infiltrates.
– may progress rapidly to respiratory failure and require intubation.
66.
PNEUMONIA AND ATELECTASIS
•Sputum for culture and sensitivity should be
sent immediately
• Quantitative cultures of the lower airways
obtained by blind tracheobronchial aspiration
• Bronchoscopically guided sampling
(bronchoalveolar lavage), or protected
specimen brush allow more targeted antibiotic
therapy.
67.
PNEUMONIA AND ATELECTASIS
PREVENTIONAND TREATMENT
• Stop smoking for at least 1 week before surgery
• Treatment-COPD,asthma, and CHF - optimized.
• Pain control & proper pulmonary hygiene - post op.
• IPPV and chest physiotherapy
• Ventilator pt -semirecumbent position, oral hygiene.
• Chlorhexidine rinse or nasal gel,ET care, elimination
of secretions around the ET cuff, frequent suctioning
with a closed suction
• While awaiting culture results- emperical antibiotic
therapy
68.
ASPIRATION PNEUMONITIS AND
ASPIRATIONPNEUMONIA
• Aspiration of oropharyngeal or gastric contents
into the respiratory tract is a serious
complication of surgery.
• Aspiration pneumonitis(Mendelson syndrome)
is acute lung injury that results from the
inhalation of regurgitated gastric contents,
whereas aspiration pneumonia results from
the inhalation of oropharyngeal secretions that
are colonized by pathogenic bacteria.
69.
ASPIRATION PNEUMONITIS AND
ASPIRATIONPNEUMONIA
PREDISPOSING FACTORS
• Impairment of the esophageal sphincters (upper and lower) and
laryngeal reflexes, altered GI motility
• Absence of preoperative fasting.
• Urgent surgery
• Altered levels of consciousness,
• GI and airway problems
• Cerebrovascular accidents -neurologic dysphagia and dysfunction of
the gastroesophageal junction.
• Anesthetic drugs reduce esophageal sphincter tone
• Patients with NG tubes or who are debilitated- difficulty in
swallowing and clearing airway.
70.
ASPIRATION PNEUMONITIS AND
ASPIRATIONPNEUMONIA
• Pathophysiology of aspiration pneumonitis is related to
pulmonary intake of gastric contents at a low pH
associated with particulate matter.
• The severity of lung injury increases as the volume of
aspirate increases and its pH decreases.
• Often progresses rapidly, may require intubation soon
after the injury occurs, and later sets the stage for
bacterial infection.
• The pathophysiology of aspiration pneumonia is
related to bacteria gaining access to the lungs.
71.
ASPIRATION PNEUMONITIS AND
ASPIRATIONPNEUMONIA
PRESENTATION AND DIAGNOSIS
• Associated vomiting
• May have received general anesthesia or had a NG tube
placed.
• Altered levels of consciousness.
• Initially- wheezing and labored respiration.
• Silent aspiration suggested by an infiltrate on a chest
radiograph or decreased PaO2.
• Other patients have cough, shortness of breath, and wheezing
that progress to pulmonary edema and ARDS.
• CXR- infiltrate in the posterior segments of the upper lobes
and the apical segments of the lower lobes.
72.
ASPIRATION PNEUMONITIS AND
ASPIRATIONPNEUMONIA
• TREATMENT
– Reduce gastric contents, minimize regurgitation, and
protect the airway.
– Preoperative fasting
– Difficult airway -Awake fiber optic intubation
– In emergency situations -preoxygenation is
accomplished without lung inflation, and intubation is
performed after applying cricoid pressure during rapid-
sequence induction.
– Postoperatively- avoid the overuse of narcotics,
encourage the patient to ambulate, and feed cautiously
73.
ASPIRATION PNEUMONITIS AND
ASPIRATIONPNEUMONIA
TREATMENT(cont)
• O2 ,Urgent CXR-bilateral, fluffy infiltrates.
• Oxygen saturation -face mask without excessively high work of
breathing, intubation may not be required.
• Patient’s oxygenation deteriorates and the work of breathing
increases-Increased RR Prompt intubation
• After intubation for suspected aspiration, suctioning the
bronchopulmonary tree confirms the diagnosis and removes
any particulate matter.
• Empirical antibiotics -aspiration pneumonitis that does not
resolve or improve within 48 hours of aspiration.
• Corticosteroid administration XXXXX
• Gram-negative cover-aspiration pneumonia.
74.
PULMONARY EDEMA, ACUTELUNG INJURY,
AND ADULT RESPIRATORY DISTRESS
SYNDROME
• Three of the most common manifestations of acute
respiratory failure are pulmonary edema, acute lung injury,
and ARDS.
• Pulmonary edema -accumulation of fluid in the alveoli-
oxygenation cannot take place-hypoxemia occurs.
– Increased work of breathing
– Increased respiratory rate
– Exaggerated use of muscles of respiration
• Acute lung injury and ARDS are associated with hypo-
oxygenation because of a pathophysiologic inflammatory
response-leads to the accumulation of fluid in the alveoli
as well as thickening in the space between the capillaries
and the alveoli.
75.
PULMONARY EDEMA, ACUTELUNG INJURY,
AND ADULT RESPIRATORY DISTRESS
SYNDROME
• Acute lung injury
– Pao2/fraction of inspired oxygen (FIO2) ratio of
less than 300
– Bilateral infiltrates on chest radiograph
– PCWP less than 18 mm hg
• ARDS
– Pao2/FIO2 ratio of less than 200
– bilateral infiltrates
– PCWP less than 18 mm hg.
PE,ALI,ARDS
PRESENTATION AND MANAGEMENT
•Frankly abnormal chest radiograph-invasive -
Swan-Ganz catheter for evaluation of PCWP.
• Elevated PCWP fluid restriction and
aggressive diuresis.
• Administration of oxygen via face mask in mild
cases and intubation in more severe cases is
also clinically indicated
• Diuresis and fluid restriction
78.
PULMONARY EDEMA, ALIAND ARDS
• Tachypnea
• Dyspnea
• Increased work of breathing
• Cyanosis is associated with advanced hypoxia and is an
emergency.
• Auscultation-poor breath sounds,crackles and
occasionally with rales.
• Arterial blood gas analysis-low pao2 and high paco2.
• Administration of oxygen alone does not usually result
in improvement of hypoxia.
79.
PULMONARY EDEMA, ACUTELUNG INJURY,
AND ADULT RESPIRATORY DISTRESS
SYNDROME
• MANAGEMENT
– Immediate intubation plus careful administration of fluids
– Strategy involves maintaining the patient on the ventilator
with assisted breathing while the injured lung heals
– Initially placed on FIO2 of 100% and then weaned to 60%
as healing occurs.
– Tidal volume-6 to 8 ml/kg, peak pressure-35 cm H2O.
– Tidal volume is set at 10 to 12 ml/kg of body weight, and
the respiratory rate is chosen to produce a paco2 near 40
mm hg.
– Inspiratory-to-expiratory ratio is set at 1 : 2.
PULMONARY EMBOLISM ANDVENOUS
THROMBOEMBOLISM
• VTE comprises DVT and pulmonary embolism (PE).
• VTE is caused by a perturbation of the homeostatic coagulation
system induced by intimal injury, stasis of blood flow, and a
hypercoagulable state.
• The highest risk of VTE occurs in patients hospitalized for surgery.
• The prevalence of PE in patients with malignancy is 11%.
• Inflammatory bowel disease -5% (DVT) and 3%(PE)
• Major trauma- incidence-DVT exceeds 50%,with fatal emboli
occurring in 0.4% to 2% of cases
• Central venous catheter–related thromboses are more common
with femoral placement.
83.
PULMONARY EMBOLISM ANDVENOUS
THROMBOEMBOLISM
• Most pulmonary emboli originate from an
existing DVT in the legs.
• iliofemoral venous system represents the site
from which most clinically significant
pulmonary emboli arise.
• Rare causes - fat embolus associated with
fractures of long bones and air embolism
PULMONARY EMBOLISM ANDVENOUS
THROMBOEMBOLISM
• PRESENTATION AND DIAGNOSIS
• Approximately 5% to 10% of patients develop a massive PE
that results in hemodynamic instability(hypotension, with
or without shock) and death.
• Establishing the diagnosis of PE-
– Confirmatory tests(helical CT scan or pulmonary angiogram)
– Ancillary tests(venous duplex ultrasound [VUS] and D dimer
assay).
– Helical ct (spiral CT or CT pulmonary angiography)-high
specificity (92%) and sensitivity (86%)
• Pulmonary angiogram- gold standard test-visualizes the
arterial tree directly & detects intravascular filling defects.
– Less used-invasive & requires expertise
86.
PULMONARY EMBOLISM ANDVENOUS
THROMBOEMBOLISM
• ECG-rapid, noninvasive, available bedside test
• Transthoracic echocardiography- hemodynamic
consequences of acute ventricular pressure overload—
– right ventricular dysfunction (hypokinesia and dilation),
– interventricular septal flattening and paradoxical motion,
– elevated tricuspid gradient,
– pulmonary hypertension,
– patent foramen ovale
• Dysfunction of the right ventricle occurs in 30% to 50%
of patients with PE who undergo echocardiography.
87.
PULMONARY EMBOLISM ANDVENOUS
THROMBOEMBOLISM
• Venous CDFI-extremities -indirect test for
diagnosing PE.
• PE patients show findings consistent with DVT
• 80% ofpatients with PE have a DVT on the
venogram.
• D dimer levels are typically elevated in patients
with acute thromboembolism.
• Of the many D dimer tests,(ELISA) is the most
sensitive
88.
PULMONARY EMBOLISM ANDVENOUS
THROMBOEMBOLISM
• Chest radiograph
• ECG
• Arterial blood gas analysis
• D dimer assay
• If leg symptoms are present-VUS
• If leg symptoms are absent-Spiral CT
• If spiral CT negative- clinical suspicion-
Angiogram
POSTOPERATIVE HYPERTENSION
• Therisk of hypertension is related to the type
of surgery performed and the presence of
perioperative hypertension.
• Preoperatively
– Essential hypertension
– Renovascular causes
– vasoactive tumors
• Intraoperatively, fluid overload and
pharmacologic agents may cause
hypertension.
93.
POSTOPERATIVE HYPERTENSION
• Postoperatively
–Pain
– Hypothermia
– Hypoxia
– Fluid overload in the postanesthesia period
– Discontinuation of long-term antihypertensive therapy before
surgery
– Intraabdominal bleeding
– Head trauma
– Clonidine withdrawal syndrome
– Pheochromocytoma crisis.
94.
POSTOPERATIVE HYPERTENSION
• PRESENTATIONAND MANAGEMENT
– Routine pre operative workup
– Diastolic >110 mm Hg-assessed and treated
preoperatively.
– Long-term antihypertensive medications-continue
up to day of surgery.
– Oral clonidine clonidine patch for at least 3
days before surgery.
POSTOPERATIVE HYPERTENSION
• HYPERTENSIVECRISIS
– Severe elevation of blood pressure associated with organ
dysfunction—cerebral and subarachnoid hemorrhage and
stroke, acute cardiac events,renal dysfunction, and bleeding
from the operative wound.
– Carotid endarterectomy, aortic aneurysm surgery, and many
head and neck procedures.
• Diastolic hypertension (>110 mm Hg)-cardiac
complications
• Systolic hypertension (>160 mm Hg)-increased risk for
stroke and death.
97.
POSTOPERATIVE HYPERTENSION
• Medications-Rapidonset of action, Short half-life,
and Few autonomic side effects
– Nitroprusside and nitroglycerin (vasodilators)
– Labetalol and esmolol (beta blockers)
– Enalaprilat (useful for patients taking long-term ACE
inhibitors)
– Nicardipine (calcium channel blocker)
• Acute setting –Do not decrease blood pressure
>25% -avoid ischemic strokes and hypoperfusion
injury to other organs.
98.
PERIOPERATIVE ISCHEMIA ANDINFARCTION
• Approximately 30% of all patients undergoing
a surgical procedure have some degree of CAD
• Operation within 3 months of an infarction -
8% to 15% reinfarction rate; between 3 and 6
months postoperatively-3.5%.
99.
PERIOPERATIVE ISCHEMIA ANDINFARCTION
• Myocardial ischemia and MI result from the
imbalance between myocardial oxygen supply and
demand.
• Primary causes that reduce myocardial perfusion
and oxygen supply
– Coronary artery-thrombus that develops on a disrupted
atherosclerotic plaque
– Dynamic obstruction caused by spasm of an epicardial
coronary artery or diseased blood vessel
– severe narrowing-progressive atherosclerosis.
100.
PERIOPERATIVE ISCHEMIA ANDINFARCTION
• Secondary causes that increase myocardial oxygen
requirements, In the presence of Limited myocardial
perfusion
• Extrinsic cardiac factors that include
– Fever and tachycardia (increased myocardial oxygen demand),
– Hypotension (reduced coronary blood flow)
– Anemia
– Hypoxemia (reduced myocardial oxygen delivery).
• The increased circulating catecholamines associated with
surgical stress further increase myocardial oxygen demand.
101.
PERIOPERATIVE ISCHEMIA ANDINFARCTION
• Presentation and Diagnosis
• Acute coronary syndrome comprises a
constellation of clinical symptoms that are
compatible with myocardial ischemia and
encompasses MI
– ST segment elevation myocardial infarction(STEMI)
and depression (Q wave and non–Q wave)
– Unstable angina/non–ST segment elevation
myocardial infarction (NSTEMI).
102.
PERIOPERATIVE ISCHEMIA ANDINFARCTION
• Risk-greatest in the first 48 hours after surgery
• Chest pain radiating into the jaw and left arm
region—is often not present.
• Shortness of breath
• Increased heart rate
• Hypotension
• Respiratory failure
103.
PERIOPERATIVE ISCHEMIA ANDINFARCTION
• Perioperative-often silent
– Shortness of breath (heart failure, respiratory
failure)
– Increased heart rate (arrhythmias)
– Change in mental status
– Excessive hyperglycemia in patients with diabetes.
• Many perioperative MIs are non–Q wave
NSTEMI.
104.
PERIOPERATIVE ISCHEMIA ANDINFARCTION
• Periprocedural MI is associated with the release of
biomarkers of necrosis,
• MB isoenzymes of
– Creatine kinase (CK-MB)
– Troponins
• T (TnT),
• I (TnI),
• C (TnC).
• TnT and TnI are derived from heart-specific genes-
cardiac troponins-not present in healthy individuals
105.
PERIOPERATIVE ISCHEMIA ANDINFARCTION
• Environment with Continuous ECG monitoring and
defibrillator capability.
• Biomarkers of myocardial necrosis-measured.
• CK-MB- less sensitive specific
• Troponins
– detected in blood by 2 to 4 hours
– Elevation-delayed for 8 to 12 hours.
– persist longer, for up to 5 to 14 days.
• Elevated cardiac troponin-above the 99th percentile of
normal in two or more blood samples-at least 6 hours apart
indicate the presence of myocardial necrosis.
PERIOPERATIVE ISCHEMIA AND
INFARCTION
•Perioperative
– beta blockers
– Careful intraoperative monitoring
– Maintenance of perioperative normothermia and
vital signs .
• Continued postoperative pharmacologic
management .
110.
PERIOPERATIVE ISCHEMIA ANDINFARCTION
• Chronic stable angina
– Continue-antianginal medications
– Beta blockers are continued to the time of surgery
and thereafter.
– ECG-before, immediately after, and for 2 days after
surgery.
– Monitored for 48 hours after surgery
– High-risk patients- 5 days
– Cardiac enzyme levels
111.
PERIOPERATIVE ISCHEMIA ANDINFARCTION
• Medical management of myocardial ischemia
and MI
– Immediate administrationof high-flow oxygen
– Transfer to the ICU
– Early consultation with a cardiologist.
• Immediate administration of beta blockers
(oral or IV, dose-titrated to decrease heart rate
to <70 beats/min) and aspirin (160 to 325 mg)
112.
PERIOPERATIVE ISCHEMIA ANDINFARCTION
• Nitroglycerin (given as a continuous IV infusion
after a loading dose) alleviates pain and is
beneficial for patients with MI complicated by
heart failure or pulmonary edema.
• Systemic heparinization
• ACE inhibitors
• Thrombolytic therapy- Contraindicated
• No response to medical therapy-Angiography
113.
CARDIOGENIC SHOCK
• 50%or more of left ventricular muscle mass is
irreversibly damaged reduction in
COhypoperfusion.
• CAUSES
– Ruptured papillary muscle or ventricular wall
– Aortic valvular insufficiency
– Mitral regurgitation,
– Ventricular septal defect.
POSTOPERATIVE CARDIAC ARRHYTHMIAS
•Sinus tachycardia and atrial flutter - most
common types of tachyarrhythmia.
• Sinus tachycardia -caused by pain,fever,
hypovolemia, anemia, and anxiety
• Atrial flutter –electrolyte imbalance, history of
atrial fibrillation, COPD
• Ventricular ectopics-post operative-hypoxia,
acute hypokalemia, and hypercapnia
POSTOPERATIVE CARDIAC ARRHYTHMIAS
TREATMENT
•Control of the ventricular response
• Distinction between arrhythmias that traverse
the atrioventricular node(atrial fibrillation,
ectopic atrial tachycardia) from arrhythmias
that do not (ventricular tachycardia,
fibrillation)
119.
TREATMENT
Cardiology consultation
Monitoring ofpatient on a telemetry floor or in ICU
12-lead ECG and long strip to differentiate between atrial and ventricular arrhythmia
Clinical assessment
• Vital signs
• Peripheral perfusion
• Cardiac ischemia and CHF
• Level of consciousness
TREATMENT OF BRADYARRHYTHMIA
ANDHEART BLOCK
BRADYARRYTHMIA
• Sustained:
Atropine or β-
adrenergic
agonist
• Transient:
No therapy
HEART BLOCK
• Persistent high-grade second-
degree or third-degree block:
Insertion of permanent
pacemaker
122.
POSTOPERATIVE HEART FAILURE
•Clinical syndrome characterized by any structural or
functional cardiac disorder that impairs the ability of the
ventricle to fill with or eject blood.
• CAUSES
– Perioperative MI
– Volume overload
– Hypertension
– Sepsis
– Occult cardiac valvular disease
– PE
– New-onset atrial fibrillation.
123.
POSTOPERATIVE HEART FAILURE
•PRESENTATION
– Shortness of breath
– Wheezing
– Tachycardia
– Narrow pulse pressure
– Low pressure or orthostatic hypotension
– Jugular venous distention
– Peripheral edema
– Rales
– General evidence of poor peripheral perfusion.
URINARY RETENTION
• Inabilityto evacuate a urine-filled bladder- Causes
– MC-reversible abnormality -discoordination of the
trigone and detrusor muscles -increased pain and
postoperative discomfort.
– Perianal operations
– Hernia repair.
– Surgery for low rectal cancer -injury to the nervous
system
– Spinal procedures
– Vigorous IV administration of fluid.
– Benign prostatic hypertrophy
128.
Presentation and Management
•Dull constant discomfort in the hypogastrium.
• Urgency and actual pain -as the retention worsens.
• Percussion just above the pubis – fullness and tenderness.
• Prevention in the population at greatest risk- older adults ,LAR
– Observe, Time since voiding -6-7 hrs
– Adequate management of pain
– Judicious administration of IV fluids
– Awareness of how much time has passed since the last voiding
• . General management
– Initial straight catheterization or placement of a Foley catheter,
– High-risk patients, cystoscopy and cystometry may be required.
129.
Acute Renal Failure/Hospital-acquiredrenal insufficiency
• Sudden reduction in renal output that
results in the systemic accumulation of
nitrogenous wastes.
Major vascular procedures
(ruptured aneurysm)
Patients with advanced
diabetes undergoing
operations,
Major urologic operations,
Renal Transplant
Life-threatening trauma
Major blood loss, Major burn injuries,
Cardiopulmonary bypass
procedures,
Major abdominal cases
associated with septic shock,
Transfusion reactions, Multiorgan system failure
130.
Types- ARF
• Oliguricrenal failure
– urine in which volumes less than 480 mL are seen
in a day.
• Nonoliguric renal failure
– output exceeding 2 liters/day and associated with
large amounts of isosthenuric urine that clears no
toxins from the bloodstream.
132.
ARF-Prevention
– Identification ofpatients with preexisting renal dysfunction;
– Avoid hypovolemia, hypotension, medications dec renal function;
– Judicious use of nephrotoxic drugs.
• Renal impairment- dose adjusted antibiotics -infections
• Contrast nephropathy -adequate hydration , premedication
with a free radical scavenger (e.g., N-acetylcysteine) or the
use of an alternative contrast agent (e.g., gadolinium).
• Renal hypoperfusion –Avoid-optimize CO and vol expn.
• Judicious administration of fluid - history of heart failure.
• Monitoring renal function -creatinine clearance
• Early intervention -postrenal obstruction and abdominal
compartment syndrome
133.
• Anuria thatsuddenly develops postoperatively in an
otherwise healthy individual with no preexisting
renal disease is postrenal in nature until proven
otherwise.
• A kink in the Foley catheter
• obstruction must be cleared
• major pelvic surgery-ligation of the ureters is suspect.
• If renal ultrasound or a CT scan shows hydronephrosis,
immediate surgical treatment is indicated.
134.
• Increase inthe serum creatinine level,
• Decrease in creatinine clearance, and
• Urine output less than 400 mL/day (<20 mL/hr).
• Brown urine in the Foley bag in a trauma patient -
myoglobinuria
– rapid hydration
– diuresis
– alkalinization of the urine
135.
Urine R/E, M/E
–Hyaline casts-hypoperfusion,
– Coarse granular casts - acute tubular necrosis.
– Lipoid casts -NSAIDinduced and contrast-induced
nephropathy
– White and red cell casts -pyelonephritis.
136.
Prerenal vs renalazotemia
– Prerenal azotemia- Concentrating ability of the nephrons
Normal
• normal urine osmolality (>500 mOsm/liter )
• Normal fractional excretion of sodium( FENa <1%).
– Acute tubular necrosis-concentrating ability of the kidney is lost,
• urine osmolality equal to serum (350 mOsm )
• high urine sodium levels ( >50 mg/L,)
– Best laboratory test to discriminate prerenal from renal
azotemia- FENa.
• Prerenal azotemia, FENa is 1% or less,
• Renal azotemia-exceeds 3%.
137.
Prerenal-Hypovolemeia vs cardiac?
•Diuretic vs more fluids
• History
• 1 litre in 20-30 min
• Foley- hourly U/O
• central venous pressure or Swan-Ganz catheter -left-sided
or right-sided heart filling pressure.
• CHF- diuretics, fluid restriction, and appropriate cardiac
medications
• Ultrasound - renal atrophy-chronic metabolic disease.
138.
ARF- Treatment
• Managementof fluid and electrolyte
imbalance
• Monitoring of fluid administration,
• Avoidance of nephrotoxic agents,
• Provision of adequate nutrition,
• Adjustment of doses of renally excreted
medications until recovery of renal function.
139.
Hyperkalemia and fluidoverload - most
urgent
• Hyperkalemia -sodium-potassium exchange resin,
insulin plus glucose, an aerosolized β2-adrenergic
agonist, and calcium gluconate.
• Insulin and β2-adrenergic agonists- shift potassium
intracellularly.
• Less severe hyperkalemia-ion exchange resin
(sodium polystyrene [Kayexalate]) enema
• Refractory hyperkalemia associated with metabolic
acidosis and rhabdomyolysis requires hemodialysis.
140.
• β2-adrenergic agonist
–nebulizer containing 10 to 20 mg in 4 mL of saline over 10
minutes or
– an IV infusion containing 0.5 mg
• Calcium gluconate
– Hyperkalemia-associated cardiac irritability (prolonged P–R
interval or peaked T waves) treated urgently -10% calcium
gluconate solution over 15-minutes and simultaneous IV
administration of insulin and glucose (10-U IV bolus with
50 mL of a 50% dextrose solution, followed by
continuation of glucose to prevent hypoglycemia).
– Calcium gluconate -10 mL of a 10% solution over a 5-
minute- reduce arrhythmias.
141.
• Phosphate levels
–Hypophosphatemia- induce rhabdomyolysis
and respiratory failure
• Treatment- oral administration of Fleet Phospho-
soda.
–Hyperphosphatemia with hypercalcemia-
increases the risk for calciphylaxis
• Treatment-administration of phosphorus binders
(calcium carbonate) or dialysis..
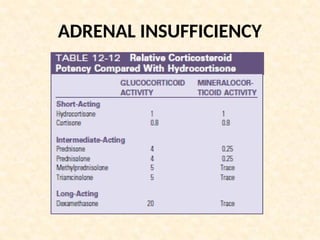
ADRENAL INSUFFICIENCY
• Failureof the adrenal glands to produce
adequate glucocorticoids.
– Primary adrenal insufficiency-
• Addison disease-adrenal cortex-destroyed by cytotoxic
lymphocytes.
– Secondary adrenal insufficiency
• Long-term administration of Glucocorticoids.
Suppression
of
hypothalam
ic-pituitary
Adrena
l
atroph
Adrena
l
insuffici
145.
ADRENAL INSUFFICIENCY
• Acuteadrenal insufficiency
– Abrupt cessation of pharmacologic doses of long-
term glucocorticoid therapy
– Surgical excision or destruction of the adrenal
gland(adrenal hemorrhage, necrosis, or
thrombosis in patients with sepsis or
antiphospholipid syndrome)
– Surgical excision/Destruction (postpartum
necrosis) of the pituitary gland.
ADRENAL INSUFFICIENCY
RAPID ADENOCORTICOTROPICHORMONE STIMULATION TEST
IN PATIENTS WITH ADRENAL ISUFFICIENCY
• Determine baseline serum cortisol level.
• Give IV (or IM) cosyntropin, 250 μg.
• Measure serum cortisol levels 30 to 60 minutes after cosyntropin is given.
• Results
• Normal adrenal function:
• Basal or postcorticotropin plasma cortisol concentration is at least 18
μg/dL or preferably 20 μg/dL.
• Primary adrenal insufficiency
• Cortisol secretion is not increased.
• Severe secondary adrenal insufficiency
• Cortisol levels increase a little or not at all because of adrenocortical
atrophy.
ADRENAL INSUFFICIENCY
TREATMENT
• Stressdose of hydrocortisone (100 mg)-with
induction of anesthesia.
• For minor surgical procedures-maintenance dose
-continued postoperatively.
• For major surgical procedures, stress dose (100
mg) is continued every 8 hours until the patient
is stable or free of complications and then
tapered to the usual maintenance dose.
152.
ADRENAL INSUFFICIENCY
TREATMENT
• Symptomaticpatients are treated with
hydrocortisone or cortisone.
• Fludrocortisone (substitute for aldosterone) is also
administered to patients with primary disease.
• Treatment of functional acute adrenal insufficiency
involves immediate, rapid administration of high-
dose hydrocortisone or methylprednisolone
HYPERTHYROID CRISIS
• Hyperthyroidism-sustainedincrease in the
synthesis of thyroid hormones
• Thyrotoxicosis- clinical syndrome that
results from an abnormal elevation of
circulating levels of thyroid hormone,
regardless of cause.
• Medical emergency
– Thyrotoxic patients with toxic adenoma or toxic
multinodular goitre
– Graves disease.
155.
HYPERTHYROID CRISIS
PRESENTATION ANDDIAGNOSIS
• Precipitated by stressfull event
• Hyperthyroidism
– Nervousness
– Fatigue
– Palpitations
– Heat intolerance
– Weight loss
– Atrial fibrillation (in older patients)
– Ophthalmopathy-eyelid retraction or lag,
periorbital edema, and proptosis
156.
HYPERTHYROID CRISIS
• Suddenonset
• Accentuation of the symptoms and signs of thyrotoxicosis and
organ system dysfunction
– Hyperpyrexia
– Tachycardia
– Out of proportion to fever
– Dehydration
– Collapse
– Central nervous system dysfunction (delirium, psychosis,
seizure, coma)
– Cardiac manifestations
– GI symptoms
– Liver dysfunction.
157.
HYPERTHYROID CRISIS
DIAGNOSIS
• Elevatedlevels of thyroid hormones
• Suppresed levels of TSH
• Thyroid scintigraphy with technetium-99m
pertechnetate or iodine-123 (123I)
–Graves disease-diffuse uptake
–Plummer disease-inhomogeneous pattern
with hot, cold, and warm areas
–Goetsch disease (toxic solitary nodule)-
intense activity in the area of the nodule,
with suppression of paranodular tissue.
HYPOTHYROIDISM
• ECG
– Bradycardia
–Low voltage
– Prolonged P–R, QRS, and Q–T intervals.
• Primary hypothyroidism
– Serum total T4, free T4, and free T3 levels-low
– TSH level-elevated
• Secondary disease
– TSH level-low
– Free T4 index, and free T3-low.
162.
HYPOTHYROIDISM
TREATMENT
• Replacement hormonetherapy continued
till euthyroid state reached
• Myxedema coma or patients showing
clinical signs of significant hypothyroidism
–Immediately treated with thyroid
hormone
–IV administration of hydrocortisone, to
avoid an addisonian crisis
–IV levothyroxine or T3 may be given until
oral ingestion is possible.
163.
SYNDROME OF INAPPROPRIATE
ANTIDIURETICHORMONE SECRETION
• Most common cause of chronic normovolemic
hyponatremia(serum sodium<135 mmol/liter)
• Remains hyponatremic despite all attempts to correct the
imbalance in the presence of persistent antidiuretic activity
from elevated arginine vasopressin levels.
• Predisposing factors
– Trauma
– Stroke
– Antidiuretic hormone– producing tumors
– Drugs (ACE inhibitors, dopamine, nsaids)
– Pulmonary conditions.
164.
SYNDROME OF INAPPROPRIATE
ANTIDIURETICHORMONE SECRETION
• PRESENTATION
–Anorexia
–Nausea
–Vomiting
–Obtundation
–Lethargy
• With more rapid onset
–seizures, coma, and death can result.
165.
SYNDROME OF INAPPROPRIATE
ANTIDIURETICHORMONE SECRETION
PRESENTATION
• The cardinal criteria of SIADH
–Hyponatremia with hypotonicity of plasma
–Urine osmolality in excess of plasma
osmolality
–Increased renal sodium excretion
–Absence of edema or volume depletion
–Normal renal function.
166.
SYNDROME OF INAPPROPRIATE
ANTIDIURETICHORMONE SECRETION
TREATMENT
• Treatment of the underlying disease process
• Treatment of hyponatremia- removal of excess water
• Fluid restriction is the mainstay of management
• Correction –rate of 0.5 mmol/ liter/hr until the serum
sodium concentration is 125 mg/dL or higher.
• Rapid correction-serious permanent neurologic damage.
• Diuretics
Ileus and EarlyPostoperative Bowel
Obstruction
• Early postoperative bowel obstruction - within 30
days after surgery
– Functional (i.e., ileus), -inhibition of propulsive
bowel activity
• Primary or postoperative ileus- occurs immediately
after surgery in the absence of precipitating factors
and resolves within 2 to 4 days
• Secondary, adynamic, or paralytic ileus- result of a
precipitating factor and associated with a delay in
return of bowel
– Mechanical (Partial or complete, high or low,
closed vs open loop)
• luminal, mural, or extraintestinal barrier
169.
• Surgical stressand manipulation of the bowel result in
sustained inhibitory sympathetic activity results in
suppression of the neuromuscular apparatus.
• Opiates and opioid peptides in the enteric nervous
system suppress neuronal excitability.
• After resection and reanastomosis of the small bowel,
the distal part of the bowel does not react to the
pacemaker and the frequency of contractions decreases.
Normal return ofbowel activity
• Small bowel motility - within several hours
• Gastric motility- within 24 to 48 hours
• Colonic motility-within 48 to 72 hours.
• Bowel sounds, flatus, and bowel movements.
• Gastric dilation and vomiting
173.
Presentation
• Cause, degreeand
• Stasis and progressive accumulation of gastric
and intestinal secretions and gas-bowel loses
its tone and dilate- abdominal distention,
pain, nausea and vomiting, and obstipation
174.
Adynamic Vs Mechanical
•Adynamic ileus
– diffuse discomfort but no sharp colicky pain
– distended abdomen.
– quiet abdomen, with few bowel sounds
• Mechanical obstruction
– high-pitched, tinkling sounds
– Fever, tachycardia,
– +/- manifestations of hypovolemia, and sepsis
175.
• In adynamicileus, abdominal radiographs reveal
diffusely dilated bowel throughout the intestinal
tract, with air in the colon and rectum.
• With mechanical bowel obstruction, there is
small bowel dilation with air-fluid levels and
thickened valvulae conniventes in the bowel
proximal to the point of obstruction and little or
no gas in the bowel distal to the obstruction
176.
• Measures toprevent ileus intraop
– Handle the tissues gently
– limit peritoneal dissection to only what is
essential.
– The bowel must not be allowed to desiccate by
prolonged exposure to air without protection
– Anti-adhesion barriers- an oxidized cellulose
product and a product that is a combination of
sodium hyaluronate and carboxymethyl cellulose.
• Three stepapproach for post op ileus
resuscitation
investigation
surgical intervention.
• Emergency relaparotomy is performed if there is a
closed loop, high-grade, or complicated small bowel
obstruction, intussusception, or peritonitis.
• Adynamic ileus and partial mechanical-waiting
expectantly for resolution(7-14 d)
179.
Acute Abdominal CompartmentSyndrome
• Abdominal compartment syndrome (ACS) describes increasing
organ dysfunction or failure as a result of IAH.
• IAH
– consistent increased IAP value higher than 12 mm Hg
– minimum of 3 measurements 4 to 6 hours apart,
– measured at the end of expiration
• ACS
– IAP -20 mm Hg or greater,
– abdominal perfusion pressure < 50 mm Hg (at least 3 measurements
performed 1 to 3 hours apart)
– (abdominal perfusion pressure = mean arterial pressure − IAP)
– associated with failure of one or more organ systems
180.
• Primary ACSdevelops as a result of pathologic IAH caused
by intra-abdominal pathology and
• Secondary ACS develops in the absence of intra-
abdominal primary pathology, injury.
• Primary ACS is most commonly encountered in victims of
multiple trauma and after damage control surgery due to
bowel edema and contamination, continued bleeding,
coagulopathy, packing used to control bleeding, capillary
leak, and massive fluid resuscitation and transfusion.
181.
• In nontraumapatients, IAH and possibly primary ACS
have been reported to occur in patients with
– Ascites
– Retroperitoneal hemorrhage
– Pancreatitis
– Pneumoperitoneum
– After reduction of chronic hernias
– Repair of ruptured abdominal aortic aneurysm,
– Complex abdominal procedures, and liver
transplantation
182.
• Secondary ACSis in part iatrogenic and
commonly encountered in patients with
–shock requiring aggressive fluid
resuscitation with crystalloids
–Thermally injured and shock trauma victims
–Critically ill hypothermic
–septic patients
–Sustained cardiac arrest
183.
Diagnosing ACS
• Respiratorydifficulty, Oliguria ,high filling pressures
and vasopressor therapy is required. The abdomen
becomes distended and tense, and neurologic
deterioration may occur.
• Use of the urinary bladder catheter -gold std-
indirectly IAP.
– GI (IAP <10 to 15 cm H2O),
– GII (IAP <16 to 25 cm H2O)
– GIII (IAP <26 to 35 cm H2O)
– GIV (IAP >36 cm H2O).
184.
• The preventionof primary ACS -by leaving the
peritoneal cavity open in patients at risk for IAH and
after high-risk surgical procedures.
• Patients at risk for secondary ACS receiving crystalloid
resuscitation must be monitored closely.
• The decision surgical intervention is not based on IAH
alone but rather on the presence of organ dysfunction
in association with IAH.
185.
• Decompression leadsto reduction of IAH,
severe hypotension and abrupt increase in the
true tidal volume delivered to the patient,
with washout of the byproducts of anaerobic
metabolism
• This results in respiratory alkalosis
186.
• Decrease ineffective preload
• Hence, decompression is performed after
adequate preload with volume has been
established.
188.
Postoperative Gastrointestinal Bleeding
•Possible sources in the stomach include peptic
ulcer disease, stress erosion, a Mallory-Weiss
tear, and gastric varices
• In the small intestine, arteriovenous
malformations and bleeding from an
anastomosis
• In the large intestine, anastomotic hemorrhage,
diverticulosis, arteriovenous malformations
189.
Risk Factors forDevelopment of Stress Erosions
• Multiple trauma
• Head injury
• Major burns
• Clotting abnormalities
• Severe sepsis
• Systemic inflammatory response syndrome
• Cardiac bypass
• Intracranial operations
190.
The basic principlesof management of postoperative GI bleeding
1. Fluid resuscitation and restoration of
intravascular volume
2. Checking and monitoring clotting parameters and
correcting abnormalities, as needed
3. Identification and treatment of aggravating
factors
4. Transfusion of blood products
5. Identification and treatment of the source of the
bleeding
191.
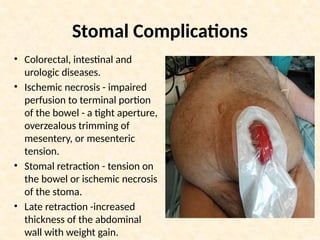
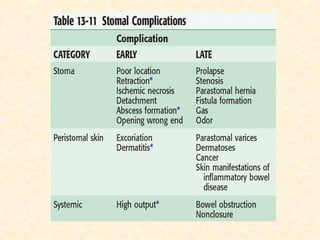
Stomal Complications
• Colorectal,intestinal and
urologic diseases.
• Ischemic necrosis - impaired
perfusion to terminal portion
of the bowel - a tight aperture,
overzealous trimming of
mesentery, or mesenteric
tension.
• Stomal retraction - tension on
the bowel or ischemic necrosis
of the stoma.
• Late retraction -increased
thickness of the abdominal
wall with weight gain.
193.
• Stomal prolapsecan result in incomplete
diversion of stool, interfere with the stoma
appliance, lead to leakage of stool
• A peristomal fistula is often a sign of Crohn’s
disease
• Pyoderma gangrenosa may develop in patients
with inflammatory bowel disease
• Parastomal varices may develop in patients with
liver disease.
Clostridium difficile Colitis
•It is an inflammatory bowel disease caused by
toxins produced by unopposed proliferation of
C. difficile
• cephalosporins, clindamycin, and ampicillin-
amoxicillin were most commonly associated
with CDI
197.
• Presents withwatery diarrhea
• The stools are foul-smelling and may be
positive for the presence of occult blood
• In severe colitis, the diarrhea becomes
associated with abdominal cramps and
anorexia, abdominal tenderness, dehydration,
tachycardia, a raised leukocyte count
198.
• Pseudomembranous colitisis the more dramatic
form of the disease and develops in 40% of patients
• Antibiotic of choice is metronidazole
• Colectomy is indicated when medical treatment
fails or when the patient develops hemodynamic
instability, fulminant disease, toxic megacolon, or
peritonitis.
199.
Anastomotic leak
• Itis leakage of intestinal contents after resection and
anastomosis
• The level of the anastomosis in the GI tract is
important.
• Small bowel, ileocolic, and ileorectal anastomoses are
considered safe
• Esophageal, pancreaticoenteric, and colorectal
anastomoses are considered high risk for leakage.
• In the esophagus, lack of serosa appears to be a
significant contributing factor.
200.
• In therectum, the highest leak rate is found in
anastomoses in the distal rectum, 6 to 8 cm from
the anal verge.
• Adequate microcirculation at the resection margins
is crucial for the healing of any anastomosis.
• Intraluminal distention is believed to be
responsible for rupture of an anastomosis.
201.
Construction of ananastomosis that is at low risk for disruption
• Adequate exposure, gentle handling of tissues,
aseptic precaution,and meticulous, careful
dissection
• Adequate mobilization -tension-free anastomosis
• Correct technical placement of sutures or staples
with little variance
• Matching of the lumens
• Preservation of the blood supply to the ends
202.
• Factors interferingwith the perianastomotic
microcirculation include
– Smoking
– Hypertension
– locally enhanced coagulation activity as a result
of surgical trauma
– perianastomotic hematoma
– presence of macrovascular disease
–Infection
• The earlywarning signs of anastomotic leak are
malaise, fever, abdominal pain, ileus, localized
erythema around the surgical incision, and
leukocytosis.
• There may be an initial excessive drainage from the
surgical wound or surgical wound dehiscence and/or
evisceration.
• Sepsis is a prominent feature of anastomotic leakage
and results from diffuse peritonitis or localized
abscess
205.
• Once ananastomotic leak is suspected or
diagnosed, resuscitation is started immediately
• Oral intake is stopped and the bowel is put at rest
• Reoperation is indicated if there is diffuse
peritonitis, intraabdominal hemorrhage,
suspected intestinal ischemia, major wound
disruption, or evisceration
206.
Intestinal Fistulas
• Afistula represents an abnormal
communication between two epithelialized
surfaces, one of which is a hollow organ.
• In the GI tract, a fistula may develop between
any two digestive organs or between a hollow
organ and the skin
207.
• They commonlyoccur as the result of
–Anastomotic breakdown
–Crohn’s disease
–Radiation enteritis
–Distal obstruction
–Abscess or peritonitis
208.
• Enterocutaneous fistulasare usually
associated with a triad of sepsis, fluid and
electrolyte imbalance, and malnutrition
• Fistula -high or low output on the basis of the
volume of discharge in 24 hours.
– low output (<200 mL/24 hr)
– Moderate output (200 to 500 mL/24 hr),
– High output (>500 mL/24 hr).
209.
• The firststep in the management of a GI fistula is
to prevent its occurrence
• Oral intake is stopped and the bowel is put at rest
• Management involves resuscitation, TPN,
correction of electrolyte imbalances, and
transfusions
HEPATOBILIARY COMPLICATIONS
BILE DUCTINJURIES
• Cholecystectomy accounts for most postoperative
biliary injuries and strictures.
• Bile leak may-bile duct injury, cystic duct stump leak,
divided accessory duct, or injury to the intestine.
• Acute cholecystitis, a foreshortened cystic duct,
anomalies of the biliary tree, hemorrhage from injury
to the cystic or hepatic artery, failure to define
anatomy of calot
• The most common injury sustained during the
laparoscopic procedure is complete transection at or
below the hepatic duct bifurcation
213.
HEPATOBILIARY COMPLICATIONS
PRESENTATION ANDDIAGNOSIS
• Bile leakaccumulate in the subhepatic spaceform
biloma or seep into the peritoneal cavitybile ascites
– Right upper quadrant pain
– Fever
– Nausea
– Abdominal distention
– Malaise.
• Bile-intraoperatively placed drain-manifest as a bile
leak
– Leukocytosis
– Slightly elevated bilirubin level.
214.
HEPATOBILIARY COMPLICATIONS
DIAGNOSIS
• Nuclearmedicine imaging-presence of a leak or
obstruction
• CT scan-identify bile collections or ascites
• ERCP-define the type and level of injury accurately.
• Percutaneous transhepatic cholangiography-define
the proximal anatomy and site of injury
• MRCP-testof choice-late strictures and define the
bile duct anatomy
215.
HEPATOBILIARY COMPLICATIONS
TREATMENT- Intraop
•Proper surgical technique and adequate
identification of the anatomy
• The cystic duct and artery to be divided when the
anatomy is clearly delineated.
• Avoid Excessive traction on the gallbladder-tenting
of the common duct.
• Bleeding in the area of the cystic duct-blind clipping
and cautery must avoided
• Intraoperative cholangiography helps identify the
anatomy and any injuries
216.
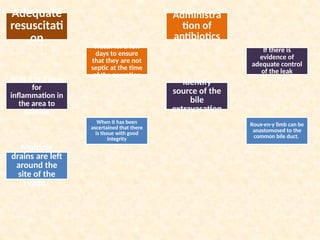
HEPATOBILIARY COMPLICATIONS
• TREATMENT(CONT)
•Intraoperative diagnosis of leak- immediate
repair
A
n
a
c
c
e
s
s
o
r
y
d
u
c
t
l
i
g
a
t
e
d
H
i
g
h
i
n
j
u
r
y
c
a
n
b
e
r
e
p
a
i
r
e
d
w
i
t
h
a
r
o
u
e
x
-
e
n
-
Y
b
i
l
i
a
r
y
e
n
t
e
r
i
c
a
n
a
s
t
o
m
o
s
i
s
Adequate
resuscitati
on
Administra
tion of
antibiotics
Watch fora few
days to ensure
that they are not
septic at the time
of the operation
If there is
evidence of
adequate control
of the leak
Wait 5 to 7 days
for
inflammation in
the area to
subside
Identify
source of the
bile
extravasation
When it has been
ascertained that there
is tissue with good
integrity
Roux-en-y limb can be
anastomosed to the
common bile duct.
Multiple
drains are left
around the
site of the
repair.
DELIRIUM-PRESENTATION AND DIAGNOSIS
–Acutely agitated, uncooperative, and confused.
– Previous psychiatric disorder-withdrawn and
depressed.
– Noncommunicative and emotionally flat
– Withdraw from any emotional exchange.
– Altered level of consciousness
– Changes in cognition.
– Reduced ability to focus
– Decreased levels of awareness
– Difficulty with attention
– Symptoms worsen at night
DELIRIUM, COGNITIVE DISORDER,AND
PSYCHOSIS
DELIRIUM TREMENS
• The most immediately threatening disorder encountered by
physicians
• Occurs 48 hours to 14 days after acute alcohol withdrawal.
• Extreme autonomic hyperactivity
• Fever
• Tremor
• Tachycardia
• Confusion, psychosis, agitation, and seizures.
• Because of the serious underlying nutritional and medical
deficiencies, these patients have moderately high mortality,
225.
DELIRIUM, COGNITIVE DISORDER,AND
PSYCHOSIS
TREATMENT
Treatment of patients with acute confusion or a sudden
change in behavior after surgery requires the following:
1. Recognition of the disorder
2. Close observation and monitoring
3. Identification and elimination of the precipitating factor
4. Treatment of any associated laboratory abnormalities
5. Selective use of imaging or other studies to rule out an
organic brain lesion
6. Application of measures to protect the patient and staff
7. Treatment
226.
DELIRIUM, COGNITIVE DISORDER,
ANDPSYCHOSIS
MEDICAL THERAPY
• Haloperidol, a neuroleptic (0.5 to 2 mg, given iv or im
to achieve a rapid effect and then orally for
maintenance therapy).
• Benzodiazepines are the DOC for acute alcohol
withdrawal.
• Other medications
– Beta blockers (to control autonomic
manifestations)
– Clonidine (to control HTN) are given in addition to
benzodiazepine to patients with acute alcohol
withdrawal.
SEIZURE DISORDERS
MANAGEMENT
• Administrationof IV benzodiazepine- immediate care
• Phenytoin (Dilantin)-most commonly used
anticonvulsant for new-onset generalized or focal
seizures
• Phenobarbital-because of sedation-it is not an agent of
choice.
• Status epilepticus- carbamazepine (Tegretol) and
valproic acid.
• Refractory to other drugs-Gabapentin
230.
SEIZURE DISORDERS
WORK UP
•Detailed history
• Physical examination
• History of previous medication and drug use
• WBC count to rule out occult infection
• Electrolyte and metabolic assessment.
• CT or MRI is indicated-new-onset seizure
activity(Tumours)
• Electroencephalogram-abnormal waveform activity.
231.
STROKE AND TRANSIENTISCHEMIC ATTACKS
Postoperative strokes
Ischemic strokes
1.perioperative hypotension
2.overzealous control of hypertension
3.cardioemboli in patients with atrial
fibrillation.
Hemorrhagic strokes
1.Therapy with anticoagulants
2.Factors related to coagulation disorders,
such as chronic abuse of alcohol, AIDS,
cocaine use, bleeding diathesis
3.preexisting cerebrovascular anomalies
232.
STROKE AND TRANSIENTISCHEMIC ATTACKS
• PRESENTATION AND MANAGEMENT
• A focal alteration in motor function, alteration in mental
status, aphasia, or occasionally unresponsiveness
• Prevention of a perioperative stroke
– Hypertension-adequate treatment
– Overzealous correction-avoided.
– Atrial fibrillation-prophylaxis with anticoagulants.
– High-risk surgical procedure (e.G., Carotid endarterectomy)-
monitored intraoperatively- transcranial doppler and
electroencephalography.
233.
STROKE AND TRANSIENTISCHEMIC ATTACKS
TREATMENT
• IV line placed and be monitored for cardiac arrhythmias.
• Coagulation parameters-presence of a coagulopathy
• Blood culture-bacteremia and bacterial endocarditis.
• CT scan or MRI- distinguish between hemorrhagic and
ischemic stroke
• Hypertensive hemorrhagic stroke-control of the hypertension,
• Embolic stroke-anticoagulation
• Hemorrhagic stroke- reversal of the coagulopathy with
protamine if secondary to heparin or platelet transfusion if
secondary to antiplatelet therapy.
• Mannitol and dexamethasone are given to reduce cerebral
swelling.
234.
STROKE AND TRANSIENTISCHEMIC ATTACKS
• Surgical intervention-localized hematoma or
vascular anomaly
• Thrombolytic therapy (recombinant tissue
plasminogen activator) -restoring cerebral blood
flow and minimizing brain injury-instituted early
after the onset.
• low-dose aspirin therapy-standard-acute ischemic
infarction
• antiplatelet agents (e.g., clopidogrel bisulfate,
ticlopidine hydrochloride) are added in patients
who continue to have symptoms.
#45 Cytokines are low-molecular-weight proteins that act in an autocrine, paracrine, or endocrine fashion to influence a broad range of cellular functions and exhibit proinflammatory and antiinflammatory effects.
#136 History -preexisting renal dysfunction,dehydration
ratio of blood urea nitrogen to creatinine is more than 20. Examination of the patient may reveal distended neck veins, rales in the lungs, and a cardiac gallop—all signs that a failing heart may be underperfusing the kidneys as the cause of the oliguria.
#185 Shock and ischemia
increase capillary permeability; combined with excessive
crystalloid resuscitation (leading to dilution of plasma) and gut
reperfusion, which further increase microvascular permeability,
exudation of fluid with resultant interstitial edema, bowel wall
edema, and ascites occurs.
#186 :(1) using a regular Foley catheter, disconnect from drainage tubing, directly inject 50 mL, clamp, insert needle, and measure;
(2) using a three-way Foley catheter, inject saline into one port, and measure IAP through the other; or
(3) serially connect a regular Foley catheter to a three-way stopcock and a transducer. Other measurement kits are commercially available.
#187 IAP ranges from subatmospheric to
5 mm Hg and fluctuates with respiration, body mass index, and
activity. IAP ranges from 3 to 15 mm Hg after uncomplicated
abdominal surgery. IAP reflects intra-abdominal volume and
abdominal wall compliance. With increased volume, there is a
decrease in compliance, and any further change in volume results
in an increase in pressure, leading to IAH.
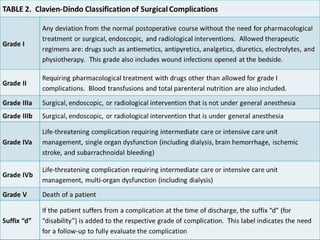
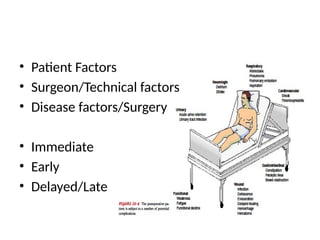
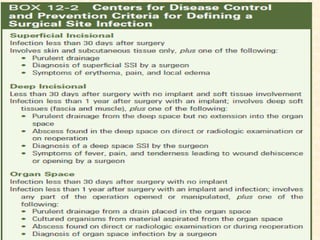
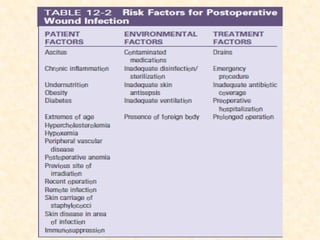
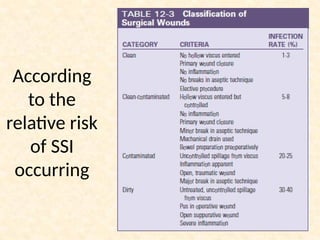

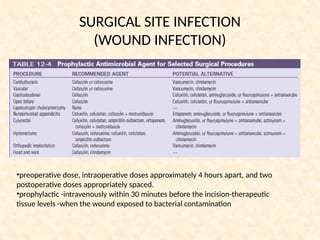
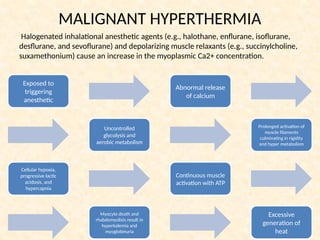

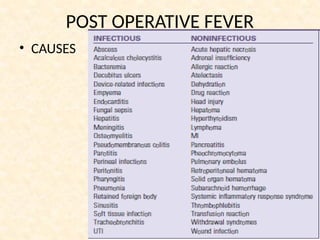
![POST OPERATIVE FEVER-CR-BSI
• The use of central venous catheters
• Microorganisms that colonize t he hubs or from
contamination of the injection site of the CVC(intraluminal
source) or skin (extraluminal source).
• Coagulase- staphylococci, hospital acquired bacteria (e.g.,
MRSA, multidrug-resistant gram-bacilli, fungal species
[Candida albicans]) –mc organisms .
• Metastatic infections (endocarditis)-rre but serious
complication
• Risk factors -duration of CVC, patient location (outpatient
versus inpatient), type of catheter, number of lumens and
manipulations daily, emergent placement, need for TPN,
presence of unnecessary connectors.](https://image.slidesharecdn.com/postopcomplications-250817130616-7d37d76f/85/Post-Op-complications-in-general-surgery-48-320.jpg)

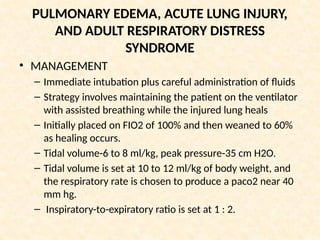
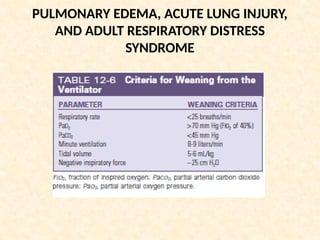
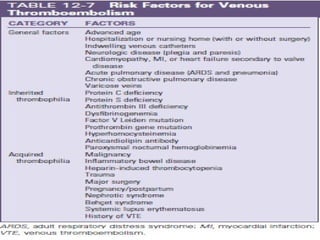
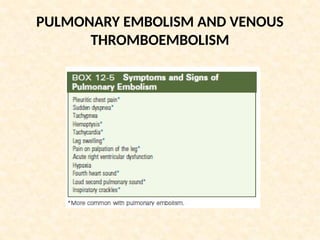
![PULMONARY EMBOLISM AND VENOUS
THROMBOEMBOLISM
• PRESENTATION AND DIAGNOSIS
• Approximately 5% to 10% of patients develop a massive PE
that results in hemodynamic instability(hypotension, with
or without shock) and death.
• Establishing the diagnosis of PE-
– Confirmatory tests(helical CT scan or pulmonary angiogram)
– Ancillary tests(venous duplex ultrasound [VUS] and D dimer
assay).
– Helical ct (spiral CT or CT pulmonary angiography)-high
specificity (92%) and sensitivity (86%)
• Pulmonary angiogram- gold standard test-visualizes the
arterial tree directly & detects intravascular filling defects.
– Less used-invasive & requires expertise](https://image.slidesharecdn.com/postopcomplications-250817130616-7d37d76f/85/Post-Op-complications-in-general-surgery-85-320.jpg)


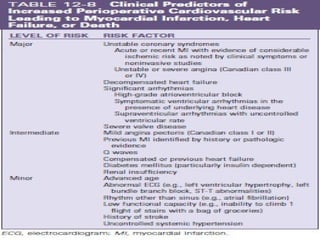
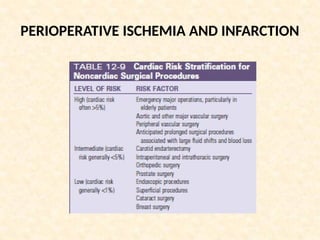
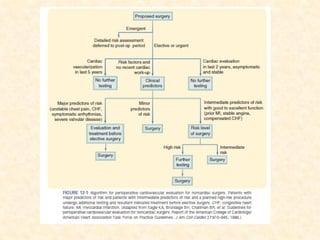

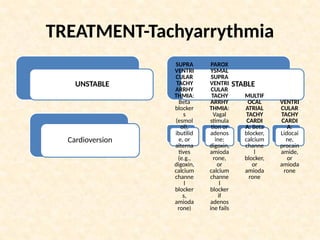
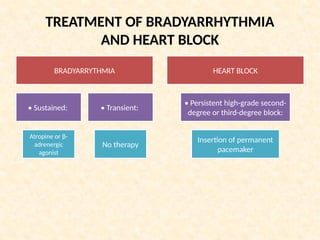
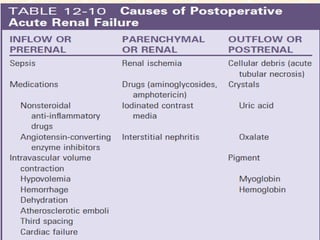
![Hyperkalemia and fluid overload - most
urgent
• Hyperkalemia -sodium-potassium exchange resin,
insulin plus glucose, an aerosolized β2-adrenergic
agonist, and calcium gluconate.
• Insulin and β2-adrenergic agonists- shift potassium
intracellularly.
• Less severe hyperkalemia-ion exchange resin
(sodium polystyrene [Kayexalate]) enema
• Refractory hyperkalemia associated with metabolic
acidosis and rhabdomyolysis requires hemodialysis.](https://image.slidesharecdn.com/postopcomplications-250817130616-7d37d76f/85/Post-Op-complications-in-general-surgery-139-320.jpg)