






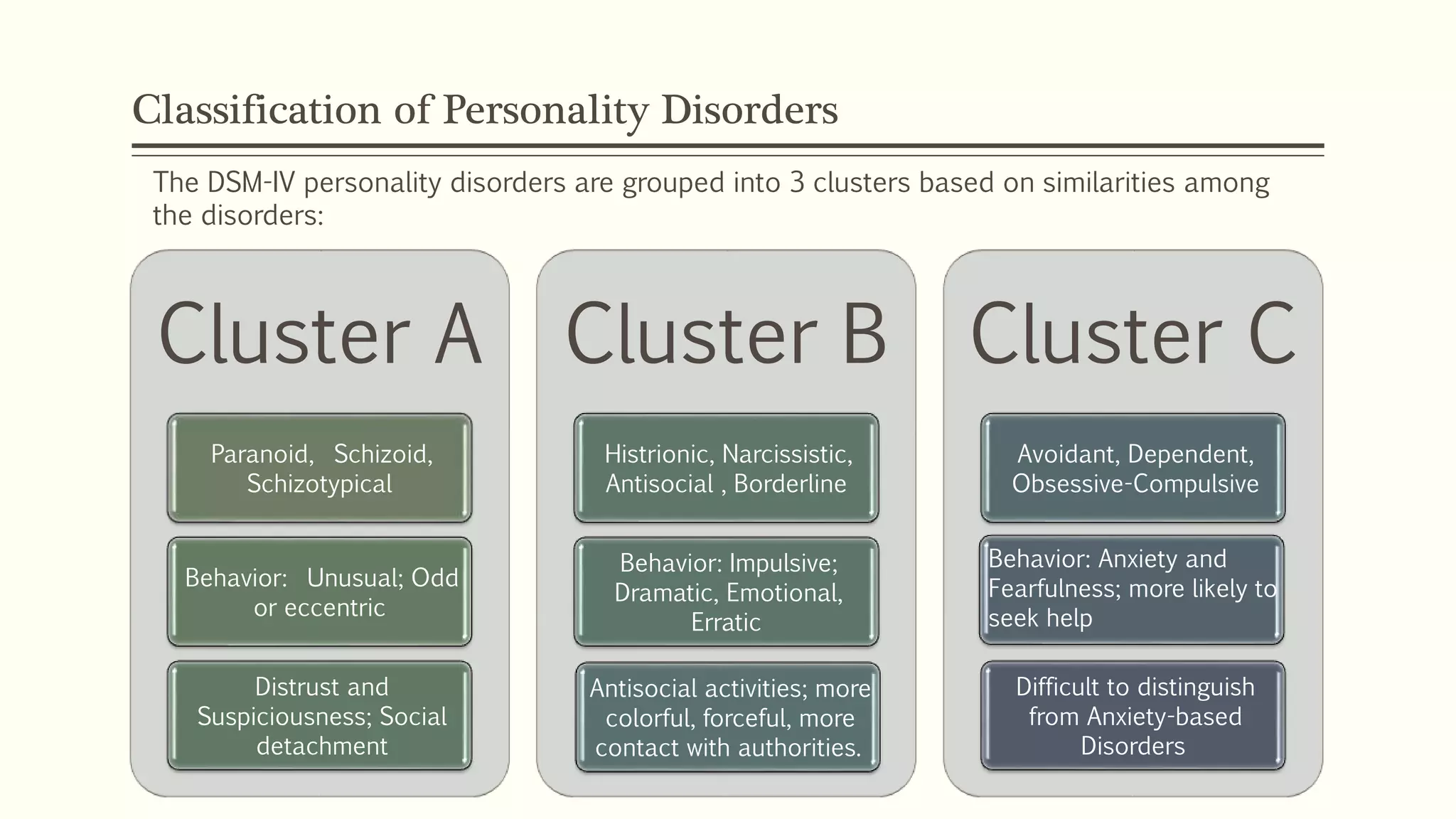
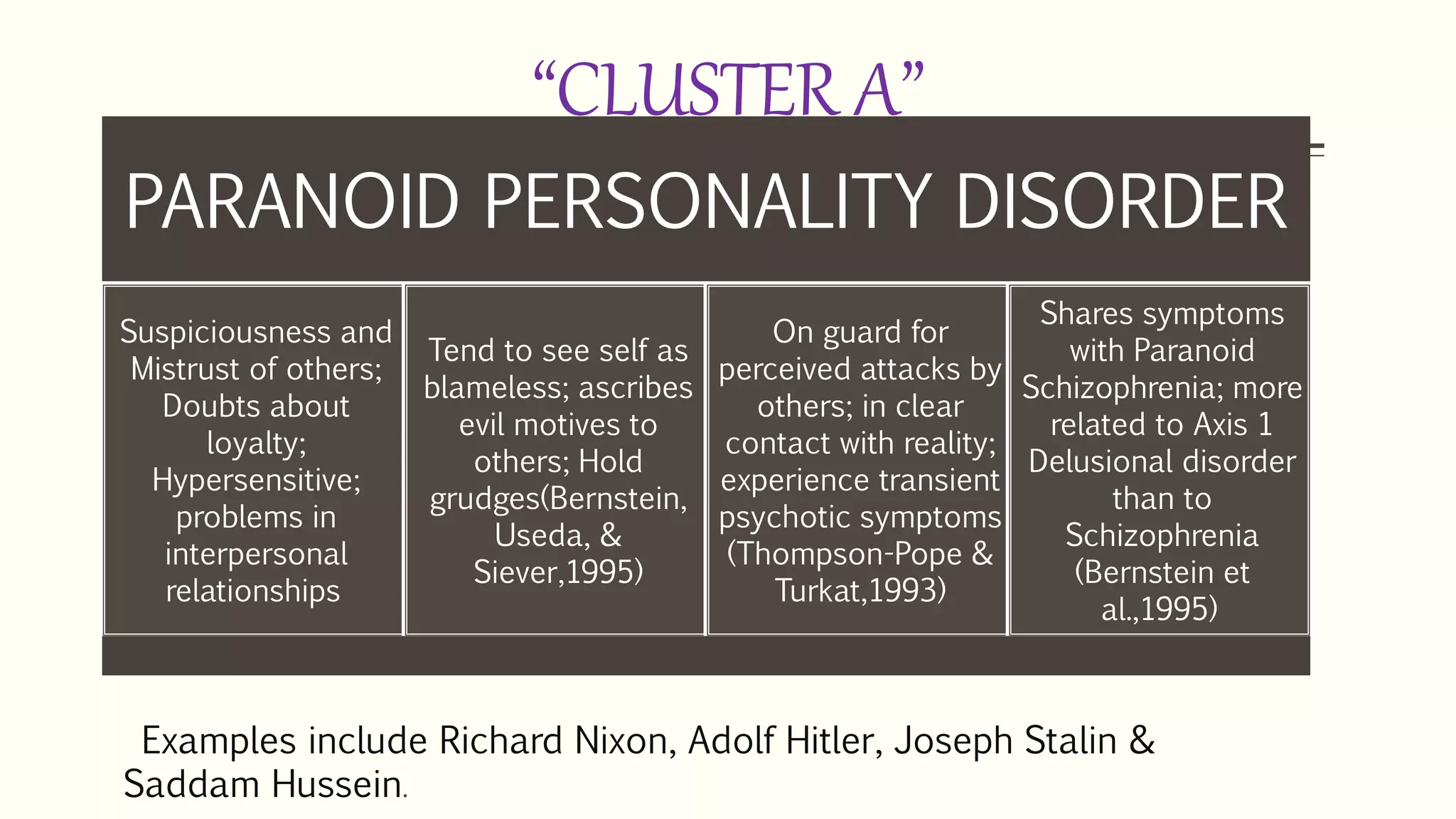









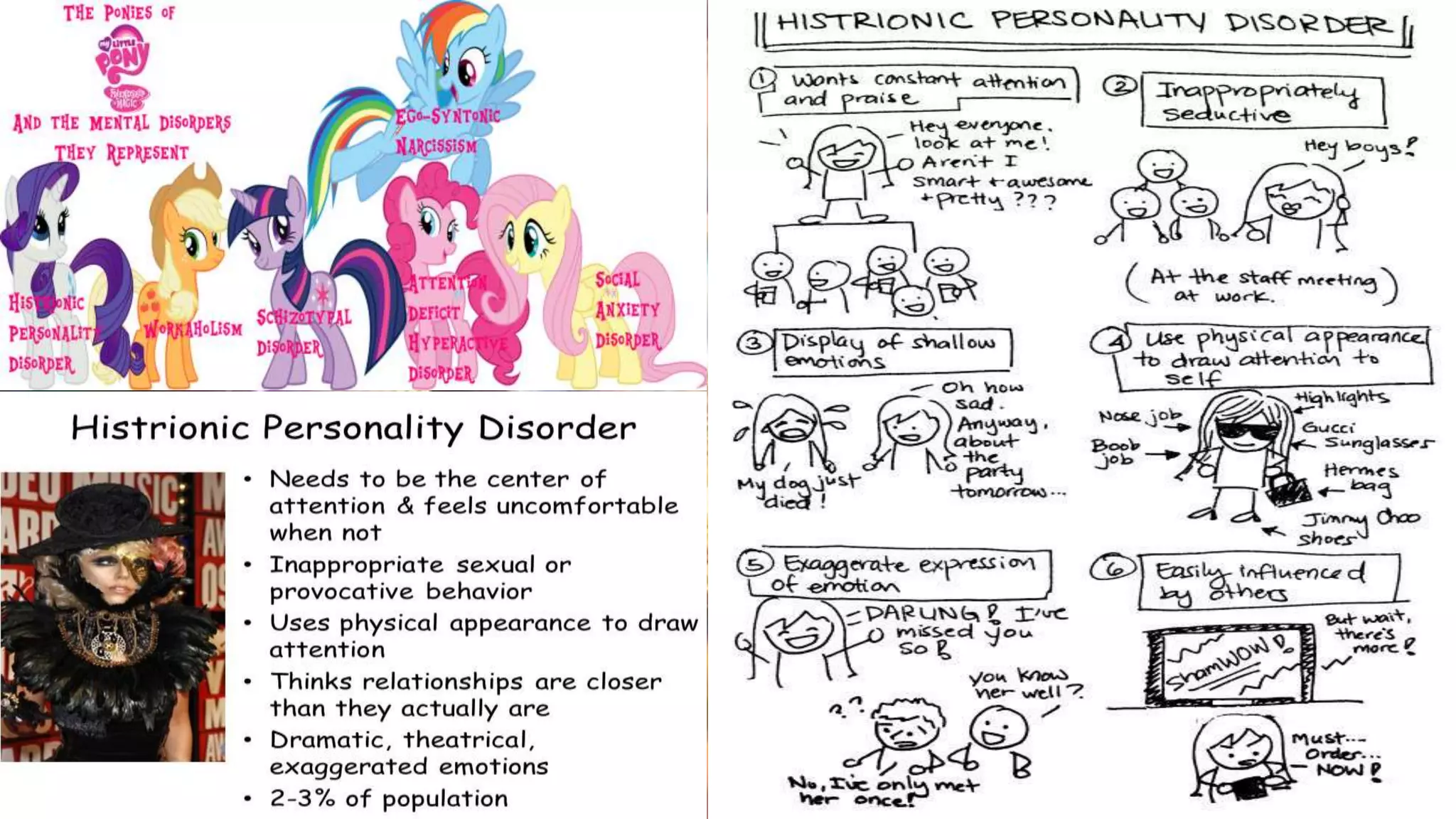








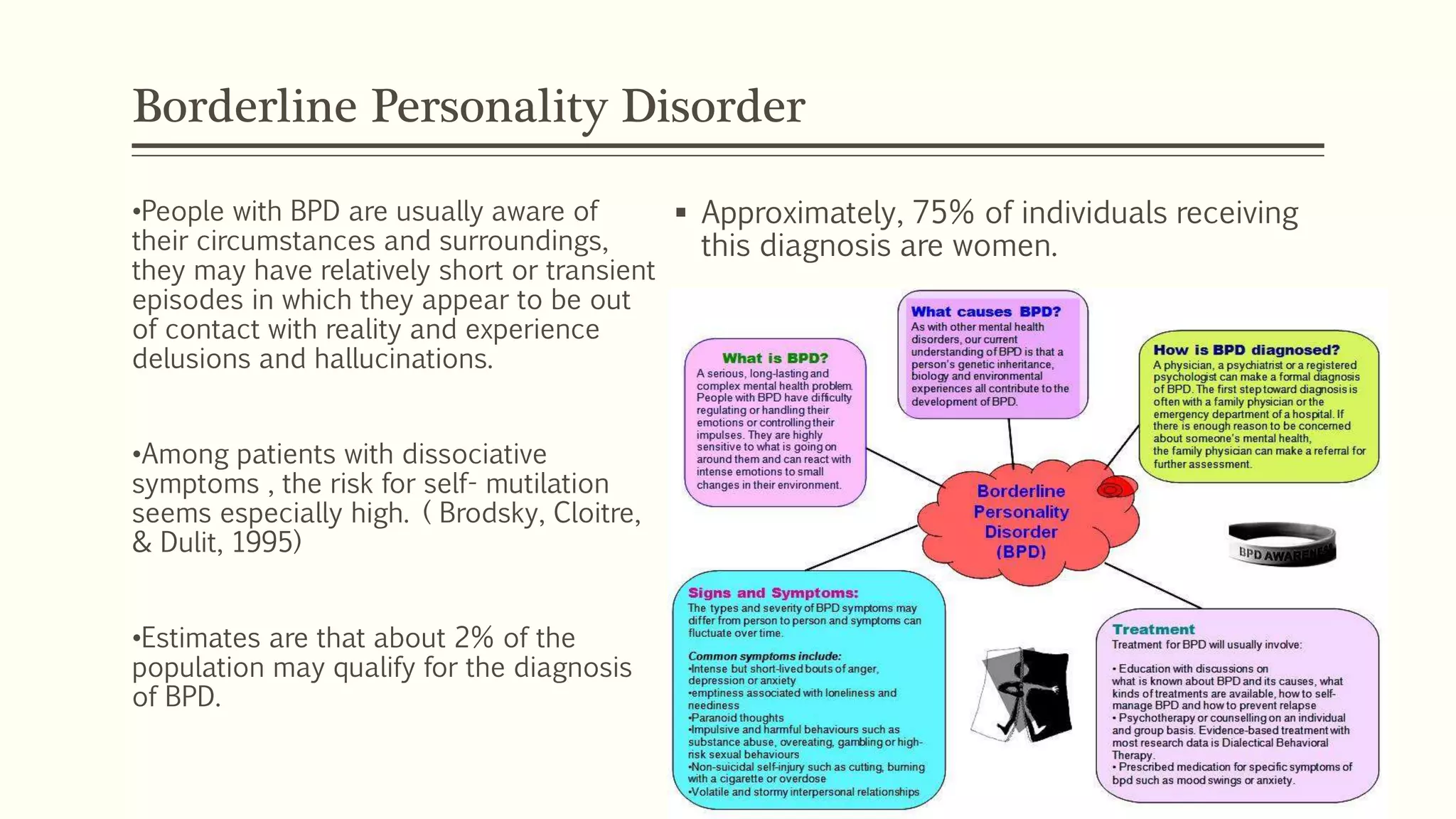













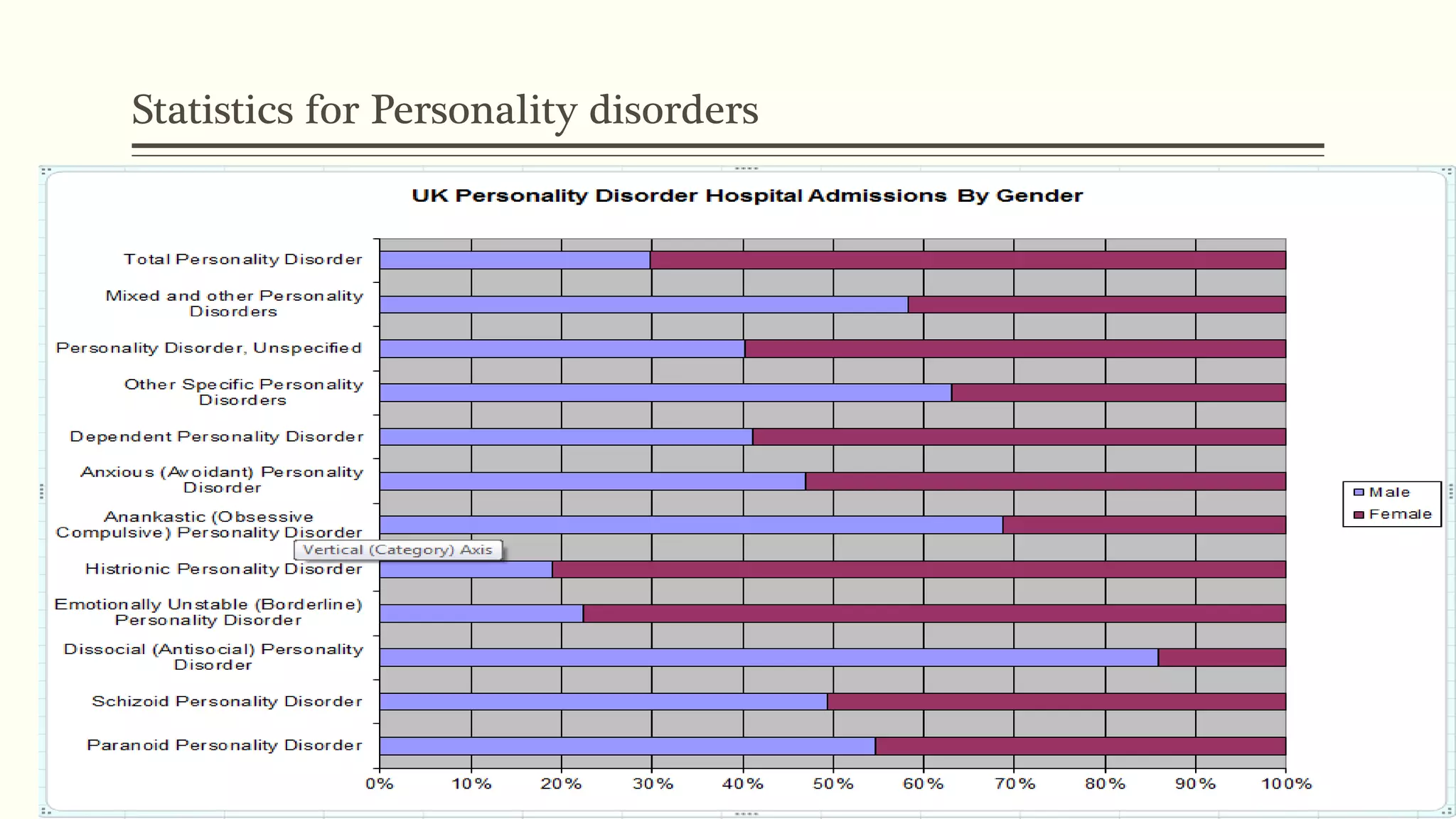


The document provides an extensive overview of personality disorders, detailing their definition, diagnostic criteria according to DSM-IV-TR, and the various classifications into three clusters: A, B, and C, based on traits such as odd behavior, emotional instability, and anxiety. It discusses specific personality disorders within these clusters, highlighting common characteristics, prevalence rates, and relevant examples. Additionally, the text addresses the distinction between personality disorders and traits, emphasizing the impact on functioning and the associated risk factors for co-morbid mental health conditions.















































