The document provides information on personality disorders, including:
1. The definition of a personality disorder as an enduring pattern of inner experience and behavior that deviates from cultural expectations and causes impairment.
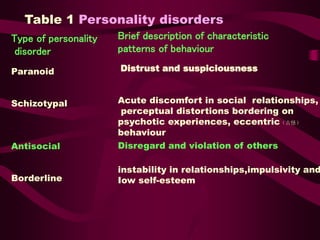
2. The main types of personality disorders are described, including antisocial, borderline, histrionic, narcissistic, avoidant, dependent, and obsessive-compulsive personality disorders.
3. Assessment of personality disorders involves clinical history, standardized measures, and examining areas like childhood experiences, relationships, employment, and criminal history. Treatments evaluated include psychotherapy, cognitive therapies, and intensive programs, but outcomes vary depending on the specific personality disorder.