Appendiceal tumours
Metastatic Colorectal
Cancer
Peritoneal metastatic
disease from GI cancer
Peritoneal
Mesothelioma
Primary Peritoneal
Carcinoma
Rare tumours
3.
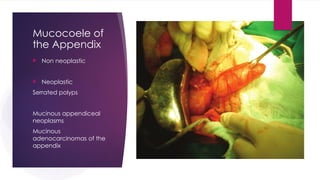
Mucocoele of
the Appendix
Non neoplastic
Neoplastic
Serrated polyps
Mucinous appendiceal
neoplasms
Mucinous
adenocarcinomas of the
appendix
4.
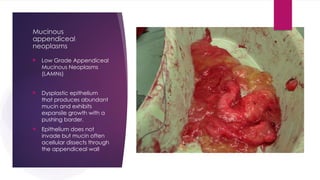
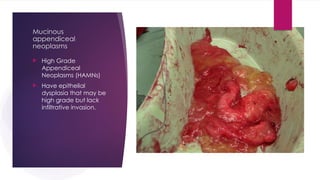
Mucinous
appendiceal
neoplasms
Low GradeAppendiceal
Mucinous Neoplasms
(LAMNs)
Dysplastic epithelium
that produces abundant
mucin and exhibits
expansile growth with a
pushing border.
Epithelium does not
invade but mucin often
acellular dissects through
the appendiceal wall
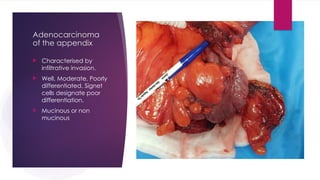
Adenocarcinoma
of the appendix
Characterised by
infiltrative invasion.
Well, Moderate, Poorly
differentiated. Signet
cells designate poor
differentiation.
Mucinous or non
mucinous
8.
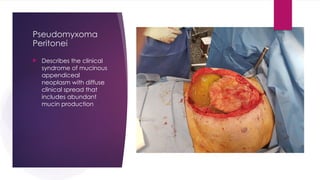
Pseudomyxoma
Peritonei
Describes theclinical
syndrome of mucinous
appendiceal
neoplasm with diffuse
clinical spread that
includes abundant
mucin production
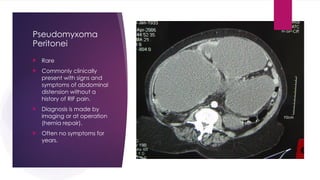
10.
Pseudomyxoma
Peritonei
Rare
Commonlyclinically
present with signs and
symptoms of abdominal
distension without a
history of RIF pain.
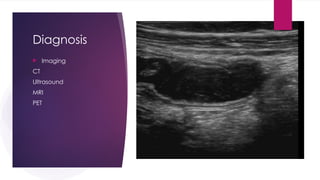
Diagnosis is made by
imaging or at operation
(hernia repair).
Often no symptoms for
years.
STAGING
LAMNs thatare confined to the appendiceal wall without invasion or loss of
the muscularis propria are classified as Tis(LAMN). This is to reflect the
excellent outcome for confined LAMNs. The T1 and T2 stages are not used
for LAMNs. LAMNs that demonstrate involvement with either acellular mucin
or mucinous epithelium of the subserosa or serosa are classified as T3 or
T4a, respectively. Acellular mucin involving the appendiceal serosa or
mesoappendix is classified as T4a, while mucin involvement of distant
peritoneal sites is classified as M1. In order to address the improved
outcome for cases in which peritoneal dissemination is limited to acellular
mucin only, these cases are classified as M1a. Other metastatic categories
are M1b, which refers to metastases confined to the peritoneum only, and
M1c, which refers to metastases outside the peritoneum.
15.
STAGING
In contrastto LAMNs, high-grade appendiceal mucinous neoplasms (HAMNs)
are staged not as in situ tumors but as invasive adenocarcinomas (T1 to T4),
because of their higher risk of recurrence. However, this area is controversial,
and the clinical significance of a diagnosis of HAMN, as opposed to LAMN,
remains unclear.
SURGICAL TREATMENT OF
MUCOCOELEINTACT OR RUPTURED
Appendicectomy with mesoappendix with or without caecectomy.
Ileocolic resection ONLY if this will remove all disease.
Thorough laparoscopy or laparotomy documenting and biopsing sites of
disease within the peritoneal cavity.
DO NOT ATTEMPT TO DEBULK THE PERITONEAL CAVITY.
TUMOUR CELLS LOVE RAW SURFACES
18.
NEXT STAGES
Moststudies show that patients with just acellular mucin deposits on the
visceral peritoneal surface of the appendix (T4a)have a recurrence rate of 3
to 7 percent while for those with cellular mucin(T4M1) outside of the
appendix, the risk is higher and ranges from 33 to 78 percent.
LAMN 7% lymph node metastases at Right Hemicolectomy and no difference
in 5 year survival.
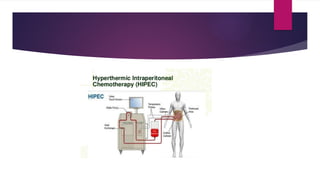
Disseminated mucous or tumour deposits require complete debulking and
Heated Intraperitoneal Chemotherapy (HIPEC)
19.
Preoperative preparation.
Discussionand consent with family
Anaesthetic review
Stomal therapy review
Prehabilitation
Vaccinations in case of splenectomy.
Cessation of anticoagulants
Bowel preparation preop
Preop carbohydrate drinks.
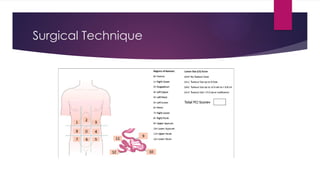
Surgical Technique
RightHemicolectomy with enbloc peritonectomy
Ureteric exposure
Pelvic clearance including stripping bladder and rectum of peritoneum
Left paracolic gutter dissection or Left colectomy (Appendices Epiploica)
Omentectomy
Small bowel clearance
R Diaphragm stripping, Liver capsule excision
L Diaphragm stripping +/- splenectomy
Lesser omentum and stomach
24.
Exclusions to operation
Extensive small bowel disease requiring resection to treat
Disease requiring total gastrectomy
Extensive non resectable porta hepatis disease
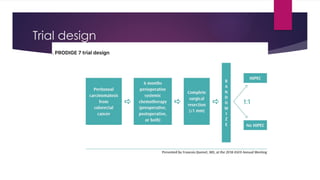
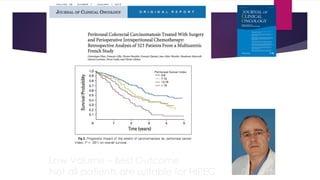
PRODIGE 7 –ACCORD 15
The trial criteria included a 6 month treatment course of perioperative
systemic chemotherapy administered either before or after cytoreductive
surgery (CRS).
CRS was performed in experienced peritoneal malignancy units and
patients were randomized to CRS alone with complete tumour removal or
CRS and HIPEC while in the OR. HIPEC consisted of Oxaliplatin (460 mg/m2)
heated to between 42 and 43 degrees for 30 minutes. 5FU & Folinic acid
were given intravenously over 20mins in HIPEC cases.
37.
The primaryendpoint was the overall survival (OS). (Wanted to increase
from 30% to 48%) Secondary endpoints were relapse-free survival (RFS) and
toxicity. 264 patients were required to show a gain in median OS from 30 to
48 months (HR = 0.625) with a two-sided α = 0,046 and 80% power.
38.
265 patientsfrom 17 centers were included between February 2008 and
January 2014: 132 in Arm without HIPEC and 133 in Arm with HIPEC. The
median age was 60 years (range: 30-74). Baseline characteristics were well
balanced. The overall post-operative mortality rate was 1.5% and was not
different between the two arms. (90% R0) The morbidity rates did not differ
statistically at 30 days. At 60 days, the grade 3-5 morbidity rate was
significantly higher with HIPEC (24.1% vs. 13.6%, p= 0.030).
39.
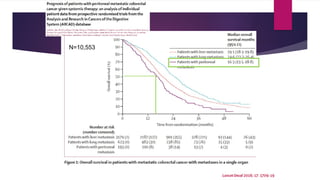
After amedian follow up of 63.8 months (95% CI: 58.9-69.8), the median OS
was 41.2 months (95% CI 35.1-49.7) in the non-HIPEC Arm and 41.7 months
(95% CI: 36.2-52.8) in the HIPEC Arm, HR = 1.00 (95% CI: 0.73-1.37) p = 0.995.
The median RFS was 11.1 months (95% CI: 9-12.7) in non-HIPEC Arm and
13.1 months (95% CI: 12.1-15.7) in HIPEC Arm, HR = 0.90 (95% CI: 0.69-1.90)
(p = 0.486), whilst the 1-year RFS rates were 46.1% in non-HIPEC Arm and 59
% in the HIPEC Arm.
40.
Conclusions: Thetherapeutic curative management of PC from colorectal
cancer by CRS shows satisfactory survival results. While the addition of
HIPEC with oxaliplatin does not influence the OS.
Finding: Statistically improved survival in a subgroup PCI 11-15.
41.
PRODIGE 7
Excellentoutcomes in patients with CPM treated by CRS
(cytoreductive surgery) and intravenous chemotherapy in specialized
peritoneal malignancy units.
The results demonstrate unheralded control of peritoneal metastatic
disease with a median survival of 40 months in both arms attributable to
meticulous surgical technique in combination with systemic
chemotherapy.
Disease free survival 13 & 11 months
42.
PRIMACY OF OPTIMALSURGERY
Despite all advances in chemotherapy, optimal surgery is key to cancer
control and cure for most cases. Patients with CPM deserve to be
assessed, selected and managed by experienced peritoneal malignancy
units where safe judicious use of CRS and HIPEC can optimize outcomes
and minimize complications
Low Volume –Best Outcome
Not all patients are suitable for HIPEC
50.
PIPAC:
Pressurised Intraperitoneal
Aerosol Chemotherapy
Notall patients suitable for HIPEC
Minimally invasive drug delivery system
For Palliative management of Peritoneal Cancer due
to:
Colorectal
Appendiceal
Gastric
Ovarian cancer
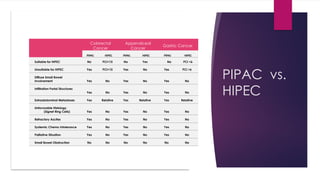
51.
PIPAC vs.
HIPEC
Colorectal
Cancer
Appendiceal
Cancer
Gastric Cancer
PIPACHIPEC PIPAC HIPEC PIPAC HIPEC
Suitable for HIPEC No PCI<15 No Yes No PCI <6
Unsuitable for HIPEC Yes PCI>15 Yes No Yes PCI >6
Diffuse Small Bowel
Involvement Yes No Yes No Yes No
Infiltration Portal Structures
Yes No Yes No Yes No
Extraabdominal Metastases Yes Relative Yes Relative Yes Relative
Unfavorable Histology
(Signet Ring Cells) Yes No Yes No Yes No
Refractory Ascites Yes No Yes No Yes No
Systemic Chemo Intolerance Yes No Yes No Yes No
Palliative Situation Yes No Yes No Yes No
Small Bowel Obstruction No No No No No No
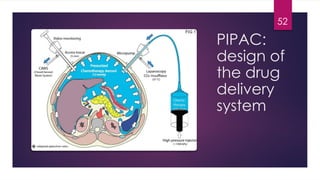
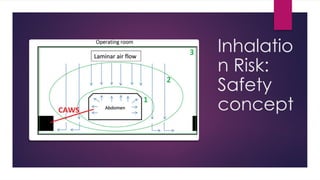
Why Aerosol
Delivery?
Liquids:
Occupythe lower part of a
space corresponding to its
own volume
Do not expand
Flow along a path of least
resistance
An aerosol is a suspension of
liquid droplets within a gas
A gas expands evenly within a
closed space
57.
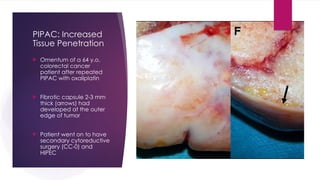
PIPAC: Increased
Tissue Penetration
Omentum of a 64 y.o.
colorectal cancer
patient after repeated
PIPAC with oxaliplatin
Fibrotic capsule 2-3 mm
thick (arrows) had
developed at the outer
edge of tumor
Patient went on to have
secondary cytoreductive
surgery (CC-0) and
HIPEC
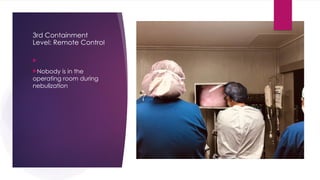
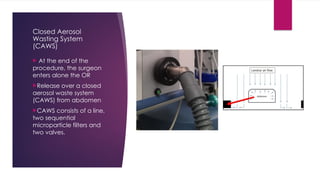
Closed Aerosol
Wasting System
(CAWS)
At the end of the
procedure, the surgeon
enters alone the OR
Release over a closed
aerosol waste system
(CAWS) from abdomen
CAWS consists of a line,
two sequential
microparticle filters and
two valves.
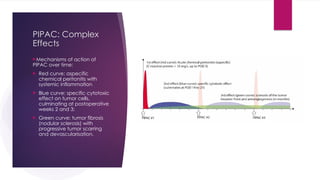
64.
PIPAC: Complex
Effects
Mechanisms ofaction of
PIPAC over time:
Red curve: aspecific
chemical peritonitis with
systemic inflammation
Blue curve: specific cytotoxic
effect on tumor cells,
culminating at postoperative
weeks 2 and 3;
Green curve: tumor fibrosis
(nodular sclerosis) with
progressive tumor scarring
and devascularisation.
65.
PIPAC IN
AUSTRALIA
Theaim of this study is to assess
feasibility, tumour response, occurrence
and severity of adverse events, and
quality of life scores, in determining the
effective palliative nature of PIPAC
therapy in Australian patients with
peritoneal metastases from gastric,
pancreatic, appendiceal and
colorectal primary tumours.
PIPAC IN
AUSTRALIA
Resultsare promising with a statistically
significant overall survival from time of first
PIPAC in patients undergoing 3 or more PIPAC
procedures. Although not statistically
significant, results for PCI scores, ascites and
quality of life show trends suggestive that PIPAC
is beneficial. The absence of any severe
complications (CTCAE Grade 4 or 5) in this study
further supports that PIPAC is a safe and
feasible treatment option.