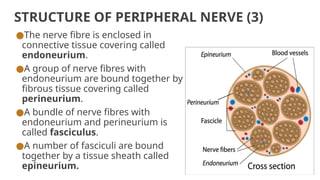
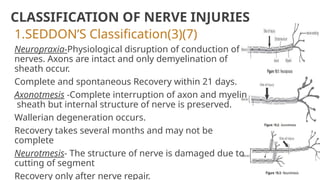
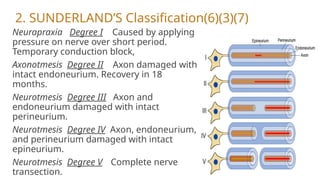
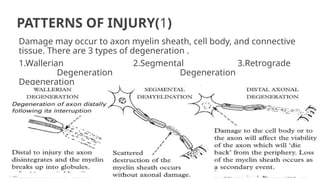
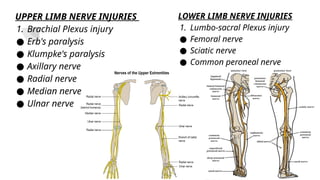
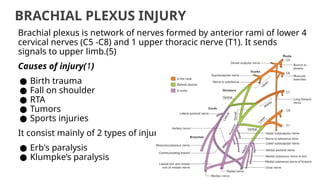
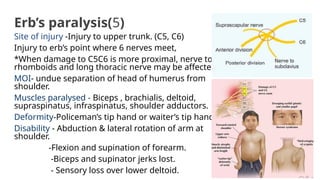
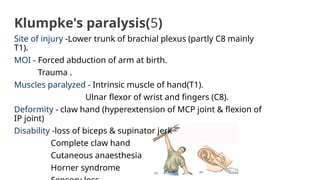
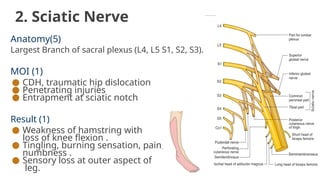
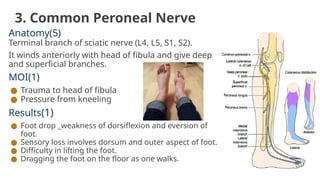
The document discusses peripheral nerve injuries, including their structure, classification, mechanisms, and specific injuries related to the upper and lower limbs. It outlines Seddon's and Sunderland's classifications of nerve injuries, describing various conditions such as neuropraxia, axonotmesis, and neurotmesis, as well as the causes and treatment options for these injuries. Investigations like electromyography and nerve conduction velocity tests are mentioned, along with conservative and operative treatment methods.