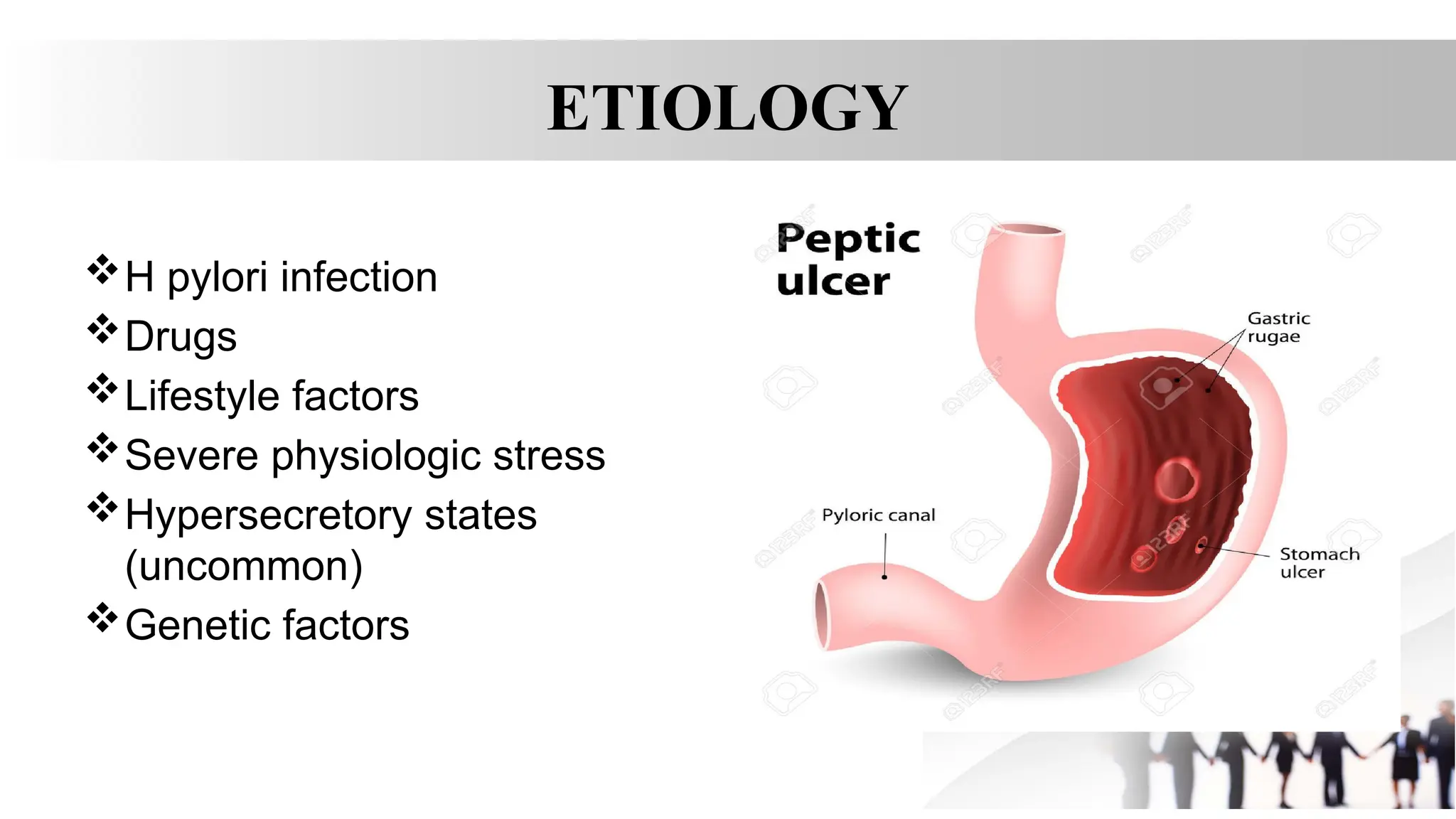
Open soresin the lining of your stomach
or the upper part of the small intestine.
That happens when your stomach acids
etch away your digestive tract’s
protective layer of mucus.
You may have no symptoms, or you
may feel discomfort or burning pain.
Peptic ulcers can lead to internal
bleeding, which sometimes can mean
you’ll need blood transfusions in the
hospital.
• Alarm features" that warrant prompt
gastroenterology referral include
bleeding, anemia, early satiety,
unexplained weight loss, progressive
dysphagia or odynophagia, recurrent
vomiting, and a family history of
gastrointestinal (GI) cancer. Patients with
perforated peptic ulcer disease usually
present with a sudden onset of
severe,sharp abdominal pain.
HYPERSECRETORY STATES
Gastrinoma (Zollinger-Ellisonsyndrome) or
multiple endocrine neoplasia type I (MEN-I)
Antral G cell hyperplasia
Systemic mastocytosis
Basophilic leukemias
Cystic fibrosis
Short bowel syndrome
Hyperparathyroidism
6.
ADDITIONAL
• Cushing ulcersare associated with a brain tumor or injury and typically are single, deep
ulcers that are prone to perforation. They are associated with high gastric acid output and
are located in the duodenum or stomach. Extensive burns are associated with Curling
ulcers.
• Stress ulceration and upper-gastrointestinal (GI) hemorrhage are complications that are
increasingly encountered in critically ill children in the intensive care setting. Severe illness
and a decreased gastric pH are related to an increased risk of gastric ulceration and
hemorrhage.
TYPES
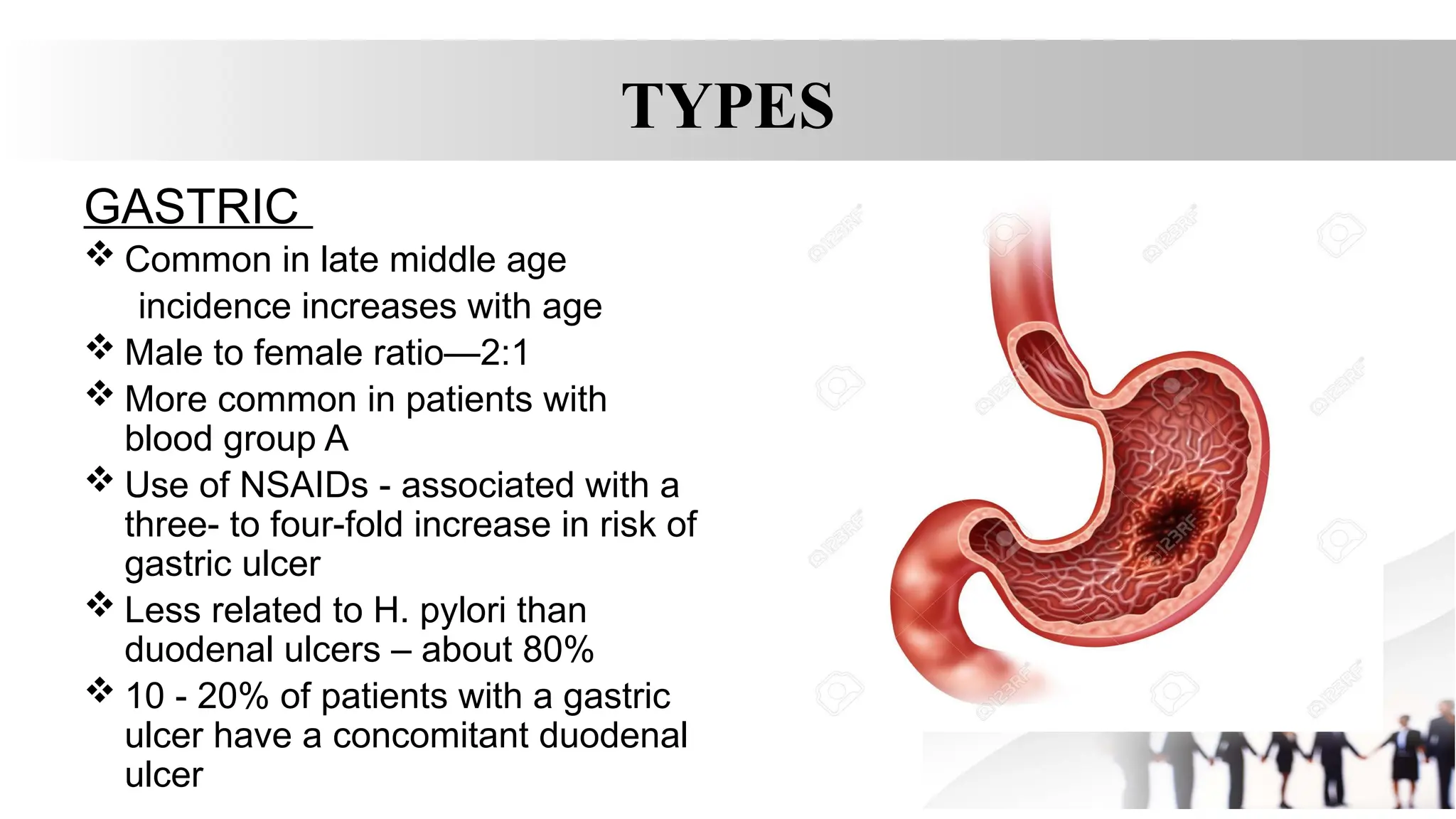
GASTRIC
Common inlate middle age
incidence increases with age
Male to female ratio—2:1
More common in patients with
blood group A
Use of NSAIDs - associated with a
three- to four-fold increase in risk of
gastric ulcer
Less related to H. pylori than
duodenal ulcers – about 80%
10 - 20% of patients with a gastric
ulcer have a concomitant duodenal
ulcer
9.
TYPES
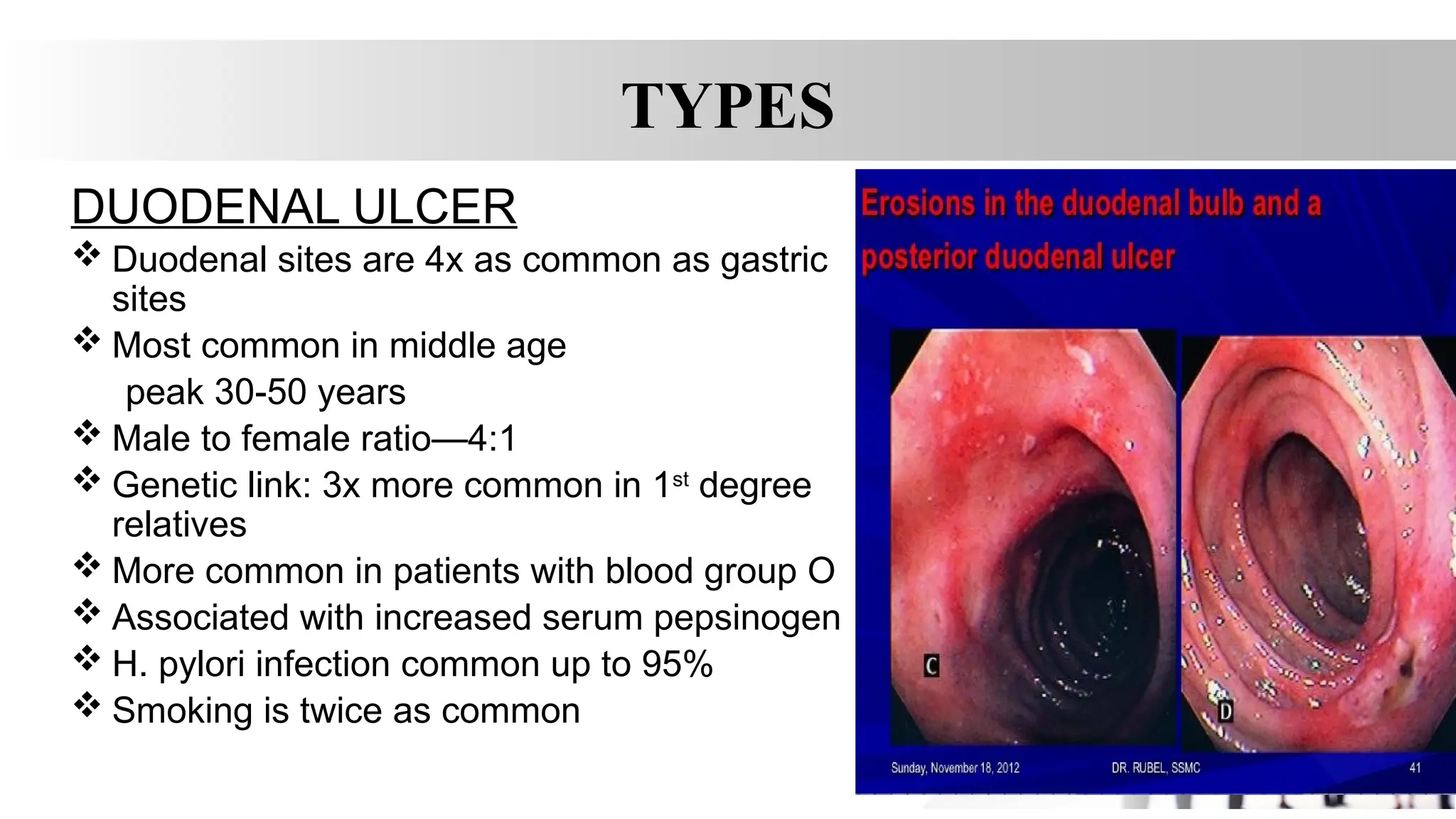
DUODENAL ULCER
Duodenalsites are 4x as common as gastric
sites
Most common in middle age
peak 30-50 years
Male to female ratio—4:1
Genetic link: 3x more common in 1st
degree
relatives
More common in patients with blood group O
Associated with increased serum pepsinogen
H. pylori infection common up to 95%
Smoking is twice as common
12.
PATHOPHYSIOLOGY
• Peptic ulceroccur when the balance between the aggressive
factors and the defensive mechanisms is disrupted.
• Aggressive factors, such as nonsteroidal anti-inflammatory drugs
(NSAIDs), H pylori infection, alcohol, bile salts, acid, and pepsin,
can alter the mucosal defense by allowing back diffusion of
hydrogen ions and subsequent epithelial cell injury.
• The defensive mechanisms include tight intercellular junctions,
mucus, bicarbonate, mucosal blood flow, cellular restitution, and
epithelial renewal.
13.
PATHOPHYSIOLOGY
• In patientsinfected with H pylori, high levels of gastrin and pepsinogen
and reduced levels of somatostatin have been measured.
• In infected patients, exposure of the duodenum to acid is increased.
Virulence factors produced by H pylori, including urease, catalase,
vacuolating cytotoxin, and lipopolysaccharide, are well described.
• Most patients with duodenal ulcers have impaired duodenal
bicarbonate secretion, which has also proven to be caused by H pylori
because its eradication reverses the defect.
• The combination of increased gastric acid secretion and reduced
duodenal bicarbonate secretion lowers the pH in the duodenum, which
promotes the development of gastric metaplasia
14.
SYMPTOMS
• Pain—Gnawing,Aching,Burning.
– Duodenalulcers: occurs 1-3 hours after a meal and may awaken patient
from sleep. Pain is relieved by food, antacids, or vomiting.
– Gastric ulcers: food may exacerbate the pain while vomiting relieves it.
• Nausea, vomiting, belching, dyspepsia, bloating, chest discomfort, anorexia,
hematemesis, &/or melena may also occur.
– nausea, vomiting, & weight loss more common with Gastric ulcers
15.
PHYSICAL EXAMINATION
• Inuncomplicated peptic ulcer disease, the clinical findings are few and nonspecific and include the
following:
• Epigastric tenderness (usually mild)
• Right upper quadrant tenderness may suggest a biliary etiology or, less frequently, peptic ulcer disease
• Melena resulting from acute or subacute gastrointestinal bleeding
16.
PHYSICAL EXAMINATION
• Patientswith perforated peptic ulcer disease usually present with a sudden onset of severe, sharp
abdominal pain. Most patients describe generalized pain; a few present with severe epigastric pain. As
even slight movement can tremendously worsen their pain, these patients assume a fetal position.
Abdominal examination usually discloses generalized tenderness, rebound tenderness, guarding, and
rigidity. However, the degree of peritoneal findings is strongly influenced by a number of factors,
including the size of the perforation, amount of bacterial and gastric contents contaminating the
abdominal cavity, time between perforation and presentation, and spontaneous sealing of perforation.
• These patients may also demonstrate signs and symptoms of septic shock, such as tachycardia,
hypotension, and anuria. Not surprisingly, these indicators of shock may be absent in elderly or
immunocompromised patients or in those with diabetes. Patients should be asked if retching and
vomiting occurred before the onset of pain.
17.
WORK UP
• completeblood cell (CBC) count, liver function tests (LFTs), and levels of
amylase and lipase may be useful. CBC count and iron studies can help
detect anemia, which is an alarm signal that mandates early endoscopy to
rule out other sources of chronic gastrointestinal (GI) blood loss.
18.
• UREA BREATHTEST
• RAPID UREASE TEST
• SERUM ANTIBODY
• CULTURE OF GASTRIC BIOPSY
• STOOL ANTIGEN TEST
19.
ENDOSCOPY
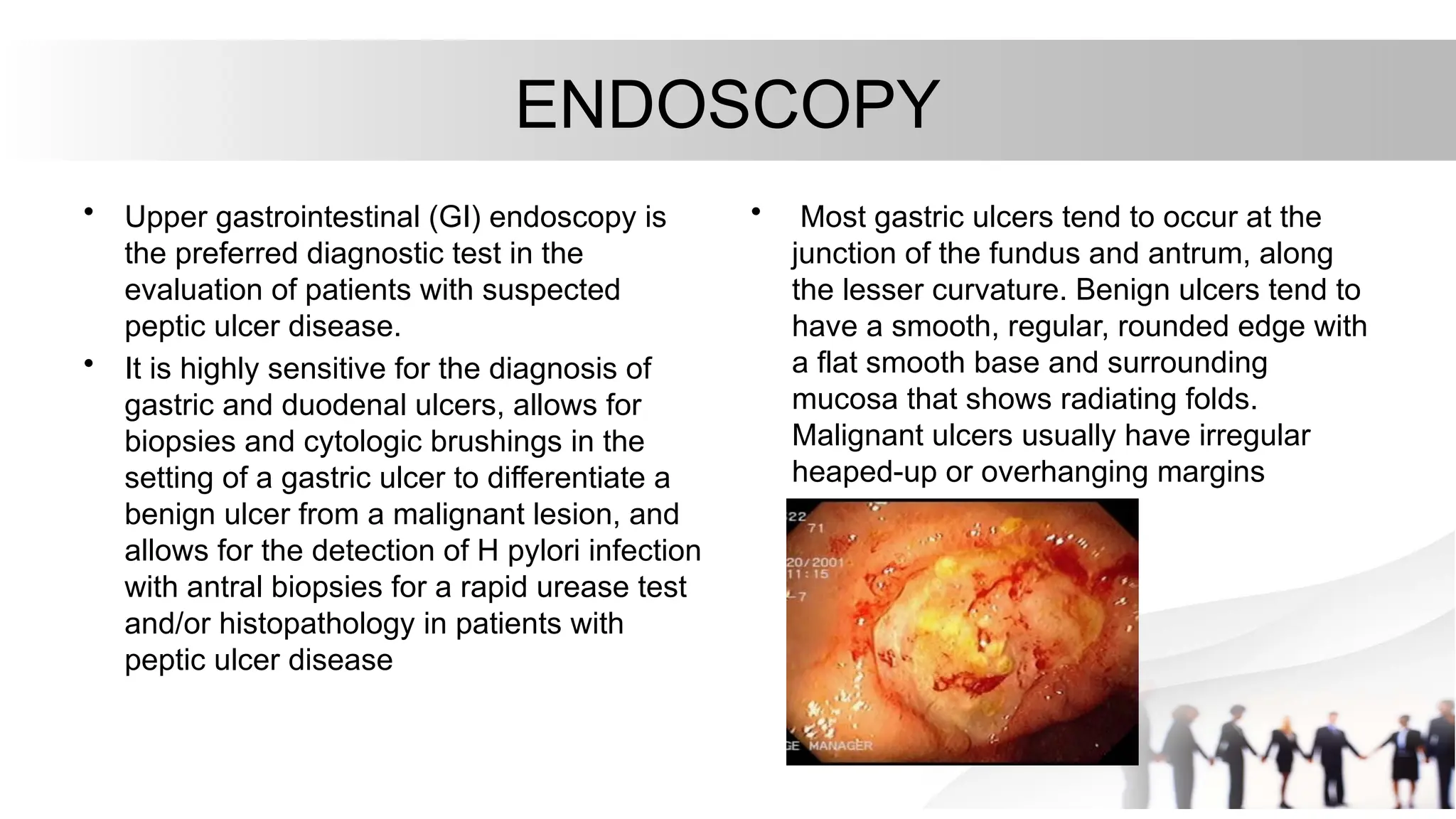
• Upper gastrointestinal(GI) endoscopy is
the preferred diagnostic test in the
evaluation of patients with suspected
peptic ulcer disease.
• It is highly sensitive for the diagnosis of
gastric and duodenal ulcers, allows for
biopsies and cytologic brushings in the
setting of a gastric ulcer to differentiate a
benign ulcer from a malignant lesion, and
allows for the detection of H pylori infection
with antral biopsies for a rapid urease test
and/or histopathology in patients with
peptic ulcer disease
• Most gastric ulcers tend to occur at the
junction of the fundus and antrum, along
the lesser curvature. Benign ulcers tend to
have a smooth, regular, rounded edge with
a flat smooth base and surrounding
mucosa that shows radiating folds.
Malignant ulcers usually have irregular
heaped-up or overhanging margins
20.
• RADIOGRAPHY
• Inpatients presenting acutely, a chest
radiograph may be useful to detect free
abdominal air when perforation is
suspected. On upper gastrointestinal (GI)
contrast study with water-soluble contrast,
the extravasation of contrast indicates
gastric perforation. Replaced with
endoscopy
• Angiography
• Angiography may be necessary in patients
with a massive gastrointestinal bleed in
whom endoscopy cannot be performed. An
ongoing bleeding rate of 0.5 mL/min or
more is needed for the angiography to be
able to accurately identify the bleeding
source. Angiography can depict the source
of the bleeding and can help provide
needed therapy in the form of a direct
injection of vasoconstrictive agents.
21.
Emergency Department Workup
•The emergency department (ED) workup will vary depending on presentation and includes
the following:
• Complete blood cell (CBC) count is used to evaluate acute or chronic blood loss.
• Electrolytes, blood urea nitrogen (BUN), and creatinine levels are useful tests for critical-
appearing patients who require fluid resuscitation
• Type and screen and crossmatched blood for transfusion is indicated in unstable or
potentially critical patients.
• Activated partial thromboplastin time (aPTT), prothrombin time (PT) and international
normalized ratio (INR) are indicated in patients with active bleeding and those on
anticoagulants.
• Amylase, lipase, and liver transaminase levels can be helpful to rule out other common
causes of epigastric pain.
• Patients younger than 55 years with no alarm features should be referred for noninvasive
testing for H pylori infection in the outpatient setting
22.
DIFFERENTIAL DIAGNOSIS
• Neoplasmof the stomach
• Pancreatitis
• Pancreatic cancer
• Diverticulitis
• Nonulcer dyspepsia (also called functional dyspepsia)
• Cholecystitis
• Gastritis
• GERD
• MI—not to be missed if having chest pain
23.
TREATMENT
• Medications: Tripletherapy for 14 days is considered the treatment of choice.
– Proton Pump Inhibitor + clarithromycin and amoxicillin
Omeprazole (Prilosec)
Lansoprazole (Prevacid)
Rabeprazole (Aciphex)
Esomeprazole (Nexium)
Clarithromycin (Biaxin)
Amoxicillin (Amoxil)
Can substitute Flagyl 500 mg PO bid for 14 d if allergic to PCN
– In the setting of an active ulcer, continue qd proton pump inhibitor therapy
for additional 2 weeks.
• Goal: complete elimination of H. Pylori. Once achieved reinfection rates are
low. Compliance!
24.
TREATMENT
• Medications—treat withProton Pump Inhibitors or H2 receptor
antagonists to assist ulcer healing
– H2: Tagament, Pepcid, Axid, or Zantac for up to 8 weeks
– PPI: Prilosec, Prevacid, Nexium, Protonix, or Aciphex for 4-8
weeks.
Alternative triple-therapy regimens
PPI + Clarithromycin (Biaxin): 500 mg PO bid +Metronidazole (Flagyl): 500 mg PO bid
Quadruple therapy:
• PPI, standard dose
• Bismuth 525 mg PO qid
• Metronidazole 500 mg PO qid
• Tetracycline 500 mg PO qid
25.
SURGERY
• People whodo not respond to medication, or who develop
complications:
– Vagotomy - cutting the vagus nerve to interrupt messages sent
from the brain to the stomach to reducing acid secretion.
– Antrectomy - remove the lower part of the stomach (antrum),
which produces a hormone that stimulates the stomach to
secrete digestive juices. A vagotomy is usually done in
conjunction with an antrectomy.
– Pyloroplasty - the opening into the duodenum and small
intestine (pylorus) are enlarged, enabling contents to pass
more freely from the stomach. May be performed along with a
vagotomy.
26.
COMPLICATIONS
• Perforation &Penetration—into pancreas, liver and retroperitoneal
space
• Peritonitis
• Bowel obstruction, Gastric outflow obstruction, & Pyloric stenosis
• Bleeding--occurs in 25% to 33% of cases and accounts for 25% of
ulcer deaths.
• Gastric CA
27.
• The indicationsfor urgent surgery include failure to achieve hemostasis endoscopically,
recurrent bleeding despite endoscopic attempts at achieving hemostasis (many advocate
surgery after two failed endoscopic attempts), and perforation
• Several modalities of endoscopic therapy are available, such as injection therapy,
coagulation therapy, hemostatic clips, argon plasma coagulator, and combination therapy.
Injection therapy is performed with epinephrine in a 1:10,000 dilution or with absolute
alcohol.
• Thermal endoscopic therapy is performed with a heater probe, bipolar circumactive probe,
or gold probe. Pressure is applied to cause coagulation of the underlying artery (coaptive
coagulation).
• Combination therapy with epinephrine injection followed by thermal coagulation appears to
be more effective than monotherapy for ulcers with a visible vessel, active hemorrhage, or
adherent clot.
28.
• Emergency operationsfor peptic ulcer perforation carry a mortality risk of 6-30%. Factors
associated with higher mortality in this setting include the following:
• Shock at the time of admission
• Renal insufficiency
• Delaying the initiation of surgery for more than 12 hours after presentation
• Concurrent medical illness (eg, cardiovascular disease, diabetes mellitus)
• Age older than 70 years
• Cirrhosis
• Immunocompromised state
• Location of ulcer (mortality associated with perforated gastric ulcer is twice that associated
with perforated duodenal ulcer)
29.
Emergency Department Care
•Treatment goals in the acute setting are the relief of discomfort and protection of the gastric
mucosal barrier to promote healing. Administer supportive therapy as needed. Most patients with
gastritis or peptic ulcer disease do not require acute interventions.
• High-risk patients include those with the following characteristics:
• Bleeding with hemodynamic instability
• Failure to clear with gastric lavage
• Coagulopathy
• Comorbid disease (especially cardiac, pulmonary, or renal)
• Advanced age
Bleeding
• Massive gastric bleeds are the most difficult complication to treat. Mainstays of resuscitation
include the following:
• Nasogastric suction helps to keep the stomach empty and contracted.
• IV PPI has been shown to reduce mortality in upper GI bleeds and reduces the incidence of rebleeding and
the need for surgical intervention [65] ; emergent surgical or endoscopic intervention may be required
30.
LIFESTYLE CHANGES
• DiscontinueNSAIDs and use Acetaminophen for pain control if
possible.
• Acid suppression--Antacids
• Smoking cessation
• No dietary restrictions unless certain foods are associated with
problems.
• Alcohol in moderation
– Men under 65: 2 drinks/day
– Men over 65 and all women: 1 drink/day
• Stress reduction

![Emergency Department Care
• Treatment goals in the acute setting are the relief of discomfort and protection of the gastric
mucosal barrier to promote healing. Administer supportive therapy as needed. Most patients with
gastritis or peptic ulcer disease do not require acute interventions.
• High-risk patients include those with the following characteristics:
• Bleeding with hemodynamic instability
• Failure to clear with gastric lavage
• Coagulopathy
• Comorbid disease (especially cardiac, pulmonary, or renal)
• Advanced age
Bleeding
• Massive gastric bleeds are the most difficult complication to treat. Mainstays of resuscitation
include the following:
• Nasogastric suction helps to keep the stomach empty and contracted.
• IV PPI has been shown to reduce mortality in upper GI bleeds and reduces the incidence of rebleeding and
the need for surgical intervention [65] ; emergent surgical or endoscopic intervention may be required](https://image.slidesharecdn.com/pepticulcerdisease-250401161023-ce0ad1a2/75/PEPTIC-ULCER-DISEASE-everything-needed-to-know-29-2048.jpg)