Downloaded 12 times









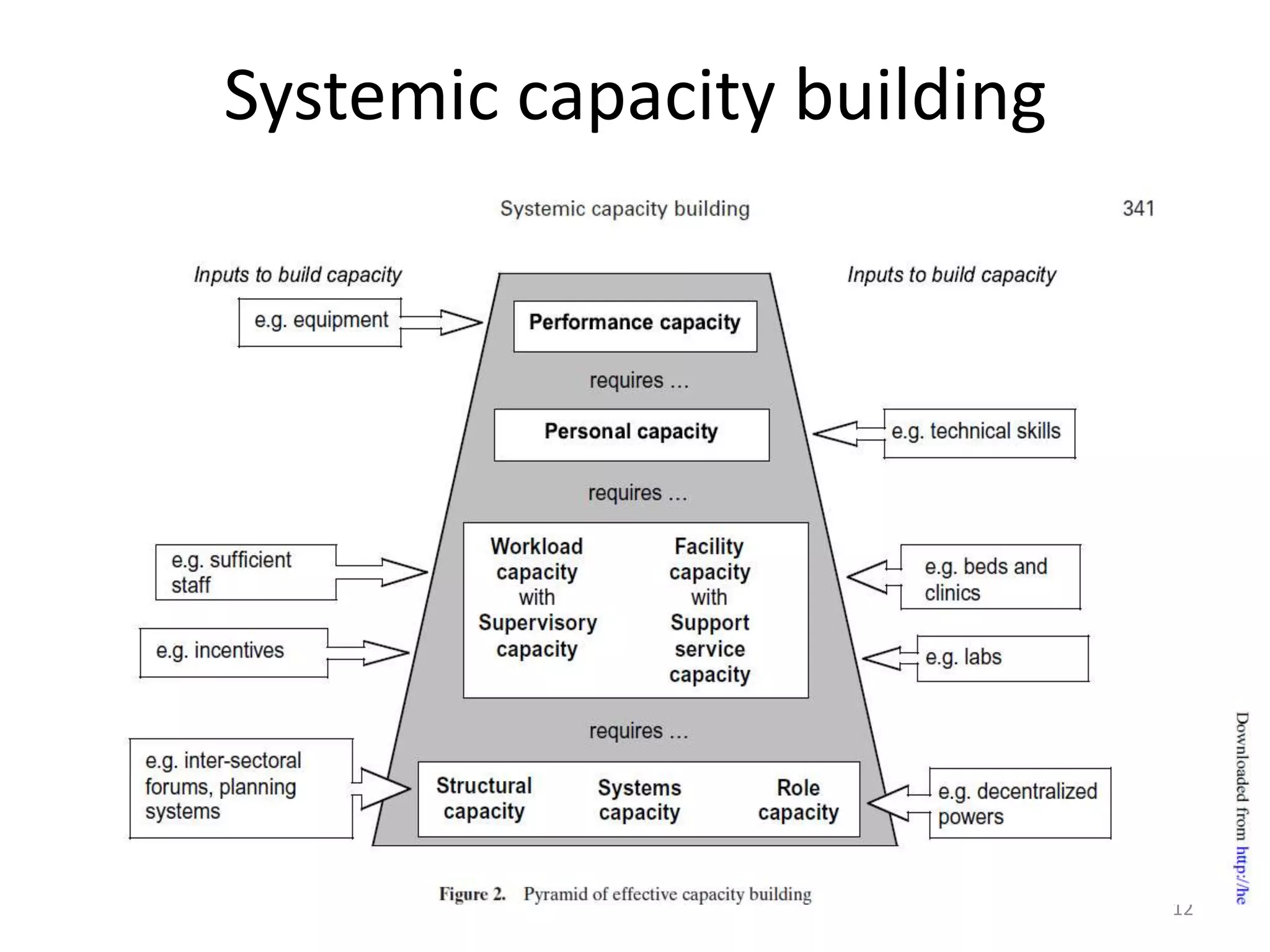










The document discusses capacity building in the public health sector of Chhattisgarh, India. It notes that capacity building refers to creating, expanding, or upgrading desired capabilities that can be drawn on over time, rather than just managing existing resources. It provides statistics on Chhattisgarh's population and health infrastructure, noting a large rural population and shortage of facilities. It also outlines issues with training capacity, quality, and rationalizing trained human resources. It discusses the state's policy decisions around strengthening training institutions and prioritizing certain programs to build capacity in the public health workforce.



































































