Download to read offline

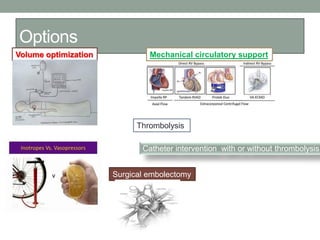
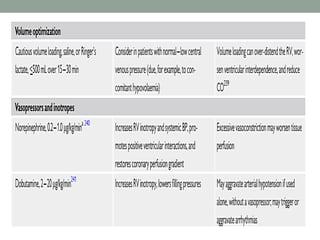
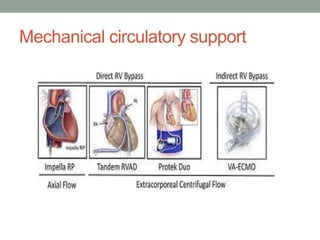
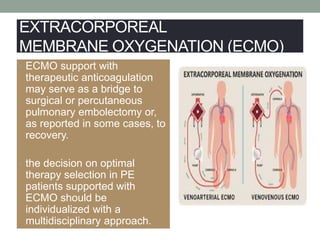
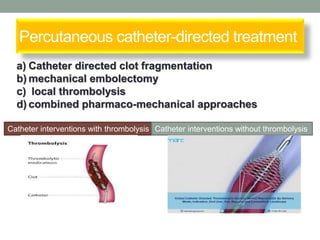
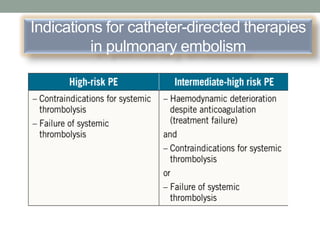
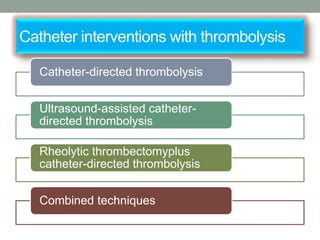
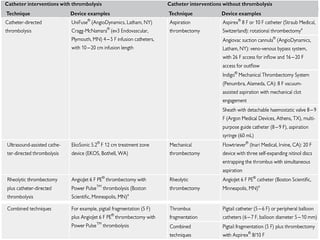
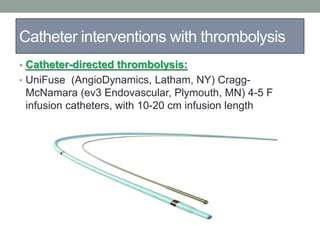


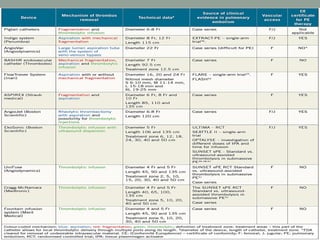
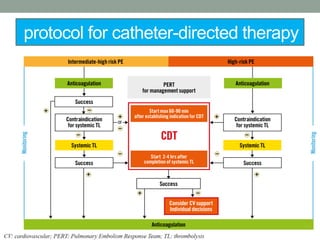

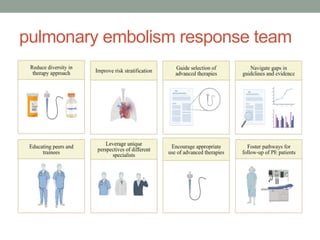
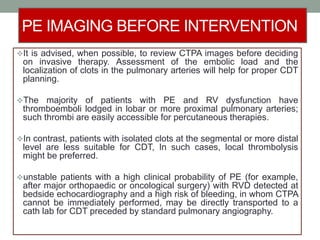


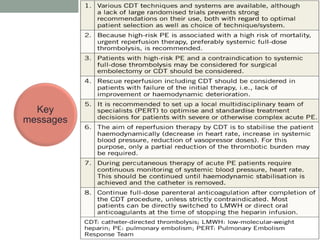

The document discusses various management strategies for pulmonary embolism (PE), emphasizing that treatment should be tailored to individual patient needs and local healthcare resources. It covers non-pharmacological interventions such as catheter-directed therapies, surgical embolectomy, and mechanical circulatory support options like ECMO and Impella RP, highlighting their indications and efficacy. Protocols for catheter-directed interventions include patient assessment, procedure steps, and post-treatment management to ensure optimal outcomes.

























































