PD article Cosmetic, aesthetic or restorative_ (1)

This document discusses issues with cosmetic or aesthetic dentistry when it is not practiced as part of comprehensive restorative dentistry. The author expresses concern that some cosmetic dentists focus only on appearance and disregard patient oral health and function. Examples are given of cases where improper cosmetic procedures led to problems like loss of tooth structure, premature restoration failure, and patient harm. The author argues that successful cosmetic dentistry requires understanding all aspects of restorative dentistry like occlusion, periodontal health, and risk assessment. Clinical cases are presented that illustrate the need to address underlying dental issues before focusing on appearance. The future of cosmetic dentistry, according to the author, relies on training that incorporates all elements of restor

Recommended
More Related Content
What's hot
What's hot (20)
Similar to PD article Cosmetic, aesthetic or restorative_ (1)
Similar to PD article Cosmetic, aesthetic or restorative_ (1) (20)
PD article Cosmetic, aesthetic or restorative_ (1)
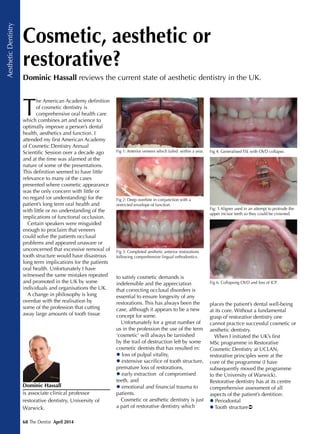
- 1. 68 The Dentist April 2014 AestheticDentistry T he American Academy definition of cosmetic dentistry is comprehensive oral health care which combines art and science to optimally improve a person’s dental health, aesthetics and function. I attended my first American Academy of Cosmetic Dentistry Annual Scientific Session over a decade ago and at the time was alarmed at the nature of some of the presentations. This definition seemed to have little relevance to many of the cases presented where cosmetic appearance was the only concern with little or no regard (or understanding) for the patient’s long term oral health and with little or no understanding of the implications of functional occlusion. Certain speakers were misguided enough to proclaim that veneers could solve the patients occlusal problems and appeared unaware or unconcerned that excessive removal of tooth structure would have disastrous long term implications for the patients oral health. Unfortunately I have witnessed the same mistakes repeated and promoted in the UK by some individuals and organisations the UK. A change in philosophy is long overdue with the realisation by some of the profession that cutting away large amounts of tooth tissue Cosmetic, aesthetic or restorative? to satisfy cosmetic demands is indefensible and the appreciation that correcting occlusal disorders is essential to ensure longevity of any restorations. This has always been the case, although it appears to be a new concept for some. Unfortunately for a great number of us in the profession the use of the term ‘cosmetic’ will always be tarnished by the trail of destruction left by some cosmetic dentists that has resulted in: loss of pulpal vitality, extensive sacrifice of tooth structure, premature loss of restorations, early extraction of compromised teeth, and emotional and financial trauma to patients. Cosmetic or aesthetic dentistry is just a part of restorative dentistry which places the patient’s dental well-being at its core. Without a fundamental grasp of restorative dentistry one cannot practice successful cosmetic or aesthetic dentistry. When I initiated the UK’s first MSc programme in Restorative Cosmetic Dentistry at UCLAN, restorative principles were at the core of the programme (I have subsequently moved the programme to the University of Warwick). Restorative dentistry has at its centre comprehensive assessment of all aspects of the patient’s dentition: Periodontal Tooth structure Dominic Hassall is associate clinical professor restorative dentistry, University of Warwick. Dominic Hassall reviews the current state of aesthetic dentistry in the UK. Fig 1: Anterior veneers which failed within a year. Fig 2: Deep overbite in conjunction with a restricted envelope of function. Fig 3: Completed aesthetic anterior restorations following comprehensive lingual orthodontics. Fig 4: Generalised TSL with OVD collapse. Fig: 5 Aligner used in an attempt to protrude the upper incisor teeth so they could be crowned. Fig 6: Collapsing OVD and loss of ICP.
- 2. 70 The Dentist April 2014 AestheticDentistry Occlusion Aesthetic Aesthetics is just one component of restorative dentistry and unless there is an understanding of the other components there will be premature failure of the aesthetic dentistry. Restorative dentistry also has at its centre risk assessment and multidisplinary long term treatment planning, not short term poorly planned quick fix cosmetic solutions or quick fix solutions for the benefit of the dentist’s bank balance. The future is restorative Without a thorough understanding of all aspects of restorative dentistry including functional occlusion and the perio:restorative interface all restorative, aesthetic or cosmetic dentistry will fail prematurely. Smile design and aesthetic appearance is just one important but relatively simple part of the restorative jigsaw puzzle. It is only with comprehensive postgraduate training in all aspects of restorative dentistry, delivered by appropriately trained and experienced individuals that comprehensive long lasting aesthetic dentistry can be delivered to the benefit of our patients. The following cases illustrate why a fundamental grasp of all aspects of restorative dentistry is the essential key in successful predictable aesthetic dentistry Clinical cases The following are some examples of common mistakes I have witnessed being regularly repeated. Figures 1-3 present an inappropriate veneer case undertaken in a patient with a deep overbite and restricted envelope of function. All the veneers debonded with a year. Comprehensive orthodontics was required to correct the occlusal disorder prior to the veneers being replaced. Figures 4-6 presents a poorly planned case where an aligner system was used in an attempt to protrude the anterior teeth so they could be ‘simply’ crowned. However there has been a failure to appreciate the actively collapsing occlusal vertical dimension (OVD) and loss of intercuspal position (ICP) due to extensive tooth surface loss (TSL) and loss of cuspal anatomy. The case requires an increase in Fig 7: Upper arch ‘smile makeover’. Fig 8: Biologic width violation. Fig 9: Absence of TSL on posteriors with incisal and palatal TSL to the ICP on the upper incisors. Fig 10: Patient smiling indicating high smile line. Fig 11: Incisal and palatal TSL to the ICP. Fig 12: Incisal and buccal TSL. OVD and protective covering of the exposed dentine and reintroduction of an ICP that the patient can locate. Only this will ensure long term occlusal stability and long term success of any anterior ‘cosmetic restorations’. The case also requires aesthetic and structural surgical crown lengthening. Figures 7 and 8 highlight a poorly executed ‘cosmetic smile makeover’. The entire upper arch had been restored with anterior veneers and posterior bridges. There were numerous faults including no control in tooth preparation technique resulting in poor margins on some restorations which resulted in violation of the biologic width and sore bleeding gums for the patient despite excellent oral hygiene. The UR1 had been over prepared and had become non vital requiring endodontic treatment and had also discoloured. There was a large slide from RCP (retruded contact position) to ICP which contributed to the UL2 veneer debonding within months, although excessive preparation and bonding wholly to dentine has contributed. In the final case (figures 9-12) a ‘cosmetic centre’ had recommended veneers on the upper incisor teeth to improve the cosmetic appearance. Unfortunately as in the first case this young patient has a restricted envelope of function with tooth surface loss (TSL) on the upper incisor teeth affecting the incisal and palatal surfaces finishing at the ICP position and incisal and buccal TSL on the lower incisor teeth, with absence of TSL on the posterior teeth. This patient requires orthodontics to correct the occlusal disorder and realign the upper incisor teeth. The patient would also benefit from improvement to the excessive gingival display. Simply placing veneers would risk giving the anterior teeth a square masculine appearance. The veneers would be subject to premature failure due to excessive frictional forces. Acknowledgements I am indebted to Peter Huntley of Orthodontic Excellence for the orthodontic treatment in case one.