
Download to read offline








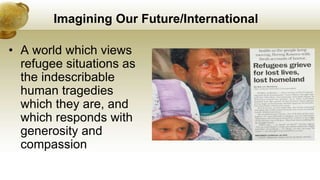



























The document outlines key discussions and insights from the North American Refugee Health Conference held in Niagara Falls, emphasizing the historical context and current challenges of refugee health. It advocates for improved practices, including better access to healthcare, compassion in treatment, and universal access to services for refugees. The author calls for transformative approaches in refugee health, such as leveraging technology and the importance of listening to refugees' stories and needs.









































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)














