Download to read offline

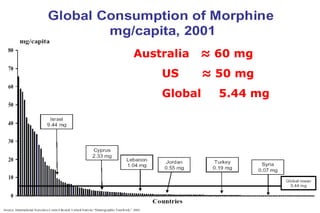

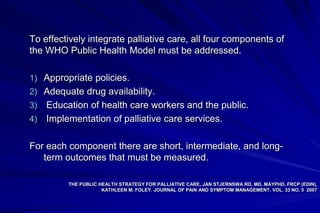
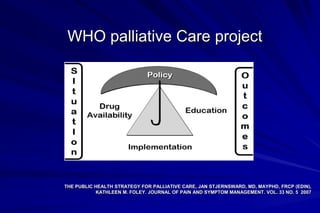


1) Palliative care aims to improve quality of life for patients facing life-threatening illness through pain and symptom relief. 2) A WHO demonstration project in Jordan helped establish palliative care policies, increase opioid availability, and provide education to healthcare workers. 3) The Jordan Palliative Care Society was formed to help implement palliative care across the country through additional training, ensuring drug access, and creating a palliative care network.




























![Care_giving_in_different_setting_ppt[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/caregivingindifferentsettingppt1-230822052012-56dc9f7f-thumbnail.jpg?width=640&height=640&fit=bounds)
















![1051شكر مؤسسة السديل للعلاج التلطيفي[1]](https://cdn.slidesharecdn.com/ss_thumbnails/10511-101210123144-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)


















