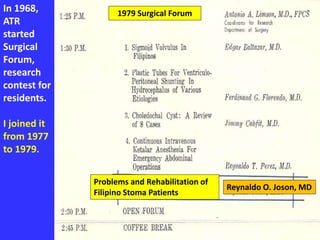
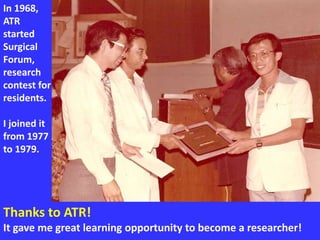
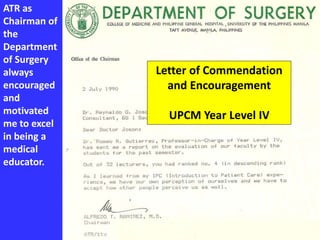
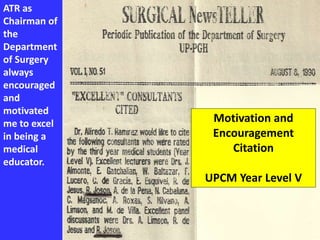
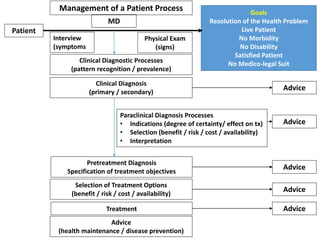
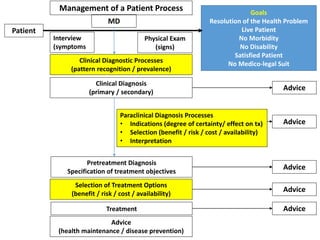
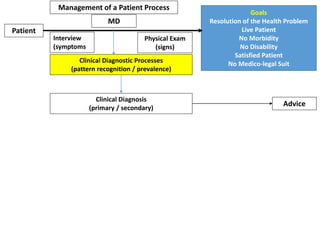
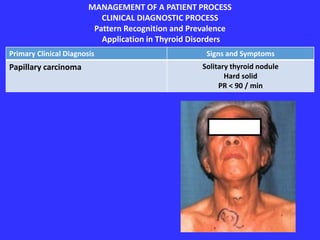
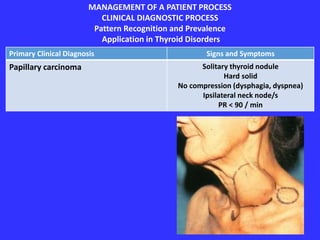
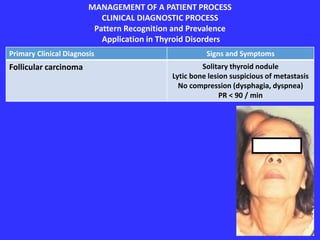
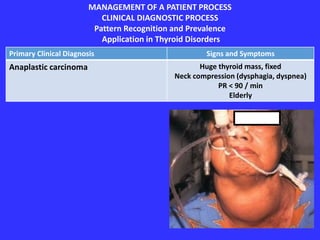
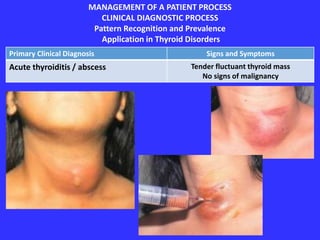
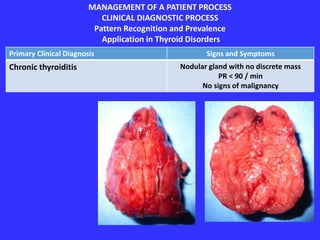
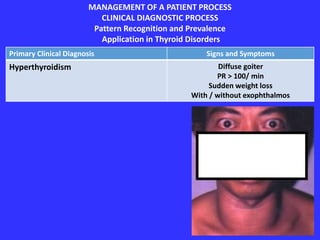
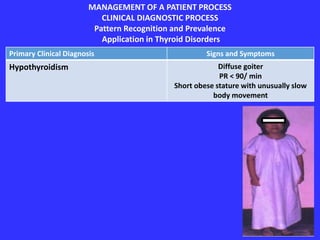
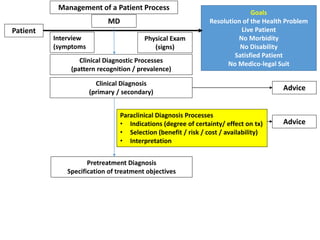
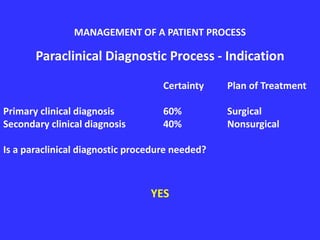
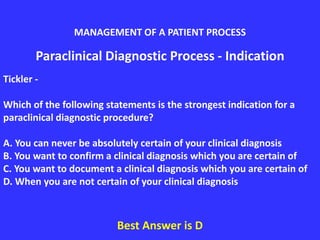
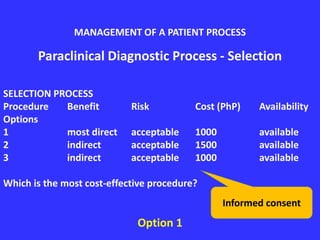
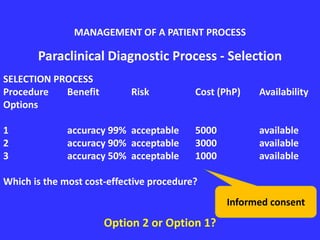
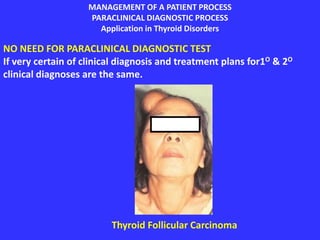
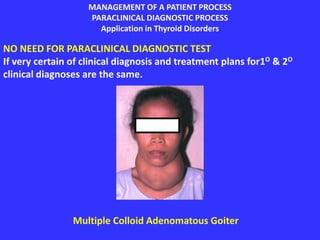
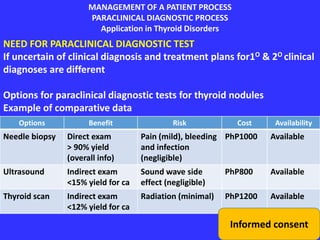
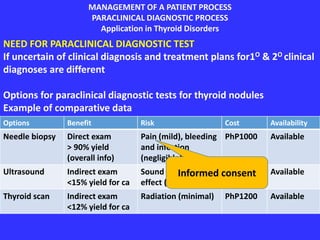
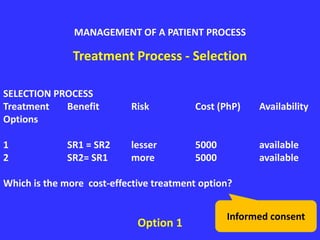
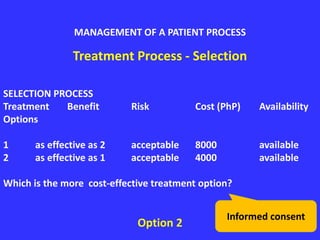
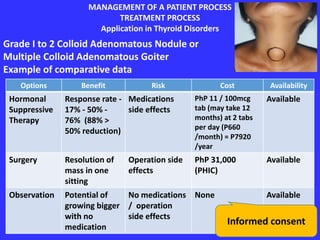
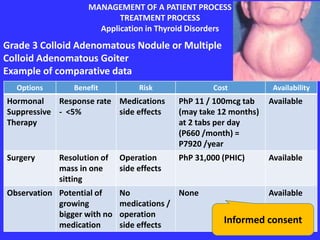
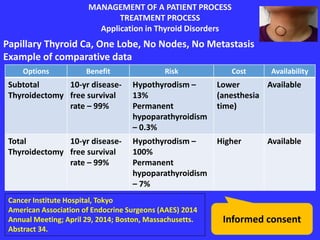
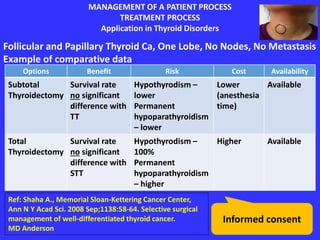
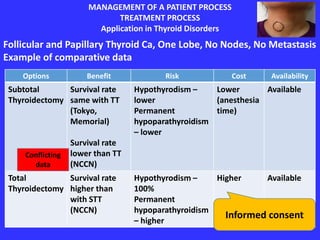
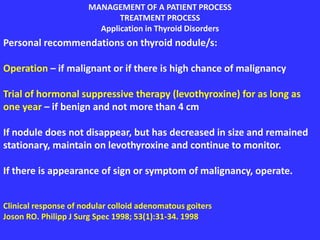
The document discusses the 16th Chancellor Alfredo T. Ramirez Memorial Lecture delivered by Reynaldo O. Joson, MD, highlighting the application of management processes in the treatment of thyroid nodules based on 30 years of experience. It emphasizes the importance of clinical diagnosis through pattern recognition and prevalence in thyroid disorders and details the decision-making processes for treatment plans. The lecture honors Dr. Ramirez's contributions to medical education, research, and surgical training in the Philippines.


















































![CURRICULUM VITAE AS CV 2015[1]](https://cdn.slidesharecdn.com/ss_thumbnails/3bad0f39-2a91-484d-9ef2-4d967874acff-160524142815-thumbnail.jpg?width=640&height=640&fit=bounds)



































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)








![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)






