Downloaded 113 times
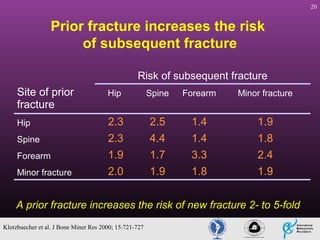
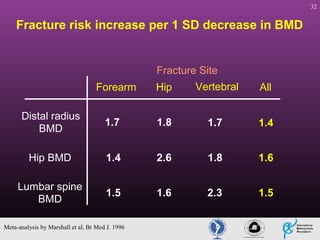



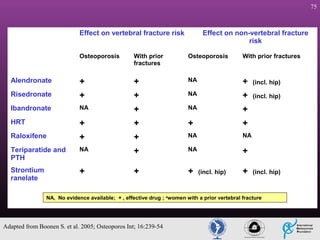

Fragility fractures represent a major global health problem. Orthopaedic surgeons have a unique opportunity to improve outcomes for fracture patients by addressing the underlying osteoporosis. Currently, few fracture patients receive evaluation and treatment for osteoporosis despite the condition increasing their risk of future fractures 2-5 times. There is a need for orthopaedic surgeons to play a more active role in optimizing care through evaluating bone mineral density, educating patients on osteoporosis risks, and facilitating referrals to ensure fracture patients receive treatment to prevent future fractures.













![Avulsion fractures ppt [1]](https://cdn.slidesharecdn.com/ss_thumbnails/avulsionfracturespptashleyandsarahmusculo1-101129093116-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)



![Osteosarcoma[2]](https://cdn.slidesharecdn.com/ss_thumbnails/osteosarcoma2-130423123803-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)










































![Osteoporosis%203rd%20yr[1]](https://cdn.slidesharecdn.com/ss_thumbnails/osteoporosis203rd20yr1-111103005118-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)








![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)















