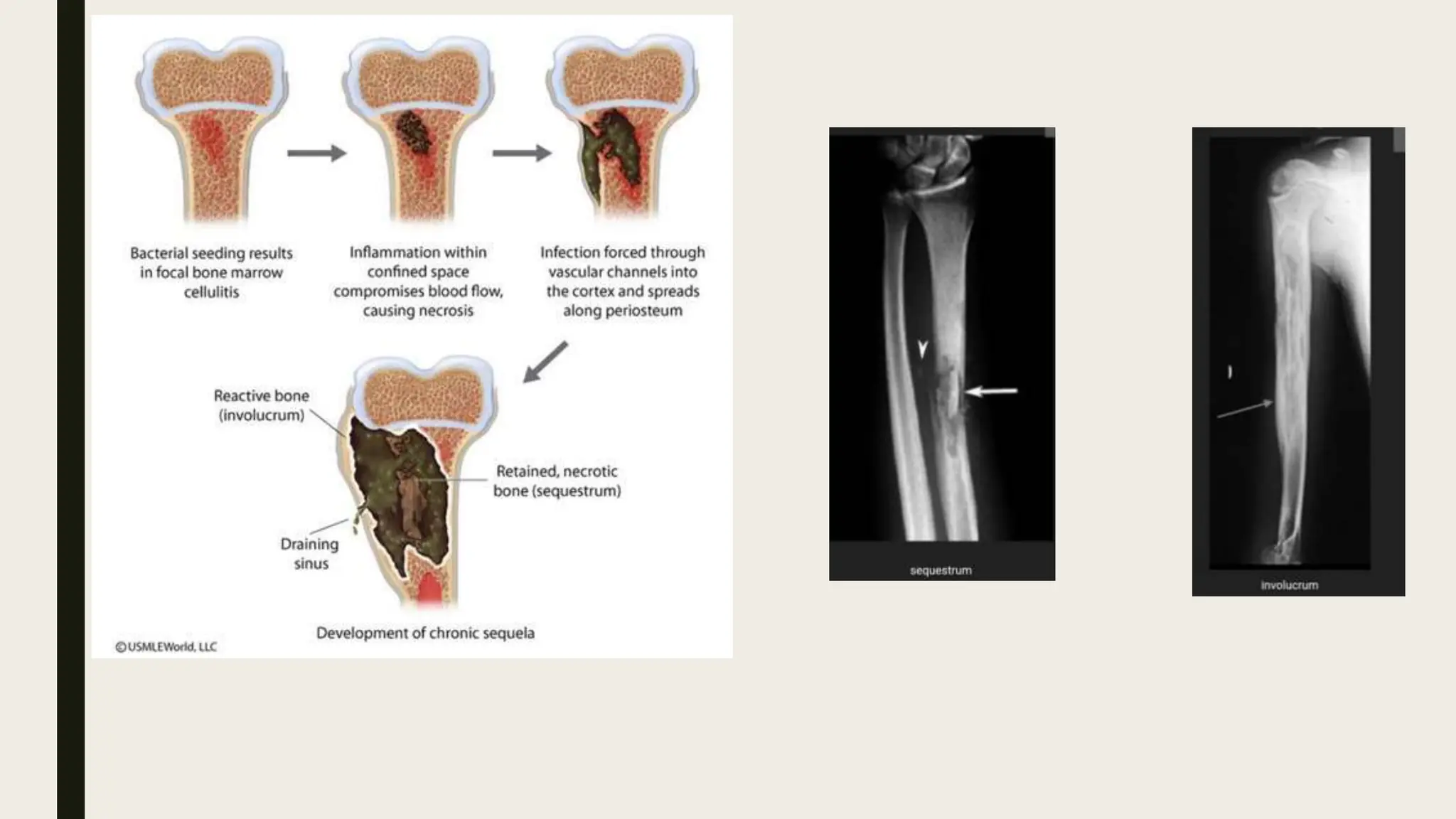
Osteomyelitis is an infection and inflammation of bone and bone marrow that is typically caused by bacteria. It can occur through hematogenous spread, direct inoculation from injuries, or contiguous spread from nearby infected tissues. Common risk factors include recent trauma, immunocompromised status, IV drug use, and diabetes. Diagnosis involves physical exam, imaging like x-rays, CT, or MRI, and lab tests. Treatment depends on factors like infection severity and location but may include antibiotics, debridement, irrigation, suppressive antibiotic therapy, hyperbaric oxygen therapy, or amputation in severe cases. Complications can include ongoing or worsening infection, amputation, sepsis, and in rare cases, malignant transformation of