Original Study
Type of Breast Cancer Diagnosis, Screening,
and Survival
Carla Cedolini,1 Serena Bertozzi,1 Ambrogio P. Londero,2 Sergio Bernardi,3,4
Luca Seriau,1 Serena Concina,1 Federico Cattin,1 Andrea Risaliti1
Abstract
Organized, invitational breast cancer screening in our population succeeded in detecting early-stage tumors,
which have been consequently treated more frequently with breast and axillary conservative surgery, com-
plementary breast irradiation, and eventual hormonal therapy. The diagnosis of invasive cancer with screening
in our population resulted in a survival gain at 5 years from the diagnosis.
Introduction: Breast cancer screening is known to reduce mortality. In the present study, we analyzed the prevalence
of breast cancers detected through screening, before and after introduction of an organized screening, and we
evaluated the overall survival of these patients in comparison with women with an extrascreening imaging-detected
breast cancer or those with palpable breast cancers. Materials and Methods: We collected data about all women
who underwent a breast operation for cancer in our department between 2001 and 2008, focusing on type of tumor
diagnosis, tumor characteristics, therapies administered, and patient outcome in terms of overall survival, and re-
currences. Data was analyzed by R (version 2.15.2), and P < .05 was considered significant. Results: Among the 2070
cases of invasive breast cancer we considered, 157 were detected by regional mammographic screening (group A),
843 by extrascreening breast imaging (group B: 507 by mammography and 336 by ultrasound), and 1070 by extra-
screening breast objective examination (group C). The 5-year overall survival in groups A, B, and C were, respectively,
99% (95% CI, 98%-100%), 98% (95% CI, 97%-99%), and 91% (95% CI, 90%-93%), with a significant difference
between the first 2 groups and the third (P < .05) and a trend between groups A and B (P ¼ .081). Conclusion: The
diagnosis of invasive breast cancer with screening in our population resulted in a survival gain at 5 years from the
diagnosis, but a longer follow-up is necessary to confirm this data.
Clinical Breast Cancer, Vol. 14, No. 4, 235-40 ª 2014 Elsevier Inc. All rights reserved.
Keywords: Breast cancer, Breast cancer screening, Invasive breast cancer, Mammographic screening, Overall survival
Introduction
Because of the detection of early-stage tumors, breast cancer
screening reduced breast cancer mortality in Europe by 25%-31%
in patients who were invited for screening and by 38%-48% in
those who were actually screened during the last decade of the
twentieth century and the first decade of the twenty-first.1 In our
region of Italy, an organized breast cancer screening was firstly intro-
duced in 2005, but despite the high compliance of invited women
1Clinic of Surgery
2Clinic of Obstetrics and Gynecology
University of Udine, Udine, Italy
3Department of Surgery, Ospedale Civile di Latisana, Udine, Italy
4 ...
A prospective study of breast lump andclinicopathologicalanalysis in relation...iosrjce
IOSR Journal of Dental and Medical Sciences is one of the speciality Journal in Dental Science and Medical Science published by International Organization of Scientific Research (IOSR). The Journal publishes papers of the highest scientific merit and widest possible scope work in all areas related to medical and dental science. The Journal welcome review articles, leading medical and clinical research articles, technical notes, case reports and others.
A prospective study of breast lump andclinicopathologicalanalysis in relation...iosrjce
IOSR Journal of Dental and Medical Sciences is one of the speciality Journal in Dental Science and Medical Science published by International Organization of Scientific Research (IOSR). The Journal publishes papers of the highest scientific merit and widest possible scope work in all areas related to medical and dental science. The Journal welcome review articles, leading medical and clinical research articles, technical notes, case reports and others.
Colorectal cancer screening and subsequent incidence of colorectal cancer: re...Cancer Council NSW
Colorectal cancer screening and subsequent incidence of colorectal cancer: results from the 45 and Up Study
Annika Steffen, Marianne F Weber, David M Roder and Emily Banks
A retrospective study on ovarian cancer with a median follow-up of 36 months ...AI Publications
Ovarian cancer is relatively common but serious and has a poor prognosis. The aim of this study is to highlight the epidemiological, diagnostic, therapeutic and evolutionary aspects of this malignant pathology managed at the Bejaia university hospital center. This is a retrospective and descriptive study over a period of 3 years (2019 - 2022) carried out on 20 patients who developed ovarian cancer. The average age of the patients was 50 years old, 53.23% of whom were over 45 years old. The CA-125 blood test was positive in 18 out of 20 patients. The tumors were discovered on ultrasound in 87.10% of cases and at laparotomy in 12.90%. Total hysterectomy with bilateral adnexectomy was the most performed procedure (64.52%). The early postoperative course was simple. 15 patients underwent second look surgery (16.13%) for locoregional recurrences. Epithelial tumors were the most frequent histological type (93.55%), including 79% in the advanced stage ( IIIc -IV) and 21% in the early stage (Ia- Ib ). Adjuvant chemotherapy was administered in 80% of patients. With a median follow-up of 36 months, 2 patients were lost to follow-up. The evolution was favorable in 27.42% and in 25.81% deaths occurred late postoperatively. Ovarian cancer is not common but serious given the advanced stages and the high rate of late postoperative deaths which were largely observed in patients deprived of adequate neoadjuvant or adjuvant chemotherapy.
Twenty five year follow up for breast cancer incidence 12-feb2014Miguel Pizzanelli
Twenty five year follow-up for breast cancer incidence
and mortality of the Canadian National Breast
Screening Study: randomised screening trial
OPEN ACCESS
Anthony B Miller professor emeritus, Claus Wall data manager, Cornelia J Baines professor
emerita, Ping Sun statistician , Teresa To senior scientist , Steven A Narod professor Dalla Lana School of Public Health, University of Toronto, Toronto, Ontario M5T 3M7, Canada; 2Women’s College Research Institute, Women’s College Hospital, Toronto, Ontario M5G 1N8, Canada; 3Child Health Evaluative Services, The Hospital for Sick Children, Toronto, Ontario, Canada
Primary small cell breast carcinoma represents less than 1% of breast cancers. Due to its rarity, there are no uniformly accepted guidelines for treatment. Its prognosis is varied being generally regarded as worse than that of most breast cancers and it poses unique diagnostic challenges. We present a case of primary small cell breast cancer, rationale for our management strategies with reference to the published literature to serve as a guide to the management of this rare cancer of the breast.
1. Primary sources2. Secondary sources3. La Malinche4. Bacon’s.docxvannagoforth
1. Primary sources
2. Secondary sources
3. La Malinche
4. Bacon’s rebellion
5. Robert Carter III
6. Mesoamerica
7. Middle Passage
8. Indentured servitude
9. The Jefferson-Hemings Controversy
10. Triangular trade
11. Saint Dominique Revolt
12. Syncretism
13. Olaudah Equiano
14. Christopher Columbus
15. Columbian Moment
16. Hernan Cortes
17. Florentine Codex
18. Master Narrative of American History
19. Reconquista
20. The Paradox of Slavery
21. Indian Removal Act 1830
22. Trail of Tears
23. Treaty of Guadalupe Hidalgo
24. Niños Heroes (Heroic Children)
25. Antonio López de Santa Anna y Pérez de Lebrón
26. The Royal Africa Company
27. John Locke
28. St. Patrick’s Battalion
29. Chilam Balam
30. Popol Vuh
31. El requerimiento (The Requirement)
32. Manifest Destiny
33. Moses and Stephen F. Austin
34. Colonialism
35. Colonial Legacy
.
1. Prepare an outline, an introduction, and a summary.docxvannagoforth
1. Prepare
an outline
,
an introduction
, and
a summary
on the article selected. It s
hould be
a report of at least 4 page
double spaced.
2. Prepare a 4
PowerPoint slides
from the report.
NOTE
: See the attachment below to review the article.
.
1. Normative moral philosophy typically focuses on the determining t.docxvannagoforth
1. Normative moral philosophy typically focuses on the determining the right action for a person to perform in a given situation. First, how specifically is Aristotle’s virtue ethics focused slightly differently? Next, Aristotle thought that virtues are traits of character that manifest themselves through habitual activity and that are good for anyone to have. What are some of the virtuous traits to have according to Aristotle and how does acting in accordance with them over time bring about “correct” moral action? What does it mean to act in a morally correct way according to Aristotle?
Directions:
Please provide detailed and elaborate responses to the following questions. Your responses should include examples from the reading assignments. Each response should be at least one half of one page in length and utilize APA format.
1. According to virtue ethicists, how are virtues acquired?
2. What is situationist psychology?
3. List and briefly describe one of the criticisms of virtue ethics.
4. What is "The Golden Mean?"
5. Why is virtue ethics particularly well-suited to the medical profession?
PART I:
Directions:
The following problems ask you to evaluate hypothetical situations and/or concepts related to the reading in this module. While there are no "correct answers" for these problems, you must demonstrate a strong understanding of the concepts and lessons from this module's reading assignment. Please provide detailed and elaborate responses to the following problems. Your responses should include examples from the reading assignments and should utilize APA guidelines. Responses that fall short of the assigned minimum page length will not earn any points.
1.
Think of a profession you are considering as a career: engineering, or perhaps law or accounting or teaching. Could you develop a distinctive set of virtues for that profession? That is, are there some virtues that would be particularly important for members of that profession? Your response should be at least one page in length.
2. An important distinction for virtue theorists is between people who are happy and people who are flourishing. Do you know anyone (a public figure or an acquaintance) whom you would count as happy but not flourishing?
Your response should be at least one half of one page in length.
3. I have lived a dissolute life for many years: a life devoted to excessive eating, heavy drinking, laziness, deceitfulness, and pettiness. At age 45, I awaken one morning in the gutter, painfully sober after a three-day binge, and I resolve to change my ways and pursue virtue. In your opinion, how long would it make me to become a virtuous person? Could I become virtuous in an hour? A week? A month? Ever?
Your response should be at least one page in length.
4. Suppose Dan is dying from an unknown disease. He is wealthy and will give half of his money to anyone who can save his life. Joe, not know.
1. Paper should be 5-pages min. + 1 page works cited2. Should have.docxvannagoforth
1. Paper should be 5-pages min. + 1 page works cited
2. Should have at least 10 annotated sources (copy article onto word, highlight main point, write a few sentences about how it'll help you in writing the paper at the bottom of page)
3
. Should have an INTRO, NARRATION, ARGUMENTS, REFUTATION, CONCUSION
4. Use in-text citations and have organized mla format works cited page
SAMPLE OUTLINE
Research Paper Outline
Title: Rebellious Libya
Thesis: The United States should not get involved with Libya’s conflicts.
I.
Introduction:
A.
Start with the question, what is war? Explain briefly.
B.
Talk about the wars of the United States.
C.
What were the outcomes of some of those wars?
II.
Narration:
A.
Give some background on Libya.
B.
Explain how Col. Muammar Gaddafi became the leader of Libya
C.
Talk about why the citizens of Libya want to overthrow Gaddafi.
D.
Explain why the people feel that the United States should get involved in Libya’s conflicts.
III.
Partition:
A.
Thesis: I believe that the United States should not get involve with Libya’s conflicts.
B.
Essay Map.
1.
Cost of war.
2.
Using money in other Departments other defense.
3.
Killing innocent civilians and soldiers.
4.
Helping unknown rebels
5.
Involvement of foreign wars
IV.
Arguments:
A.
The cost of war is rising by the minute. The Obama Administration proposed a budget of $553 billion dollars for the department.
B.
Instead of spending all that money on war, we should be investing that money on health care and education.
C.
This conflict has caused the lives of many innocent civilians. NATO openly admitted to have killed innocent civilians, due to misguidance.
D.
The rebels fighting against Gaddafi are in need of military supplies. I don’t think that it is a good idea to help unknown rebels. We helped the Afghanistan rebels when they were fighting Russia. After they were victorious, they later became the “Taliban” and used those weapons to attack the US.
E.
Getting involved in foreign wars is not a good idea. The US has been involved in many foreign wars lately. These wars have been in foreign countries where Islam is the prominent religion. Libya is one of these countries. The involvement of the US in these places, builds a bad reputation worldwide and among the Muslim community.
V.
Refutation:
A.
Gaddafi’s actions against the civilians of Libya are totally wrong. Killing your own people is bad and therefore, we should help the rebels overthrow him.
B.
Gaddafi has been in power for many years. In fact, he holds the record for most years in power in a single country. This type of power can potentially lead to corruption and mistreatment of civilians.
C.
The people of Libya deserve to have democracy. They should have the right to elect their own leader.
D.
If Al Qaeda is threatening NATO and Libyan mercenaries then we should help them fight terrorism.
VI.
Conclusion:
A.
Summarize my arguments.
B.
State why we should not get involve with Libya’s conf.
1. Name and describe the three steps of the looking-glass self.2.docxvannagoforth
1. Name and describe the three steps of the 'looking-glass self'.
2. List and describe the three stages in George Mead's model of human development.
3. Piaget developed a four-stage process to explain how children develop reasoning skills. List each and give an example of one of the stages.
4. Briefly summarize the three elements of Freud's theory of personality and explain why sociologist have negative reactions to his analysis.
5. How does the mass media reinforce society's expectations of gender?
.
1. Provide an example of a business or specific person(s) that effec.docxvannagoforth
1. Provide an example of a business or specific person(s) that effectively use social media. What tools does the business or person use? How do they apply the tools effectively? Describe areas of improvement.
This assignment has to be 4 pages long, then it needs a cover page and reference page however that can not be a part of the four pages. So it would be 6 pages if you count the cover page and reference page!
.
More Related Content
Similar to Original StudyType of Breast Cancer Diagnosis, Screening,a.docx
Colorectal cancer screening and subsequent incidence of colorectal cancer: re...Cancer Council NSW
Colorectal cancer screening and subsequent incidence of colorectal cancer: results from the 45 and Up Study
Annika Steffen, Marianne F Weber, David M Roder and Emily Banks
A retrospective study on ovarian cancer with a median follow-up of 36 months ...AI Publications
Ovarian cancer is relatively common but serious and has a poor prognosis. The aim of this study is to highlight the epidemiological, diagnostic, therapeutic and evolutionary aspects of this malignant pathology managed at the Bejaia university hospital center. This is a retrospective and descriptive study over a period of 3 years (2019 - 2022) carried out on 20 patients who developed ovarian cancer. The average age of the patients was 50 years old, 53.23% of whom were over 45 years old. The CA-125 blood test was positive in 18 out of 20 patients. The tumors were discovered on ultrasound in 87.10% of cases and at laparotomy in 12.90%. Total hysterectomy with bilateral adnexectomy was the most performed procedure (64.52%). The early postoperative course was simple. 15 patients underwent second look surgery (16.13%) for locoregional recurrences. Epithelial tumors were the most frequent histological type (93.55%), including 79% in the advanced stage ( IIIc -IV) and 21% in the early stage (Ia- Ib ). Adjuvant chemotherapy was administered in 80% of patients. With a median follow-up of 36 months, 2 patients were lost to follow-up. The evolution was favorable in 27.42% and in 25.81% deaths occurred late postoperatively. Ovarian cancer is not common but serious given the advanced stages and the high rate of late postoperative deaths which were largely observed in patients deprived of adequate neoadjuvant or adjuvant chemotherapy.
Twenty five year follow up for breast cancer incidence 12-feb2014Miguel Pizzanelli
Twenty five year follow-up for breast cancer incidence
and mortality of the Canadian National Breast
Screening Study: randomised screening trial
OPEN ACCESS
Anthony B Miller professor emeritus, Claus Wall data manager, Cornelia J Baines professor
emerita, Ping Sun statistician , Teresa To senior scientist , Steven A Narod professor Dalla Lana School of Public Health, University of Toronto, Toronto, Ontario M5T 3M7, Canada; 2Women’s College Research Institute, Women’s College Hospital, Toronto, Ontario M5G 1N8, Canada; 3Child Health Evaluative Services, The Hospital for Sick Children, Toronto, Ontario, Canada
Primary small cell breast carcinoma represents less than 1% of breast cancers. Due to its rarity, there are no uniformly accepted guidelines for treatment. Its prognosis is varied being generally regarded as worse than that of most breast cancers and it poses unique diagnostic challenges. We present a case of primary small cell breast cancer, rationale for our management strategies with reference to the published literature to serve as a guide to the management of this rare cancer of the breast.
1. Primary sources2. Secondary sources3. La Malinche4. Bacon’s.docxvannagoforth
1. Primary sources
2. Secondary sources
3. La Malinche
4. Bacon’s rebellion
5. Robert Carter III
6. Mesoamerica
7. Middle Passage
8. Indentured servitude
9. The Jefferson-Hemings Controversy
10. Triangular trade
11. Saint Dominique Revolt
12. Syncretism
13. Olaudah Equiano
14. Christopher Columbus
15. Columbian Moment
16. Hernan Cortes
17. Florentine Codex
18. Master Narrative of American History
19. Reconquista
20. The Paradox of Slavery
21. Indian Removal Act 1830
22. Trail of Tears
23. Treaty of Guadalupe Hidalgo
24. Niños Heroes (Heroic Children)
25. Antonio López de Santa Anna y Pérez de Lebrón
26. The Royal Africa Company
27. John Locke
28. St. Patrick’s Battalion
29. Chilam Balam
30. Popol Vuh
31. El requerimiento (The Requirement)
32. Manifest Destiny
33. Moses and Stephen F. Austin
34. Colonialism
35. Colonial Legacy
.
1. Prepare an outline, an introduction, and a summary.docxvannagoforth
1. Prepare
an outline
,
an introduction
, and
a summary
on the article selected. It s
hould be
a report of at least 4 page
double spaced.
2. Prepare a 4
PowerPoint slides
from the report.
NOTE
: See the attachment below to review the article.
.
1. Normative moral philosophy typically focuses on the determining t.docxvannagoforth
1. Normative moral philosophy typically focuses on the determining the right action for a person to perform in a given situation. First, how specifically is Aristotle’s virtue ethics focused slightly differently? Next, Aristotle thought that virtues are traits of character that manifest themselves through habitual activity and that are good for anyone to have. What are some of the virtuous traits to have according to Aristotle and how does acting in accordance with them over time bring about “correct” moral action? What does it mean to act in a morally correct way according to Aristotle?
Directions:
Please provide detailed and elaborate responses to the following questions. Your responses should include examples from the reading assignments. Each response should be at least one half of one page in length and utilize APA format.
1. According to virtue ethicists, how are virtues acquired?
2. What is situationist psychology?
3. List and briefly describe one of the criticisms of virtue ethics.
4. What is "The Golden Mean?"
5. Why is virtue ethics particularly well-suited to the medical profession?
PART I:
Directions:
The following problems ask you to evaluate hypothetical situations and/or concepts related to the reading in this module. While there are no "correct answers" for these problems, you must demonstrate a strong understanding of the concepts and lessons from this module's reading assignment. Please provide detailed and elaborate responses to the following problems. Your responses should include examples from the reading assignments and should utilize APA guidelines. Responses that fall short of the assigned minimum page length will not earn any points.
1.
Think of a profession you are considering as a career: engineering, or perhaps law or accounting or teaching. Could you develop a distinctive set of virtues for that profession? That is, are there some virtues that would be particularly important for members of that profession? Your response should be at least one page in length.
2. An important distinction for virtue theorists is between people who are happy and people who are flourishing. Do you know anyone (a public figure or an acquaintance) whom you would count as happy but not flourishing?
Your response should be at least one half of one page in length.
3. I have lived a dissolute life for many years: a life devoted to excessive eating, heavy drinking, laziness, deceitfulness, and pettiness. At age 45, I awaken one morning in the gutter, painfully sober after a three-day binge, and I resolve to change my ways and pursue virtue. In your opinion, how long would it make me to become a virtuous person? Could I become virtuous in an hour? A week? A month? Ever?
Your response should be at least one page in length.
4. Suppose Dan is dying from an unknown disease. He is wealthy and will give half of his money to anyone who can save his life. Joe, not know.
1. Paper should be 5-pages min. + 1 page works cited2. Should have.docxvannagoforth
1. Paper should be 5-pages min. + 1 page works cited
2. Should have at least 10 annotated sources (copy article onto word, highlight main point, write a few sentences about how it'll help you in writing the paper at the bottom of page)
3
. Should have an INTRO, NARRATION, ARGUMENTS, REFUTATION, CONCUSION
4. Use in-text citations and have organized mla format works cited page
SAMPLE OUTLINE
Research Paper Outline
Title: Rebellious Libya
Thesis: The United States should not get involved with Libya’s conflicts.
I.
Introduction:
A.
Start with the question, what is war? Explain briefly.
B.
Talk about the wars of the United States.
C.
What were the outcomes of some of those wars?
II.
Narration:
A.
Give some background on Libya.
B.
Explain how Col. Muammar Gaddafi became the leader of Libya
C.
Talk about why the citizens of Libya want to overthrow Gaddafi.
D.
Explain why the people feel that the United States should get involved in Libya’s conflicts.
III.
Partition:
A.
Thesis: I believe that the United States should not get involve with Libya’s conflicts.
B.
Essay Map.
1.
Cost of war.
2.
Using money in other Departments other defense.
3.
Killing innocent civilians and soldiers.
4.
Helping unknown rebels
5.
Involvement of foreign wars
IV.
Arguments:
A.
The cost of war is rising by the minute. The Obama Administration proposed a budget of $553 billion dollars for the department.
B.
Instead of spending all that money on war, we should be investing that money on health care and education.
C.
This conflict has caused the lives of many innocent civilians. NATO openly admitted to have killed innocent civilians, due to misguidance.
D.
The rebels fighting against Gaddafi are in need of military supplies. I don’t think that it is a good idea to help unknown rebels. We helped the Afghanistan rebels when they were fighting Russia. After they were victorious, they later became the “Taliban” and used those weapons to attack the US.
E.
Getting involved in foreign wars is not a good idea. The US has been involved in many foreign wars lately. These wars have been in foreign countries where Islam is the prominent religion. Libya is one of these countries. The involvement of the US in these places, builds a bad reputation worldwide and among the Muslim community.
V.
Refutation:
A.
Gaddafi’s actions against the civilians of Libya are totally wrong. Killing your own people is bad and therefore, we should help the rebels overthrow him.
B.
Gaddafi has been in power for many years. In fact, he holds the record for most years in power in a single country. This type of power can potentially lead to corruption and mistreatment of civilians.
C.
The people of Libya deserve to have democracy. They should have the right to elect their own leader.
D.
If Al Qaeda is threatening NATO and Libyan mercenaries then we should help them fight terrorism.
VI.
Conclusion:
A.
Summarize my arguments.
B.
State why we should not get involve with Libya’s conf.
1. Name and describe the three steps of the looking-glass self.2.docxvannagoforth
1. Name and describe the three steps of the 'looking-glass self'.
2. List and describe the three stages in George Mead's model of human development.
3. Piaget developed a four-stage process to explain how children develop reasoning skills. List each and give an example of one of the stages.
4. Briefly summarize the three elements of Freud's theory of personality and explain why sociologist have negative reactions to his analysis.
5. How does the mass media reinforce society's expectations of gender?
.
1. Provide an example of a business or specific person(s) that effec.docxvannagoforth
1. Provide an example of a business or specific person(s) that effectively use social media. What tools does the business or person use? How do they apply the tools effectively? Describe areas of improvement.
This assignment has to be 4 pages long, then it needs a cover page and reference page however that can not be a part of the four pages. So it would be 6 pages if you count the cover page and reference page!
.
1. Mexico and Guatemala. Research the political and economic situati.docxvannagoforth
1. Mexico and Guatemala. Research the political and economic situation of these countries and write about their peculiar circumstances.
2. Honduras, El Salvador and Panama. Research the political and economic situation of these countries and write about their peculiar circumstances.
3. Costa Rica and Nicaragua. Research the ecological and political situation of these countries and write about their peculiar circumstances.
4. Colombia and Ecuador. Research about the truths and myths about this two countries and write about your impressions on these stereotypes.
.
1. Many scholars have set some standards to judge a system for taxat.docxvannagoforth
1. Many scholars have set some standards to judge a system for taxation for its validity. How can you decide if a tax is good or bad?
You can consider these five following principles for your Discussion. What do these issues mean? How do you think they matter?
Adequacy Equity Exportability Neutrality Simplicity
What other tax revenue systems could you consider? How do you think they would be better or worse?
2. What role do taxes play in political issues?
3. What is your opinion of a flat tax as some politicians have proposed?
.
1. List and (in 1-2 sentences) describe the 4 interlocking factors t.docxvannagoforth
1. List and (in 1-2 sentences) describe the 4 interlocking factors that led to the ourbreak of world war 1
2. Explain the difference between and authoritarian regime and a totalitarian regime.
3. List and (in 1-2 sentences) describe the 5 factors that led to the ourbreak of world war 2.
.
1. Please explain how the Constitution provides for a system of sepa.docxvannagoforth
1. Please explain how the Constitution provides for a system of separation of powers and checks and balances. Provide a fully developed essay of at least 500 words, and cite sources used.
2. Describe how a bill becomes a law at the national level, in a fully developed essay of at least 500 words. Support your work with cited sources, references to Lecture Notes, or URLs where you obtained your information.
.
1. Please watch the following The Diving Bell & The Butterfly, Amel.docxvannagoforth
1. Please watch the following: The Diving Bell & The Butterfly, Amelie, The Lookout, A Single Man, Her, Little Children, and An Education and
Please respond to the films. In particular, respond to how the film develops the identity of a single character for an audience, and which you responded to (either the characters themselves or the way the film constructed the character) the most, or the least please , 10 sentence min and no plagiariasm also it has to be
followowed exactly whats written here.
PS: please dont waste my time if you will do a messy assigment, just dont send me a msg.
.
1. Most sociologists interpret social life from one of the three maj.docxvannagoforth
1. Most sociologists interpret social life from one of the three major theoretical frameworks/perspectives (conflict theory, functionalism, symbolic interactionism). Describe the major points of each one. List at least one sociologist who has been identified with each of these three theories.
2. What is the difference between basic sociology and applied sociology?
3. List and describe the eight steps of the scientific research model.
4. Discuss the importance of ethics in social research. Define what is meant by ethics.
.
1. Members of one species cannot successfully interbreed and produc.docxvannagoforth
1. Members of one species cannot successfully interbreed and produce fertile offspring with members of other species. This idea is known as
a. reproductive success.
b. punctuated evolution.
c. adaptive radiation.
d. the biological species concept.
e. geographic isolation.
2. The origin of new species, the extinction of species, and the evolution of major new features of living things are all changes that result from
a. macroevolution.
b. fitness.
c. speciation.
d. the biological species concept.
e. convergent evolution.
3. Which is a barrier that can contribute to reproductive isolation?
a. timing
b. behavior
c. habitat
d. incompatible reproductive structures
e. all of the above
4. Which of the following statements is false?
a. Horses and donkeys are separate species.
b. Two mules can mate and produce fertile offspring.
c. A horse and a donkey can mate and produce offspring.
d. Two donkeys can mate and produce fertile offspring.
e. Two horses can mate and produce fertile offspring.
5. The evolution of the penguin’s wing from a wing suited for flying to a “flipper-wing” used for swimming is an example of
a. refinement of existing adaptations.
b. reproductive isolation.
c. adaptation of existing structures to new functions.
d. inheritance of acquired characteristics.
e. the biological species concept.
6. Which of the following have been preserved as fossils?
a. dinosaur footprints
b. insects preserved in amber
c. petrified plant remains
d. animal bones
e. all of the above
7. The mass extinctions that included the dinosaurs took place during which period?
a. Cambrian (543–510 million years ago)
b. Devonian (409–363 million years ago)
c. Carboniferous (363–290 million years ago)
d. Jurassic (206–144 million years ago)
e. Cretaceous (144–65 million years ago)
8. The development of the complex, camera-like eye of a mammal is an example of
a. refinement of existing adaptations.
b. reproductive isolation.
c. adaptation of existing structures to new functions.
d. inheritance of acquired characteristics.
e. the biological species concept.
9. Which of the following statements is true?
a. Carbon-14 dating is useful for studying the age of early dinosaur fossils.
b. Carbon-14 has a half-life of 5,730 years.
c. Uranium-238 has a very short half-life.
d. Uranium-238 is present in all organisms.
e. Carbon-12 is not found in living plants.
10. Which of the following provides the best explanation for why Australia has so many organisms unique to that continent?
a. punctuated equilibrium
b. the biological species concept
c. convergent evolution
d. continental drift
e. cladistics
11. Scientists think that a meteor that fell in ____________________ may have led to the extinction of the dinosaurs.
a. Australia
b. the Yucatán peninsula
c. The Galápagos Islands
d. Pangaea
e. India
12. The great diversit.
1. Of the three chemical bonds discussed in class, which of them is .docxvannagoforth
1. Of the three chemical bonds discussed in class, which of them is simultaneously the weakest and most important for life on this planet as we know it?
2.Carbohydrates are very important sources of energy for life. Plants and arthropods also use carbohydrates as components of structures that are very important for their existence. Provide the names of the two most important carbohydrate based structures (one for plants and one for arthropods) and the carbohydrate components that are used to form them.
3._____________ _____________ are joined by ______________ bonds to form proteins.
4.Proteins can be used for several functions. Provide examples of structural and metabolic functions of proteins.
5.Describe the phosholipid bilayer of the plasma membrane. Why is this bilayer important for the formation of cells and the sequestration of chemical reactions within the cell?
.
1. Look at your diagrams for hydrogen, lithium, and sodium. What do .docxvannagoforth
1. Look at your diagrams for hydrogen, lithium, and sodium. What do they all have in common? What group are these elements in on the periodic table?
2. Look at your diagrams for fluorine and chlorine. What do they have in common?
Picture is in the link. Put answers on the word document and re-submit
.
1. Name the following molecules2. Sketch the following molecules.docxvannagoforth
1. Name the following molecules:
2. Sketch the following molecules:
3-cyclohexenone
4-ethyl 2,2,5-trimethyl 3-hexanone
ethyl butyrate
pentanoic acid
2-chloro 4-methyl 2,5-heptadienal
3,4-dichloro 4-ethyl octanal
p-chloro phenol
3-bromo 2-chloro 4-methyl hexane
3-cyclopropyl 1,2-cyclopentanediol
methyl phenyl ether
3,5-dimethyl 2-heptene-4,5-diol
3. Give two different uses for ethanol.
4. Name two categories of organic compounds (alkanes, aldehydes…) that have very strong characteristic odours.
.
1. List the horizontal and vertical levels of systems that exist in .docxvannagoforth
1. List the horizontal and vertical levels of systems that exist in organizations.
2.
Describe at least five steps involved in systems integration
3.
What is the role of ERP systems in system integration?
4. Why do you think functional silos are not appropriate for today's organization? Discuss your answer from organizational and technical perspectives.
5. Pick an organization that you know of or where you are/were working and provide examples of logical and physical integration issues that were faced by the organization when they broke the functional silos and moved to integrated systems.
.
1. Kemal Ataturk carried out policies that distanced the new Turkish.docxvannagoforth
1. Kemal Ataturk carried out policies that distanced the new Turkish republic of the 1920s from the Ottoman past. Why? What specific policies did Ataturk pursue? 2. Why many Arabs felt betrayed by the British (and the French) after the First World War? 3. Discuss at least three features of patrimonial leadership. List three or more Middle Eastern states where such type of political leadership persists 4. Describe the key processes (both internal and external) that initiated political and economic disintegration of the Ottoman Empire in the nineteenth century. 5. European military superiority in the late eighteenth century prompted Ottoman rulers to respond with what specific political measures? 6. The Zionist political movement originated in Europe rather than in the Middle East. Explain why and how. 7. After the Second World War, several Arab countries went through the process of transition from constitutional monarchies to republics. Identify three such countries and describe the course of events that brought about this transition. 8. How is religious Zionism different from secular Zionism? What is the relevance of this difference for the creation of the state of Israel? Has the relative influence of the two remained stable since the creation of the Israeli state? 9. What was the principle source of political legitimacy of the Ottoman Empire? 10. While most Ottoman European provinces, riding the tide of the nineteenth century nationalism, sought and won independence from Istanbul, Ottoman Arab provinces maintained their political loyalty to the Ottomans. What explains this difference between Arab and European provinces? 11. Social and political forces in favor of a constitutional reform in Iran (1905-1911) were markedly different from the groups that promoted constitutional limitations on executive powers of the sultan in the Ottoman Empire prior to the First World War? Explain this difference. 12. What are some of the key features of Arab socialisms? Which Arab leaders adopted socialist ideology? Which Arab leaders were opposed to it? 13. After the First World War, the new Middle Eastern protectorates (e.g., Syria, Lebanon, Iraq) were expected to develop into modern secular states. What specific policies did France and Britain try to implement? How successful have theses policies been? 14. The 1967 war was a watershed event for all major actors in the Middle East. Explain the consequences of the war for domestic politics in Israel and Egypt respectively.
.
1. If we consider a gallon of gas as having 100 units of energy, and.docxvannagoforth
1. If we consider a gallon of gas as having 100 units of energy, and 25 of those units are used to move the car, what law of thermodynamics accounts for the other 75 units of energy? (Points : 2)
the first law
the second law
2. Which of these is not a component of a molecule of adenosine triphosphate (ATP)? (Points : 3)
adenosine
phosphate
deoxyribose sugar
ribose sugar
3. Glycolysis is a sequence of ______ chemical reactions. (Points : 3)
nine
six
five
ten
4. Exergonic reactions produce products with a ___ energy level than that of the initial reactants. (Points : 3)
lower
higher
the same
5. When chemical X is reduced, which of these expressions would be an accurate representation of its reduced state? (Points : 3)
XO
XH
X
HX
6. Most enzymes are which kind of organic compound? (Points : 3)
carbohydrates
lipids
proteins
none of the above
7. The area on an enzyme where the substrate attaches is called the: (Points : 3)
active site
allosteric site
anabolic site
inactive site
8. Which of the following creatures would not be an autotroph? (Points : 3)
cactus
cyanobacteria
fish
palm tree
9. The process by which most of the world's autotrophs make their food is known as: (Points : 3)
glycolysis
photosynthesis
chemosynthesis
herbivory
10. Plants are the only organisms that use ATP for the transfer and storage of energy. (Points : 2)
True
False
11. The colors of light in the visible range (from longest wavelength to shortest) are: (Points : 3)
ROYGBIV
VIBGYOR
GRBIYV
ROYROGERS
12. Chlorophyll is a green pigment because it absorbs only the green part of the visible light spectrum. (Points : 2)
True
False
13. The photosynthetic pigment that is essential for the process to occur is: (Points : 3)
chlorophyll a
chlorophyll b
beta carotene
xanthocyanin
14. A photosystem is: (Points : 3)
a collection of hydrogen-pumping proteins
a series of electron-accepting proteins arranged in the thylakoid membrane
a collection of photosynthetic pigments arranged in a thylakoid membrane
found only in prokaryotic organisms
15. Which of these molecules is NOT a product of the Electron Transport System? (Points : 3)
ATP
Water
Pyruvate
NAD+
16. The dark reactions require all of these chemicals to proceed except: (Points : 3)
ATP
NADPH
carbon dioxide
oxygen
17. The structural unit of photosynthesis, where the photosystems are located, are called: (Points : 3)
chlorophylls
eukaryotes
stroma
thylakoids
18. Which of the following does NOT occur during the light independent process? (Points : 3)
CO2 is used to form carbohydrates
NADPH converts to NADP
ADP converts to ATP
ATP converts to ADP
19. The production of ATP that occurs in the presence of oxygen is called: (Points : 3)
aerobic respiration
anaerobic respiration
chemiosmosis
photosynthesis
20. The first stable chemical formed by the Calvin Cycle is: (Points :.
1. In 200-250 words, analyze the basic issues of human biology as th.docxvannagoforth
1. In 200-250 words, analyze the basic issues of human biology as they relate to chronic conditions and describe the interaction between disability, disease, and behavior. Examine and discuss the impact of biological health or illness on social, psychological, and physical problems from the micro, mezzo, and macro perspectives. Choose a chronic condition from those provided in your text and consider how you might feel, think, and behave differently if the condition were affecting you versus if the condition were affecting a stranger. How might you think differently about this chronic condition if it were affecting someone close to you, your neighbor, or someone in your community? Please include at least two supporting scholarly resources.
2.Our stage of life, intellectual/cognitive abilities, and sociocultural position in life, affect our perspectives and resultant behaviors about a number of conditions including cancer. Consider the information provided in the
“Introduction to the Miller Family”
document. Both Ella and Elías have been diagnosed with cancer. Ella has been fighting cancer with complementary and alternative methods with some success for many years. Elías, her grandson, is 10 years old and has recently been diagnosed with leukemia but has not yet begun treatment. Putting yourself in either Ella or Elías’s place, what might your perspective on your cancer be? Integrate how the stage of life, cognitive abilities, and sociocultural position of your chosen person impacts her/his perspective on his/her individual disease.
.
The French Revolution, which began in 1789, was a period of radical social and political upheaval in France. It marked the decline of absolute monarchies, the rise of secular and democratic republics, and the eventual rise of Napoleon Bonaparte. This revolutionary period is crucial in understanding the transition from feudalism to modernity in Europe.
For more information, visit-www.vavaclasses.com
The Art Pastor's Guide to Sabbath | Steve ThomasonSteve Thomason
What is the purpose of the Sabbath Law in the Torah. It is interesting to compare how the context of the law shifts from Exodus to Deuteronomy. Who gets to rest, and why?
How to Split Bills in the Odoo 17 POS ModuleCeline George
Bills have a main role in point of sale procedure. It will help to track sales, handling payments and giving receipts to customers. Bill splitting also has an important role in POS. For example, If some friends come together for dinner and if they want to divide the bill then it is possible by POS bill splitting. This slide will show how to split bills in odoo 17 POS.
This is a presentation by Dada Robert in a Your Skill Boost masterclass organised by the Excellence Foundation for South Sudan (EFSS) on Saturday, the 25th and Sunday, the 26th of May 2024.
He discussed the concept of quality improvement, emphasizing its applicability to various aspects of life, including personal, project, and program improvements. He defined quality as doing the right thing at the right time in the right way to achieve the best possible results and discussed the concept of the "gap" between what we know and what we do, and how this gap represents the areas we need to improve. He explained the scientific approach to quality improvement, which involves systematic performance analysis, testing and learning, and implementing change ideas. He also highlighted the importance of client focus and a team approach to quality improvement.
Students, digital devices and success - Andreas Schleicher - 27 May 2024..pptxEduSkills OECD
Andreas Schleicher presents at the OECD webinar ‘Digital devices in schools: detrimental distraction or secret to success?’ on 27 May 2024. The presentation was based on findings from PISA 2022 results and the webinar helped launch the PISA in Focus ‘Managing screen time: How to protect and equip students against distraction’ https://www.oecd-ilibrary.org/education/managing-screen-time_7c225af4-en and the OECD Education Policy Perspective ‘Students, digital devices and success’ can be found here - https://oe.cd/il/5yV
We all have good and bad thoughts from time to time and situation to situation. We are bombarded daily with spiraling thoughts(both negative and positive) creating all-consuming feel , making us difficult to manage with associated suffering. Good thoughts are like our Mob Signal (Positive thought) amidst noise(negative thought) in the atmosphere. Negative thoughts like noise outweigh positive thoughts. These thoughts often create unwanted confusion, trouble, stress and frustration in our mind as well as chaos in our physical world. Negative thoughts are also known as “distorted thinking”.
Read| The latest issue of The Challenger is here! We are thrilled to announce that our school paper has qualified for the NATIONAL SCHOOLS PRESS CONFERENCE (NSPC) 2024. Thank you for your unwavering support and trust. Dive into the stories that made us stand out!
Original StudyType of Breast Cancer Diagnosis, Screening,a.docx
1. Original Study
Type of Breast Cancer Diagnosis, Screening,
and Survival
Carla Cedolini,1 Serena Bertozzi,1 Ambrogio P. Londero,2
Sergio Bernardi,3,4
Luca Seriau,1 Serena Concina,1 Federico Cattin,1 Andrea
Risaliti1
Abstract
Organized, invitational breast cancer screening in our
population succeeded in detecting early-stage tumors,
which have been consequently treated more frequently with
breast and axillary conservative surgery, com-
plementary breast irradiation, and eventual hormonal therapy.
The diagnosis of invasive cancer with screening
in our population resulted in a survival gain at 5 years from the
diagnosis.
Introduction: Breast cancer screening is known to reduce
mortality. In the present study, we analyzed the prevalence
of breast cancers detected through screening, before and after
introduction of an organized screening, and we
evaluated the overall survival of these patients in comparison
with women with an extrascreening imaging-detected
breast cancer or those with palpable breast cancers. Materials
and Methods: We collected data about all women
who underwent a breast operation for cancer in our department
between 2001 and 2008, focusing on type of tumor
diagnosis, tumor characteristics, therapies administered, and
patient outcome in terms of overall survival, and re-
currences. Data was analyzed by R (version 2.15.2), and P < .05
2. was considered significant. Results: Among the 2070
cases of invasive breast cancer we considered, 157 were
detected by regional mammographic screening (group A),
843 by extrascreening breast imaging (group B: 507 by
mammography and 336 by ultrasound), and 1070 by extra-
screening breast objective examination (group C). The 5-year
overall survival in groups A, B, and C were, respectively,
99% (95% CI, 98%-100%), 98% (95% CI, 97%-99%), and 91%
(95% CI, 90%-93%), with a significant difference
between the first 2 groups and the third (P < .05) and a trend
between groups A and B (P ¼ .081). Conclusion: The
diagnosis of invasive breast cancer with screening in our
population resulted in a survival gain at 5 years from the
diagnosis, but a longer follow-up is necessary to confirm this
data.
Clinical Breast Cancer, Vol. 14, No. 4, 235-40 ª 2014 Elsevier
Inc. All rights reserved.
Keywords: Breast cancer, Breast cancer screening, Invasive
breast cancer, Mammographic screening, Overall survival
Introduction
Because of the detection of early-stage tumors, breast cancer
screening reduced breast cancer mortality in Europe by 25%-
31%
in patients who were invited for screening and by 38%-48% in
those who were actually screened during the last decade of the
twentieth century and the first decade of the twenty-first.1 In
our
region of Italy, an organized breast cancer screening was firstly
intro-
duced in 2005, but despite the high compliance of invited
women
1Clinic of Surgery
2Clinic of Obstetrics and Gynecology
University of Udine, Udine, Italy
3. 3Department of Surgery, Ospedale Civile di Latisana, Udine,
Italy
4Department of Surgery, AOU “Santa Maria della
Misericordia,” Udine, Italy
Submitted: Feb 17, 2013; Revised: Jan 23, 2014; Accepted: Feb
12, 2014; Epub:
Feb 20, 2014
Address for correspondence: Dr Carla Cedolini, Clinic of
Surgery, University of Udine,
Italy p.le SSMM Misericordia 15, 33100 Udine, Italy
E-mail contact: [email protected]
1526-8209/$ - see frontmatter ª 2014 Elsevier Inc. All rights
reserved.
http://dx.doi.org/10.1016/j.clbc.2014.02.004
(which progressively increased after the screening
introduction),
a high prevalence still exists of women who have their breast
cancer
diagnosed by extrascreening objective examination or
imaging.2,3
In the present study, analyzed, among breast cancer patients
treated in our department, the prevalence of breast cancers
detected
through the invitational screening, and the overall survival of
these
patients in comparison with that of women with an
extrascreening
imaging-detected breast cancer or those with palpable breast
cancers.
Materials and Methods
We collected retrospective data for about 2811 women who
4. underwent a breast operation following breast cancer diagnosis
or
suspicion in our clinic between January 2001 and April 2008, in
order to have a follow-up of � 5 years for every patient. Then,
we
excluded women with a diagnosis of benign lesion (471
patients),
intralobular neoplasia (22 patients), or intraductal neoplasia
(248
patients). Intraductal neoplasia represented the 17.6% of screen-
detected and the 14.4% of extrascreening imaging-detected
breast
Clinical Breast Cancer August 2014 - 235
mailto:[email protected]
http://dx.doi.org/10.1016/j.clbc.2014.02.004
Table 1 Description of the Population in the Different Groups
Characteristic
Method of Cancer Detection
PScreening Imaging Palpable Lesion
Age, years (SD) 61.6 (�5.77) 60.01 (�11.25) 61.2 (�15.14)
.104
BMI, kg/m2 (SD) 27.47 (�5.55) 25.84 (�4.76) 25.49 (�4.8)
<.05
Patients, % (no./total) Patients, % (no./total) Patients, %
(no./total)
Tobacco smokera 7.9 (12/151) 4.7 (32/685) 5.7 (49/858) .256
6. Radiotherapy 76.3 (119/156) 63.6 (510/802) 48.9 (496/1015)
<.05
Chemotherapy 26.3 (41/156) 36.3 (290/799) 51.1 (518/1013)
<.05
Hormonal therapy 85.3 (133/156) 83.3 (663/796) 73.2
(742/1013) <.05
Abbreviations: BMI ¼ body mass index; CALND ¼ complete
axillary lymph node dissection; SLNB ¼ sentinel lymph node
biopsy.
aSample size varies because of incomplete data.
bSample size varies because only conservative treatment were
eventually treated by a second procedure.
Breast Cancer Screening and Survival
236 -
lesions, while it accounted for only the 2.5% of palpable
lesions;
therefore, we decided to exclude it from data analysis because
of its
better prognosis and its consequently probable influence on the
survival analysis. In fact, it is well-known that the screening
benefit
of mortality reduction is accompanied by the harm of
overdiagnosis,
defined as the detection at screening of a cancer that would not
have
otherwise become clinically evident in the woman’s lifetime.4,5
Finally, the study population included 2070 women affected by
invasive breast cancer.
Collected data included the following patients characteristics:
7. age
at diagnosis, body mass index (BMI), familial history of breast
cancer, fertility status, eventual use of estroprogestinic
therapies.
Tumor characteristics were considered as follows: histological
type,
TNM classification and stage, nuclear grading, Mib1/Ki-67
prolif-
eration index, hormone receptors status including estrogen
receptor
(ER), progesteron receptor (PR) and Her2/neu expression,
eventual
involvement of extraaxillary lymph nodes (internal mammary
chain
or subclavear ones), and other microscopic features evaluated in
the
new classification by Veronesi et al.6 such as multifocality,
extensive
intraductal component, perivascular invasion, peritumoral
inflam-
mation, lymph node extracapsular invasion or blanched lymph
nodes. Moreover, the therapeutic management was investigated,
including conservative versus radical, breast and axillary
surgery,
Clinical Breast Cancer August 2014
eventual neoadjuvant therapies, adjuvant breast irradiation,
endo-
crine or chemotherapy administered.
Then, the study population was divided into 3 groups as
follows:
group A) screen-detected breast cancers (including lesions
detected
by mammography, ultrasound or breast objective examination
within the biyearly, organized, regional screening program);
group B)
8. extrascreening imaging-detected breast cancers (including
lesions
detected by mammography or ultrasound, which the women un-
derwent spontaneously, for example in case of familial history
of
breast cancer out from the age range of the screening, or yearly
within
the interval between 2 screening invitations, or even simply for
personal choice); group C) cancers detected by extrascreening
breast
objective examination (including palpable mass, cutis
retraction,
breast ulceration, nipple discharge, and mastitis carcinomatosa).
Data was analyzed by R (version 2.15.2), considering
significant
P < .05. Monovariate analysis was performed by 1-way Anova
or t
test in case of continuous variables, chi-square test or Fisher
exact
test in case of categorical variables. Some data are presented as
proportions with relative 95% confidence interval where appro-
priate. Overall survival was considered to be the main outcome,
and
Kaplan-Meyer curve was drown to compare the overall survival
among the 3 groups. Moreover, also the incidence of
locoregional
and distant recurrences was compared among the 3 groups.
Table 2 TNM Staging and Grading in the Different Groups
Screening Imaging Palpable Lesion
PPatients, % (no./total) Patients, % (no./total) Patients, %
10. G3 21.7 (34/157) 19.4 (161/828) 35.4 (362/1023) <.05
Abbreviation: TNM ¼ tumor, node, metastases.
aSample size varies because of incomplete data.
Carla Cedolini et al
Results
Among 2070 considered invasive breast cancers operated in our
Clinic between January 2001 and April 2008, 247 were detected
by
the regional, organized, mammographic screening (group A),
1176
by extrascreening breast imaging (group B: 768 by
mammography
and 408 by ultrasound), and 1393 by extrascreening breast
objective
examination (group C). Interventions made in patients with
breast
cancer diagnosed through screening began in 2006. Before and
after
screening introduction the number of operations for invasive
breast
cancer has not changed (respectively 21.6 vs. 21.5
interventions/
month). After the introduction of screening 20% of invasive
cancers
were diagnosed by screening and significantly decreased the
preva-
lence of cancers diagnosed by physical examination of the
breast
(56.0% antescreening vs. 44.5% postscreening period, P < .05).
If we compare patients characteristics in the 3 groups [Table 1],
despite the similar mean age at diagnosis (about 61 years old),
women in their fertile age were more frequently diagnosed to
11. have a
breast cancer by extrascreening objective examination (24.3%)
than
by breast screening (2.1%) or extrascreening breast imaging
(16.2%). And, considering that breast screening in our region is
offered to women between 50 and 69 years of age, it does not
surprise that almost the totality of screen-detected breast
cancers
(97.9%) is diagnosed after menopause.
Taking into consideration the surgical treatment, the majority
of screen-detected breast cancers were treated with breast
conser-
vative surgery (77.1% excluding 15.9% of primary
mastectomies
and 7.0% of radicalization mastectomies) and sentinel lymph
node
biopsy (65.6%). Women of group B and C underwent only
breast
conservative surgery in the 63.2% and 38.9% of cases
respectively,
and sentinel lymph node biopsy in the 47.1% and 15.0% of
cases
respectively, and these prevalence resulted significantly
different
among the 3 groups (P < .05).
For what concerns nonsurgical treatments, group C has a
significantly higher prevalence of both neoadjuvant therapy
(16.0%,
P < .05) and adjuvant chemotherapy (51.1%, P < .05), probably
due to the significantly higher prevalence of advanced stage at
diagnosis (stage III in the 25.0% of cases and stage IV in the
3.2%,
P < .05) [Table 2], and a significantly lower prevalence of
hormonal
12. therapy (73.2%, P < .05), which correlates with the higher prev-
alence of triple-negative cancers (Basal-like 14.9%, P < .05)
[Table 3]. On the other hand, group A and B were more likely to
receive breast irradiation after conservative surgery and
adjuvant
hormonal therapy when appropriate.
No significant difference was there among the 3 groups about
the
histological type, but in group C there was a significantly
higher
prevalence of tumor characteristics that are commonly
recognized to
negatively influence breast cancer prognosis [Table 2 and 3],
such as
greater tumor size (T3 and T4 respectively 2.6% and 7.9%, P <
.05),
greater lymph node involvement (N2 and N3 9% each, P < .05)
higher nuclear grading (G3 35.4%, P < .05), higher Mib1/Ki-67
proliferation index (> 20% in the 49.7% of cases, P < .05), pres-
ence of multifocality/multicentricity (19.6%, P < .05),
lymphovas-
cular invasion (16.9%, P < .05) and peritumoral inflammation
(7.0%, P < .05), luminal B (41.3%, P < .05), luminal Her
(11.1%,
P < .05), basal-like (14.9%, P < .05) and Her2-enriched (8.2%,
P < .05) molecular subtypes, extracapsular invasion of lymph
node
metastasis (12.4%, P < .05) and blanched lymph nodes (6.2%,
P < .05).
Clinical Breast Cancer August 2014 - 237
Table 3 Tumor Characteristics in the Different Groups
15. Local recurrences during follow-up 1.3 (2/157) 3.6 (30/843) 9.3
(99/1070) <.05
Distant metastases during follow-upa 1.3 (2/157) 5.1 (43/841)
13.4 (142/1059) <.05
Abbreviations: ER ¼ estrogen receptor; HER ¼ human
epidermal growth factor receptor; PR ¼ progesterone receptor.
aSample size varies because of incomplete data.
Breast Cancer Screening and Survival
238 -
Locoregional and distant recurrences were significantly more
prevalent (P < .05) in group C (respectively 9.3% and 13.4%)
than
in group A (respectively 1.3% and 1.3%) and B (respectively
3.6%
and 5.1%) [Table 3].
The 5-years overall survival in group A, B and C resulted
respectively 99% (95% CI, 98%-100%), 98% (95% CI, 97%-
99%), and 91% (95% CI, 90%-93%), with a significant
difference
among the 3 groups (P < .05) [Fig. 1A], even considering only
patients operated after screening introduction [Fig. 1B]. In
partic-
ular comparing group to group overall survival had a significant
difference among the first 2 groups and the third (A or B vs. C)
(P < .05) and a trend between group A and B (A vs. B)(P ¼
.081).
Discussion
Breast cancer screening in our population succeeded in
detecting
16. early-stage tumors with favorable tumor characteristics, which
have
been consequently treated more frequently with breast and
axillary
conservative surgery, complementary breast irradiation and
eventual
hormonal therapy. Women with a screen-detected breast cancer
had
Clinical Breast Cancer August 2014
a significantly higher 5-years overall survival than women who
had
their breast cancer diagnosed by extrascreening objective
examina-
tion or imaging, as well as a significantly lower prevalence of
locoregional and distant recurrences.
In accordance with the most published studies about this
argument, our findings confirm the association of screening
with
both smaller tumor size and less lymph node metastases at pre-
sentation,7,8 and support a survival improvement of breast
cancer
patients after breast screening introduction.1,8-19
However, there is much skepticism about the effective role of
mammographic screening on breast cancer mortality. In fact, it
is
very difficult to determine how much of the observed reduction
in
mortality can be attributed exclusively to the screening, rather
than
to improved breast cancer management or to changes in risk fac-
tors.20-26 In addiction, it is still debated whether the estimated
effect
of routine mammography on breast cancer mortality is thus
highly
17. dependent on study design.27-29
Moreover, a great number of women in our population under-
went regular breast imaging controls out from the screening
program,
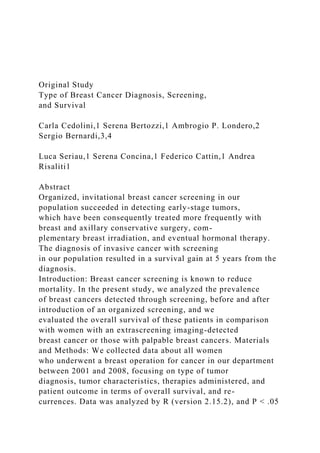
Figure 1 Overall Survival in the 3 Groups: A) Considering The
Whole Study Population; B) Considering Only Breast Cancers
Diagnosed Since the Screening Introduction
0 1 2 3 4 5 6
70%
80%
90%
100%
Follow-up time, y
Follow-up time, y
O
ve
ra
ll
su
rv
iv
19. B
Carla Cedolini et al
and the earlier detection of breast cancer in these cases may be
explained just by the increased women awareness about this
topic.
Furthermore, it is not possible to exclude that, even if the
screening would have diagnosed group C cancers, their
unfavorable
biologic behavior would have anyway correlated with a worse
prognosis. In this perspective, an analysis of interval cancers
would
be more helpful, defined as breast cancers that occur in the
age-specific screening population during the interval between 2
consequent screening invitations.30 In fact, interval cancers
repre-
sent a group of very biologically aggressive tumors with a rapid
grow
and worse prognostic factors, and their incidence may be a good
indicator of screening effectiveness.
The weakness of this study lays in its retrospective design and
the
limited number of patients if compared with other multicentric
international studies.
Conclusion
In conclusion, breast cancer screening in our population
resulted
in a significant survival gain at 5 years from the diagnosis, but
a
longer follow up should be necessary to confirm this data, and
further
studies are required in order to evaluate interval cancers in
20. order to
better assess breast screening effectiveness in our population.
Clinical Practice Points
� Organized, invitational breast cancer screening significantly
in-
creased the detection rate of early-stage tumors in our popula-
tion, and resulted in a survival gain at 5 years from the
diagnosis.
� Women who had their breast cancers diagnosed by both orga-
nized, invitational mammographic screening and extra-screening
breast imaging had a significantly higher 5-years overall
survival
rate than those who had their cancer diagnosed by breast
objective examination.
� Independently by the age group, regular breast imaging had
an
important impact on a prompt breast cancer diagnosis, and
consequently to its prognosis.
� Anyway, further studies are required in order to better
investigate
the characteristics of cancers diagnosed by objective
examination,
and especially interval cancers detected between two
consequent
screening calls.
Disclosure
The authors have stated that they have no conflicts of interest.
References
1. Broeders M, Moss S, Nyström L, et al. The impact of
mammographic screening on
21. breast cancer mortality in Europe: a review of observational
studies. J Med Screen
2012; 19(Suppl 1):14-25.
2. Driul L, Bernardi S, Bertozzi S, Schiavon M, Londero A,
Petri R. New surgical
trends in breast cancer treatment: conservative interventions and
oncoplastic breast
surgery. Minerva Ginecol 2013; 65:289-96.
3. Busolin A, Clagnan E, Franzo A, Tillati S, Zanier L. I
programmi di screening
oncologici in Friuli Venezia Giulia dal 1999 al 2010. Technical
report, Servizio
Epidemiologico - Direzione Centrale Salute, Integrazione
Sociosanitaria e Politiche
Sociali - Regione Friuli Venezia Giulia. 2011.
4. Bleyer A, Welch HG. Effect of three decades of screening
mammography on
breast-cancer incidence. N Engl J Med 2012; 367:1998-2005.
5. Independent UK Panel on Breast Cancer Screening. The
benefits and harms of
breast cancer screening: an independent review. Lancet 2012;
380:1778-86.
Clinical Breast Cancer August 2014 - 239
http://refhub.elsevier.com/S1526-8209(14)00029-9/sref1
http://refhub.elsevier.com/S1526-8209(14)00029-9/sref1
http://refhub.elsevier.com/S1526-8209(14)00029-9/sref1
http://refhub.elsevier.com/S1526-8209(14)00029-9/sref2
http://refhub.elsevier.com/S1526-8209(14)00029-9/sref2
http://refhub.elsevier.com/S1526-8209(14)00029-9/sref2
http://refhub.elsevier.com/S1526-8209(14)00029-9/sref3
22. http://refhub.elsevier.com/S1526-8209(14)00029-9/sref3
http://refhub.elsevier.com/S1526-8209(14)00029-9/sref4
http://refhub.elsevier.com/S1526-8209(14)00029-9/sref4
Breast Cancer Screening and Survival
240 -
6. Arnone P, Zurrida S, Viale G, Dellapasqua S, Montagna E,
Arnaboldi P, et al.
The TNM classification of breast cancer: need for change.
Updates Surg 2010;
62:75-81.
7. Nagtegaal ID, Duffy SW. Reduction in rate of node
metastases with breast
screening: consistency of association with tumor size. Breast
Cancer Res Treat 2013;
137:653-63.
8. Paci E, Duffy SW, Giorgi D, Zappa M, Crocetti E, Vezzosi
V, et al. Quantification
of the effect of mammographic screening on fatal breast
cancers: The Florence
Programme 1990-96. Br J Cancer 2002; 87:65-9.
9. Paci E, EUROSCREENWG. Summary of the evidence of
breast cancer service
screening outcomes in Europe and first estimate of the benefit
and harm balance
sheet. J Med Screen 2012; 19(Suppl 1):5-13.
10. Otto SJ, Fracheboud J, Verbeek ALM, et al. Mammography
screening and risk of
breast cancer death: a population-based case-control study.
Cancer Epidemiol
23. Biomarkers Prev 2012; 21:66-73.
11. Paap E, Holland R, den Heeten GJ, et al. A remarkable
reduction of breast cancer
deaths in screened versus unscreened women: a case-referent
study. Cancer Causes
Control 2010; 21:1569-73.
12. Puliti D, Miccinesi G, Collina N, et al. Effectiveness of
service screening: a case-
control study to assess breast cancer mortality reduction. Br J
Cancer 2008; 99:
423-7.
13. Roder D, Houssami N, Farshid G, et al. Population
screening and intensity of
screening are associated with reduced breast cancer mortality:
evidence of ef-
ficacy of mammography screening in Australia. Breast Cancer
Res Treat 2008;
108:409-16.
14. Allgood PC, Warwick J, Warren RML, Day NE, Duffy SW.
A case-control study
of the impact of the East Anglian breast screening programme
on breast cancer
mortality. Br J Cancer 2008; 98:206-9.
15. Gabe R, Tryggvadóttir L, Sigfússon BF, Olafsdóttir GH,
Sigurdsson K, Duffy SW.
A case-control study to estimate the impact of the Icelandic
population-based
mammography screening program on breast cancer death. Acta
Radiol 2007; 48:
948-55.
24. 16. Swedish Organised Service Screening Evaluation Group.
Reduction in breast
cancer mortality from organized service screening with
mammography: 1.
Further confirmation with extended data. Cancer Epidemiol
Biomarkers Prev
2006; 15:45-51.
Clinical Breast Cancer August 2014
17. Gorini G, Zappa M, Miccinesi G, Paci E, Costantini AS.
Breast cancer mortality
trends in two areas of the province of Florence, Italy, where
screening programmes
started in the 1970s and 1990s. Br J Cancer 2004; 90:1780-3.
18. Fielder HM, Warwick J, Brook D, et al. A case-control
study to estimate the
impact on breast cancer death of the breast screening
programme in Wales. J Med
Screen 2004; 11:194-8.
19. Tabár L, Vitak B, Chen HH, Yen MF, Duffy SW, Smith RA.
Beyond randomized
controlled trials: organized mammographic screening
substantially reduces breast
carcinoma mortality. Cancer 2001; 91:1724-31.
20. Autier P, Boniol M, Gavin A, Vatten LJ. Breast cancer
mortality in
neighbouring European countries with different levels of
screening but
similar access to treatment: trend analysis of WHO mortality
database. BMJ
2011; 343:d4411.
21. Berry DA, Cronin KA, Plevritis SK, et al. Effect of
screening and adjuvant therapy
25. on mortality from breast cancer. N Engl J Med 2005; 353:1784-
92.
22. Jones AL. Reduction in mortality from breast cancer. BMJ
2005; 330:205-6.
23. Kalager M, Zelen M, Langmark F, Adami HO. Effect of
screening mammography
on breast-cancer mortality in Norway. N Engl J Med 2010;
363:1203-10.
24. Autier P, Héry C, Haukka J, Boniol M, Byrnes G. Advanced
breast cancer
and breast cancer mortality in randomized controlled trials on
mammography
screening. J Clin Oncol 2009; 27:5919-23.
25. Esserman L, Shieh Y, Thompson I. Rethinking screening for
breast cancer and
prostate cancer. JAMA 2009; 302:1685-92.
26. Jørgensen KJ, Zahl PH, Gøtzsche PC. Breast cancer
mortality in organised
mammography screening in Denmark: comparative study. BMJ
2010; 340:c1241.
27. Olsen AH, Njor SH, Lynge E. Estimating the benefits of
mammography
screening: the impact of study design. Epidemiology 2007;
18:487-92.
28. Paap E, Verbeek ALM, Puliti D, Paci E, Broeders MJM.
Breast cancer screening
case-control study design: impact on breast cancer mortality.
Ann Oncol 2011; 22:
863-9.
26. 29. Demissie K, Mills OF, Rhoads GG. Empirical comparison of
the results of ran-
domized controlled trials and case-control studies in evaluating
the effectiveness of
screening mammography. J Clin Epidemiol 1998; 51:81-91.
30. Heidinger O, Batzler WU, Krieg V, et al. The incidence of
interval cancers in the
german mammography screening program: results from the
population-based
cancer registry in north rhine-westphalia. Dtsch Arztebl Int
2012; 109:781-7.
http://refhub.elsevier.com/S1526-8209(14)00029-9/sref5
http://refhub.elsevier.com/S1526-8209(14)00029-9/sref5
http://refhub.elsevier.com/S1526-8209(14)00029-9/sref5
http://refhub.elsevier.com/S1526-8209(14)00029-9/sref6
http://refhub.elsevier.com/S1526-8209(14)00029-9/sref6
http://refhub.elsevier.com/S1526-8209(14)00029-9/sref6
http://refhub.elsevier.com/S1526-8209(14)00029-9/sref7
http://refhub.elsevier.com/S1526-8209(14)00029-9/sref7
http://refhub.elsevier.com/S1526-8209(14)00029-9/sref7
http://refhub.elsevier.com/S1526-8209(14)00029-9/sref8
http://refhub.elsevier.com/S1526-8209(14)00029-9/sref8
http://refhub.elsevier.com/S1526-8209(14)00029-9/sref8
http://refhub.elsevier.com/S1526-8209(14)00029-9/sref9
http://refhub.elsevier.com/S1526-8209(14)00029-9/sref9
http://refhub.elsevier.com/S1526-8209(14)00029-9/sref9
http://refhub.elsevier.com/S1526-8209(14)00029-9/sref10
http://refhub.elsevier.com/S1526-8209(14)00029-9/sref10
http://refhub.elsevier.com/S1526-8209(14)00029-9/sref10
http://refhub.elsevier.com/S1526-8209(14)00029-9/sref11
http://refhub.elsevier.com/S1526-8209(14)00029-9/sref11
http://refhub.elsevier.com/S1526-8209(14)00029-9/sref11
http://refhub.elsevier.com/S1526-8209(14)00029-9/sref12
29. privately-owned company or a franchised organization. The
product that you have decided to sell is lemonade. To make the
endeavor work, you will have to define the product that you will
be selling (that is some marketable form of this drink) and
decide on a target market.
Your marketing team's mission is to prove the company’s goals
will be met by providing research, strategy development, and
reasoning why this form of this product is viable In this first
half of the project, you will report on the following:
· Target market
· Product's definition to the target marke
· Viable pricing strategy
· Brand's position in the competitive environmentComplete the
following
1. Select a company name and determine the real business world
industry of operation.
Company Name
Industry of Operation
LT3 (learnin team 3) Pro
Beverage
2. Describe in no more than 90 words the new and unique form
of lemonade that will be launced by your company.
The proposed drink will be made exclusively from lemons that
are produced from organic farms. The drink will be a non-
carbonated drink fused with the goodness of fresh lemons that
30. are grown in farms that do not employ any harmful chemicals or
fertilizers. Every produce is a true gift of the nature that will be
enjoyed by one and all. The fact that it is a non-carbonated
drink will also ensure that the drink is not as harmful as a Pepsi
or a Coke.
3. Complete the chart in a total of 90 words describing your
organization.
Who are they
Industry of Operation
Mission and Values
Differentiation from other organizations
For-profit organization made by a group of entrepreneurs who
believe in a healthy world.
Beverage Industry
To create nutritious drinks for the young population that
believes in leading a healthy lifestyle. To facilitate their ever
growing zeal to be fit, by offering value driven products in the
beverage space.
To offer a product that is a winner when it comes to being a
healthy drink. The drink will be made from organic farm
produce and will be non-carbonated drinks. Currently, there are
31. no major brands that fit that description.
Based on product type, lemonade has been classified into
alcoholic, non-alcoholic and powder mix. Also, in terms of
variety, the product can be segmented into cloudy lemonade,
pink lemonade and clear lemonade.
4. Identify the following in no more than 90 words regarding
your target market.
Composition of target market
Age- From 7 to 40 years
gender- Both Male and Female
Occupation- Students as well Job doers and professionals like
Teachers
Lifestyle- Customers who likes to love healthy lifestyle like go
to gym, do workouts etc
Segmentation criteria used in idenfitication
the segmentation Criteria used In targeting the market is
Demographic criteria and Psychographic Criteria.
Demographic segmentation is market segmentationaccording to
age, race, religion, gender, family size, ethnicity, income, and
education
Psychographic segmentation is the marketsegmentation strategy
in which the total market is divided on the basis of psychology,
personality of people, characteristics, lifestyle, attitudes etc.
5. Determine in no more than 90 words how you will define the
lemonade to your target market (include information on
packaging, labeling, etc.). How will this add value and
differentiate the brand and product from the competition while
encouraging the target market to buy?
32. Target Market Definition
Differentiation
Our lemonade will be Intensive Distribution. Making the
product available in as many locations as possible such as drive
through and vending locations around the Malls and outlets.
In store displays of a beverage being enjoyed by individuals of
different age groups, genders and race. The packaging will have
a Big image of the fruits and vegetables used to make the
beverage. This will allow for a healthier option presentation.
6. Complete the chart in a total of no more than 90 words to
compare your company with industry competitors.
Top Business Industry Competitors
Your Company’s Positioning
Lemon Leaf Café
We’re just like competitors X, only we’re Y. (showing that we
carry the same items only better)
Electric Lemonade
We’re the same as X, only cheaper and organic.
Lemonade
We combine the best traits of our competitors. Customer
satisfaction is not our goal, its our promise.
7. Define the pricing strategy in no more than 90 words that you
will use for the introduction of the product.
We would use Penetration pricing. The goal is to share our
product to as much of the community. This will allow us to
raise awareness of our new product and allow customers to
spread our product image through word of mouth.
8. Discuss in no more than 90 words the maturity life cycle
stages of your product.