This document summarizes information about anticoagulation therapy including oral anticoagulants like warfarin. It discusses their mechanism of action in inhibiting vitamin K and prolonging clotting time. It lists common indications for anticoagulant use such as atrial fibrillation or blood clots. The document outlines how prothrombin time is used to monitor effectiveness and provides target ranges for different prosthetic heart valves. It identifies drug and dietary interactions and contraindications to consider with anticoagulant therapy.

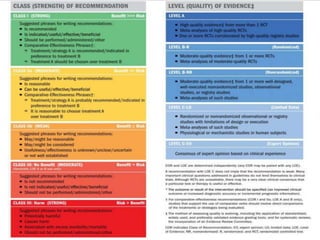
![TARGET INR FOR EACH VALVES (AHA CRITERIA)
[2017]
VALVE TARGET INR VKA ASPIRIN DURATION
•Anticoagulation with a
VKA and INR
monitoring is
recommended in
patients with a
mechanical prosthetic
valve
According to
COR – I,
LOE – A.
•Mechanical
valve(Bileaflet or Tilting
disc)AVR with no risk
for thrombo-embolism
2.5 + [I,B] + [I,A]
(75 – 100mg)
Life long
•Mech. AVR with risk
for thrombo-embolism
(AF, previous
thromboembolism, LV
3.0 + [I,B] + [I,A]
(75 – 100mg)
Life long](https://image.slidesharecdn.com/oralanticoagulation-211110115152/85/Oral-Anticoagulation-9-320.jpg)
![VALVE TARGET INR VKA ASPIRIN DURATION
Mechanical MVR 3.0 + [I,B] + [I,A]
(75 – 100mg)
Life long
Bioprosthetic MVR or
AVR in patients at low
risk of bleeding
2.5 + [IIa,B-NR] + [IIa,B]
(75 – 100mg)
At least 3 mths
as long as 6
mths.
Mechanical On-X
AVR and no
thromboembolic risk
factors
1.5 – 2.0 + [IIb, B-R
]
+
(low dose)
Life long
After TAVR in patients at
low risk of bleeding
2.5 + [IIa,B-NR] +(75-100mg)
along with
T.Clopilet
75mg for 1st
6mths [IIb,C ]
At least 3
months
Anticoagulant therapy
with oral direct
thrombin inhibitors or
anti-Xa agents should
According to
COR - III:Harm,
LOE - B.](https://image.slidesharecdn.com/oralanticoagulation-211110115152/85/Oral-Anticoagulation-10-320.jpg)



























































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)







