OPT 420 ORTHOPTICS AND VISION THERAPY NOTES current.pptx
1.
ORTHOPTICS AND VISIONTHERAPY
OPT-
DR CHARLES DARKO-TAKYI
DEPARTMENT OF OPTOMETRY AND VISION SCIENCE
UNIVERSITY OF CAPE COAST
2.
NON-STRABISMIC BINOCULAR VISION
ANOMALIES
•ACCOMMODATIVE ANOMALIES
• VERGENCE ANOMALIES
• FOCUS
• Classification and Diagnosis of anomalies
• Emphasis Scheiman and Wick’s Integrative Analysis Approach.
• Vision therapy for each conditions
UNIVERSITY OF CAPE COAST
3.
Definition: Accommodative anomaliesare characterized
by inadequate accommodative accuracy and
sustainability, inadequate amplitude, flexibility and
facility and are non-refractive and non-aging
neuromuscular abnormalities of the visual apparatus.
The accommodative classification system;
• Donders classification
• Expanded by Duke-Elder and Abrams
• Popularized by optometric authors e.g
Scheiman and Wick.
UNIVERSITY OF CAPE COAST
ACCOMMODATIVE ANOMALIES
4.
Functional etiology: categoriesof:
• accommodative insufficiency,
• ill-sustained accommodation or accommodative
fatigue.
• accommodative excess / spasm
• accommodative infacility / Inertia
UNIVERSITY OF CAPE COAST
ACCOMMODATIVE ANOMALIES
5.
Non-functional etiology
• Accommodativeparalysis
• Unequal accommodation
• Read my 2016 article: A review of the classification of
nonstrabismic binocular vision anomalies
UNIVERSITY OF CAPE COAST
ACCOMMODATIVE ANOMALIES
6.
Accommodative paralysis
• Suddenonset insufficiencies in accommodation
• Caused by either organic disorders in the nervous system or toxins. E.g.
careless use of cycloplegic drugs, toxicity, accidents, congenital defects and
diseases of the system
• It has been categorized as a sub classification of accommodative insufficiency.
• As a rare disorder, there is a failure of the accommodative apparatus to
respond to stimulus.
• Can be unilateral or bilateral, sudden or insidious
• Most often unilateral with extra ocular and pupillary involvement either fixed
or dilated. E.g. Third nerve palsy
UNIVERSITY OF CAPE COAST
ACCOMMODATIVE ANOMALIES
7.
Unequal Accommodation
• Unilateralcase of accommodative paralysis
• Accommodative insufficiency signs
• Sudden onset/sometimes insidious
• unilateral extraocular muscle involvement,
• Treatment of underlying systemic etiology
UNIVERSITY OF CAPE COAST
ACCOMMODATIVE ANOMALIES
8.
Vergence anomalies describedisjunctive movement of the eye in
which there is convergence or divergence, causing the eye to
inaccurately fixate and stabilize an image on the retina.
Two classification systems namely:
• Duane’s classification
• Wick’s classification
Purely descriptive classification and does not necessarily imply
etiology.
UNIVERSITY OF CAPE COAST
VERGENCE ANOMALIES
9.
Duane’s classification: Taitextended it to non-strabismic
Four main types namely:
• convergence insufficiency,
• convergence excess,
• divergence insufficiency
• divergence excess.
UNIVERSITY OF CAPE COAST
VERGENCE ANOMALIES
• Define: Visiontraining and treatment of vision related anomalies
• Rationale: Can train a lazy muscle or paretic muscle to work actively.
• Only possible if the condition is of a functional etiology with no systemic diseases or neurological disorder
( Nerve palsy ) involvement.
• History very important; no sudden onset of symptoms e.g diplopia and severe headaches etc
• Role out all systemic disease involvement before opting for orthoptics and vision therapy.
• Can do office-based therapy or home-based therapy
• Office based recommended for initial monitoring and training
• And when there is lack of extra training tools to send home
UNIVERSITY OF CAPE COAST
ORTHOPTICS AND VISION THERAPY
13.
Two broad categoriesnamely:
• Instrument training - includes all techniques in which the patient is required to look
directly into an instrument.
• movement of the patient is restricted,
• difficult to see the patient’s eyes.
• less natural or more artificial than other forms of therapy.
• Example : stereoscopic type device.
• Free space training, involves techniques in which the
• patient is in a less restricted environment,
• more movement is possible, and it is easier to observe the patient’s eyes.
• more closely approximates normal seeing conditions and is considered less artificial than instrument
training.
UNIVERSITY OF CAPE COAST
CATEGORIZATION OF VISION THERAPY INSTRUMENTATION AND
THERAPY- chapter five
14.
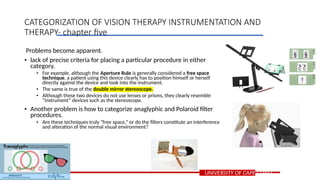
Problems become apparent.
•lack of precise criteria for placing a particular procedure in either
category.
• For example, although the Aperture Rule is generally considered a free space
technique, a patient using this device clearly has to position himself or herself
directly against the device and look into the instrument.
• The same is true of the double mirror stereoscope.
• Although these two devices do not use lenses or prisms, they clearly resemble
“instrument” devices such as the stereoscope.
• Another problem is how to categorize anaglyphic and Polaroid filter
procedures.
• Are these techniques truly “free space,” or do the filters constitute an interference
and alteration of the normal visual environment?
UNIVERSITY OF CAPE COAST
CATEGORIZATION OF VISION THERAPY INSTRUMENTATION AND
THERAPY- chapter five
15.
Classification based on: type of equipment being used
1. Anaglyphs and Polaroid filters
2. Lenses, prisms, and mirrors
3. Septa and apertures
4. Paper, pencil, and miscellaneous tasks
5. Stereoscopes
6. Afterimages, entoptic phenomena, and electrophysiologic techniques.
UNIVERSITY OF CAPE COAST
CATEGORIZATION OF VISION THERAPY INSTRUMENTATION AND
THERAPY- chapter five
16.
1. Stereoscopes
• Brewsterstereoscopes
• Wheatstone stereoscopes
• Haploscopes
• Cheiroscopes
UNIVERSITY OF CAPE COAST
CATEGORIZATION OF VISION THERAPY INSTRUMENTATION AND
THERAPY- chapter five
17.
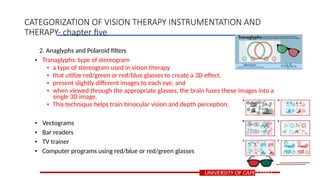
2. Anaglyphs andPolaroid filters
• Tranaglyphs: type of stereogram
• a type of stereogram used in vision therapy
• that utilize red/green or red/blue glasses to create a 3D effect.
• present slightly different images to each eye, and
• when viewed through the appropriate glasses, the brain fuses these images into a
single 3D image.
• This technique helps train binocular vision and depth perception.
• Vectograms
• Bar readers
• TV trainer
• Computer programs using red/blue or red/green glasses
UNIVERSITY OF CAPE COAST
CATEGORIZATION OF VISION THERAPY INSTRUMENTATION AND
THERAPY- chapter five
18.
3. Lenses, prisms,and mirrors
• Flip lenses: build accommodative facility
• Loose lenses
• Flip prisms: build vergence facility
• Loose prisms
• Prism bars: build fusional reserves
• Hand-held mirror
UNIVERSITY OF CAPE COAST
CATEGORIZATION OF VISION THERAPY INSTRUMENTATION AND
THERAPY- chapter five
19.
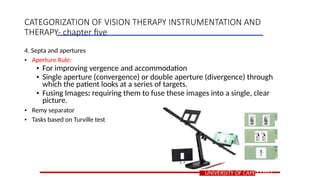
4. Septa andapertures
• Aperture Rule:
• For improving vergence and accommodation
• Single aperture (convergence) or double aperture (divergence) through
which the patient looks at a series of targets.
• Fusing Images: requiring them to fuse these images into a single, clear
picture.
• Remy separator
• Tasks based on Turville test
UNIVERSITY OF CAPE COAST
CATEGORIZATION OF VISION THERAPY INSTRUMENTATION AND
THERAPY- chapter five
20.
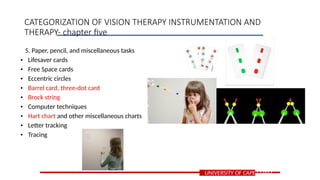
5. Paper, pencil,and miscellaneous tasks
• Lifesaver cards
• Free Space cards
• Eccentric circles
• Barrel card, three-dot card
• Brock string
• Computer techniques
• Hart chart and other miscellaneous charts
• Letter tracking
• Tracing
UNIVERSITY OF CAPE COAST
CATEGORIZATION OF VISION THERAPY INSTRUMENTATION AND
THERAPY- chapter five
21.
6. Afterimages, entopticphenomena, and electrophysiologic techniques
• Devices for creating afterimages
• Maxwell spot
• Haidinger brush
• Auditory biofeedback
UNIVERSITY OF CAPE COAST
CATEGORIZATION OF VISION THERAPY INSTRUMENTATION AND
THERAPY- chapter five
22.
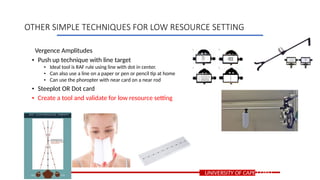
Vergence Amplitudes
• Pushup technique with line target
• Ideal tool is RAF rule using line with dot in center.
• Can also use a line on a paper or pen or pencil tip at home
• Can use the phoropter with near card on a near rod
• Steeplot OR Dot card
• Create a tool and validate for low resource setting
UNIVERSITY OF CAPE COAST
OTHER SIMPLE TECHNIQUES FOR LOW RESOURCE SETTING
23.
Accommodative Amplitude
• Pushup technique with accommodative target
• Ideal tool is RAF rule
• Can also use a near VA card at home or phoropter
• DOUCC PLOT
• i.e similar to dot steeplot but has letters within the circle.
• Ideal for Pseudoconvergence insufficiency
• SED’s Chart
• Design to train various accommodative parameters depending on the plate
• Under validation now
UNIVERSITY OF CAPE COAST
OTHER SIMPLE TECHNIQUES FOR LOW RESOURCE SETTING