DEPARTMENT OF PHARMACOLOGY
ALGESIA:
An unpleasant bodily sensation perceived as suffering, usually evoked
by an external or internal noxious stimulus.
ANALGESIC :
A drug that selectively relieves pain by acting in the CNS or on
peripheral pain mechanisms, without significantly altering
consciousness.
Excessive pain can cause :
• Sinking sensation
• Apprehension
• Sweating
• Nausea
• Palpitation
• Rise or fall in blood pressure
• Tachypnoea. 2
3.
DEPARTMENT OF PHARMACOLOGY
Typesof pain :
SOMATIC PAIN :
Pain arising from the skin or integumental structures likes
muscles, bones and joints.
VISCERAL PAIN :
Pain arising from the viscera is vague dull aching type difficult to
pinpoint to a site.
REFERRED PAIN :
When pain referred to a cutaneous area which receives nerve
supply from the same spinal segment as that of the affected
viscera.
3
4.
DEPARTMENT OF PHARMACOLOGY
ANALGESICS:
Opioidanalgesics / morphine like – analgesics
Nonopioid / non narcotic / aspirin – like /
antipyretic or anti-inflammatory analgesics.
Adjuvant analgesics: Anticonvulsants : Gabapentin /
pregabalin, Carbamazepine Antidepressants –
Amitriptyline.
4
5.
DEPARTMENT OF PHARMACOLOGY
Opium–
• Eber’s papyrus
SERTURNER a pharmacist isolated the active principle –
Morphine in 1806.
Named after Greek god of dreams – Morpheus.
Derived from the poppy capsule – Papaver somniferous
5
DEPARTMENT OF PHARMACOLOGY
8
ENDOGENOUSOPIOID PEPTIDES
• Beta – Endorphins – Proopiomelanocortin (POMC)
• Enkephalins -Pro enkephalin
• Dynorphins – A and B
• Nociceptin / Orphanin.
• Endomorphins 1 and 2
• Secreted naturally by the body for pain response.
DEPARTMENT OF PHARMACOLOGY
10
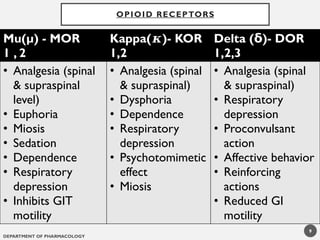
NOR– Nociceptin opioid receptor
Drug reward and reinforcement, stress responsiveness,
learning and memory.
Note:
Opioid receptors - also present – Peripheral nerves –
respond to peripherally applied opioids and locally released
endogenous peptides during inflammation.
DEPARTMENT OF PHARMACOLOGY
15
Pathwayof reward :
µ receptors are situated on GABAnergic neurons in CNS.
Connected to various dopaminergic neurons in CNS.
Opioids – blocks release of GABA
GABA mediated inhibition is reduced
Leads to increase dopaminergic outflow in ventral pallidum
Positive reinforcing state – Enhance reward
14.
DEPARTMENT OF PHARMACOLOGY
SYSTEMICEFFECTS OF OPIOID ANALGESICS
Central nervous system effects
1)Analgesia :
Mainly through Mu(µ) - µ1 and µ2 receptors
Raises the pain threshold.
Perception of pain and reaction to it are altered.
Dull aching pain is better reduced rather than sharp
pricking pain.
16
15.
DEPARTMENT OF PHARMACOLOGY
2)Euphoria :
Floating sensation with decreased anxiety and distress.
Produces a warm flushing of the skin and immensely
pleasurable sensation lasting for about 45 seconds which
is known as Kick or Rush .
Mediated through Mu 1 receptors.
3)Sedation and Hypnosis :
Drowsiness.
Morphine disrupts normal REM and non REM sleep
patterns.
17
16.
DEPARTMENT OF PHARMACOLOGY
4)Respiratorydepression –
Depress the medullary centers that regulate
the rate of respiration.
It may alter the rhythm to produce irregular and periodic
breathing.
Commonest cause of death in acute opioid
poisoning.
18
DEPARTMENT OF PHARMACOLOGY
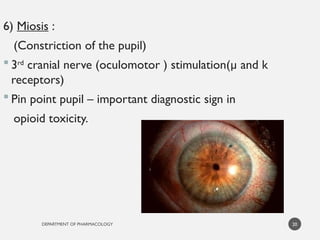
6)Miosis :
(Constriction of the pupil)
3rd
cranial nerve (oculomotor ) stimulation(µ and k
receptors)
Pin point pupil – important diagnostic sign in
opioid toxicity.
20
19.
DEPARTMENT OF PHARMACOLOGY
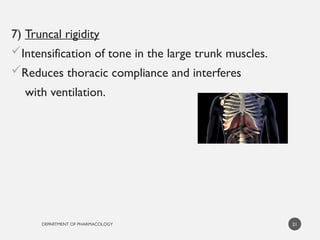
7)Truncal rigidity
Intensification of tone in the large trunk muscles.
Reduces thoracic compliance and interferes
with ventilation.
21
20.
DEPARTMENT OF PHARMACOLOGY
22
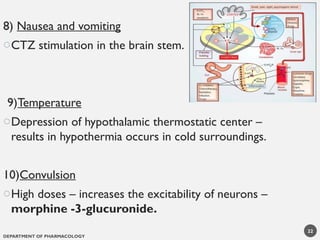
8)Nausea and vomiting
oCTZ stimulation in the brain stem.
9)Temperature
oDepression of hypothalamic thermostatic center –
results in hypothermia occurs in cold surroundings.
10)Convulsion
oHigh doses – increases the excitability of neurons –
morphine -3-glucuronide.
21.
DEPARTMENT OF PHARMACOLOGY
PERIPHERALEFFECTS
1)Cardiovascular system
Most opioids cause bradycardia and hypotension by
depression of vasomotor centre, histamine release and
directly acting on blood vessels – dilatation.
Meperidine causes tachycardia (due to structural
similarity to atropine).
23
22.
DEPARTMENT OF PHARMACOLOGY
2)Gastrointestinal tract
Motility is decreased and increased tone in the stomach.
Decreased secretion of hydrochloric acid.
Delay in the passage of fecal matter and
increased absorption of water in the large
intestine.
24
23.
DEPARTMENT OF PHARMACOLOGY
3)Biliary Tract
Contraction of biliary smooth muscle.
Constriction of sphincter
of Oddi - intrabiliary pressure.
25
24.
DEPARTMENT OF PHARMACOLOGY
4)Genitourinary system
Decreases renal plasma flow.
Increases renal tubular sodium reabsorption.
Increases ureteral and bladder tone.
Increases sphincter tone.
Inhibits voiding reflex.
Results in urinary retention especially in elderly.
26
25.
DEPARTMENT OF PHARMACOLOGY
5)Uterus
It may prolongs labor.
6)Neuroendocrine
Stimulates release of ADH , Prolactin and Somatotropin
but inhibits release of LH, FSH and ACTH.
Addicts – suffer from impotence, loss of libido and
infertility.
27
26.
DEPARTMENT OF PHARMACOLOGY
28
7)Pruritus:
Flushing of the skin
accompanied by sweating and itching – dilatation of
cutaneous blood vessels.
8) Immune system :
Mild immunosuppressant action
27.
DEPARTMENT OF PHARMACOLOGY
PHARMACOKINETICS:
Given orally absorption – slow.
Undergoes extensive first pass metabolism.
Bioavailability – 20 to 40%.
Rectal routes or highly lipid soluble preparations
are available.
29
28.
DEPARTMENT OF PHARMACOLOGY
Given subcutaneously onset of action is in 15
to 20 mins, Duration : 3-5 hours.
Metabolized by glucuronide conjugation.
Morphine-6 –glucuronide – More potent.
Morphine undergoes enterohepatic
circulation.
Morphine crosses blood brain and placental
barrier
Dose reduction is required in renal disease
patients.
30
DEPARTMENT OF PHARMACOLOGY
32
MCQ:
Whichamong the following metabolite of Morphine
is responsible for CNS excitability action?
a. Morphine 6 glucuronide
b.Morphine 3 glucuronide
c. Morphine 6 sulphate
d.Morphine 3 sulphate
31.
DEPARTMENT OF PHARMACOLOGY
33
Tolerance
Continued use of opioid analgesics.
Dose has to be increased to achieve the same analgesic
effect.
Marked tolerance develops to the analgesic, sedating,
respiratory depressant, antidiuretic, emetic and
hypotensive effects.
DEPARTMENT OF PHARMACOLOGY
35
DEPENDENCE
Physiologicalstate of neuroadaptation
resulting from repeated administration of
the drug
1)Psychological :
- Drug seeking behavior.
- Tolerance may or may not be present.
- Withdrawal effects are less frequent.
34.
DEPARTMENT OF PHARMACOLOGY
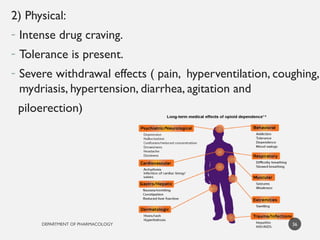
2)Physical:
- Intense drug craving.
- Tolerance is present.
- Severe withdrawal effects ( pain, hyperventilation, coughing,
mydriasis, hypertension, diarrhea, agitation and
piloerection)
36
35.
DEPARTMENT OF PHARMACOLOGY
37
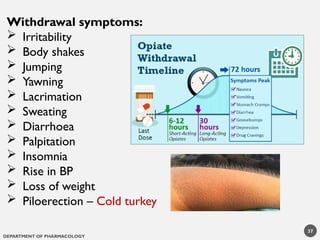
Withdrawalsymptoms:
Irritability
Body shakes
Jumping
Yawning
Lacrimation
Sweating
Diarrhoea
Palpitation
Insomnia
Rise in BP
Loss of weight
Piloerection – Cold turkey
36.
DEPARTMENT OF PHARMACOLOGY
ACUTEMORPHINE POISONING :
Accidental, suicidal or homicidal.
Lethal dose – 250mg.
SIGNS :
• Respiratory depression with shallow breathing
• Pin point pupils
• Hypotension
• Shock
• Cyanosis
• Flaccidity
• Stupor
• Hypothermia
• Coma
• Death due to respiratory failure and pulmonary edema.
38
37.
DEPARTMENT OF PHARMACOLOGY
TREATMENT:
A- Airway, B- Breathing, C- circulation
• Positive pressure ventilation.
• Maintenance of BP
• Gastric lavage with potassium permanganate to remove
unabsorbed drug.
• Specific antidote is Naloxone – 0.4 -0.8mg IV repeated till
respiration becomes normal.
39
38.
DEPARTMENT OF PHARMACOLOGY
40
TREATMENTOF DEPENDENCE:
Hospitalization of the patient.
Gradual withdrawal of morphine.
Substitution therapy – Methadone
(1mg Methadone = 4mg Morphine).
Naltrexone
Clonidine
Diazepam, Psychotherapy, Occupational therapy and
rehabilitation.
DEPARTMENT OF PHARMACOLOGY
42
Uses:
As analgesic:
In Myocardial infarction to relieve pain, pain in the patients
having cancers of higher stages.
Neurogenic shock due to severe pain- crush injuries.
Cancer pains.
Epidural analgesia – Morphine ( Fentanyl > Morphine)
Patient controlled analgesia (PCA)
Preanesthetic medication
Acute left ventricular failure / acute pulmonary edema.
41.
DEPARTMENT OF PHARMACOLOGY
43
CONTRAINDICATIONSOF MORPHINE:
1. Head injury
2. Bronchial asthma
3. Chronic obstructive pulmonary disease
4. Hypotension.
5. Hypothyroidism
6. Infants and elderly
7. Hypertrophy of prostate
8. Biliary spasm.
9. Pregnancy
10. Unstable personality
42.
DEPARTMENT OF PHARMACOLOGY
44
CO D E I N E
- It is methyl-morphine, occurring naturally in opium.
- 1/10th
of analgesic potency of morphine.
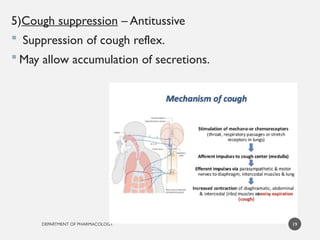
- Depresses the cough centre in sub analgesic doses.
43.
DEPARTMENT OF PHARMACOLOGY
45
CO D E I N E
- Produces less respiratory depression.
- Given orally.
- Partial mu agonist, when used as analgesic in high
doses, produce constipation.
- Used as antitussive.
44.
DEPARTMENT OF PHARMACOLOGY
46
-Synthetic opioid.
- Long acting mu receptor agonist and also blocks NMDA
receptors.
- Effective by oral route.
- Euphoric effects are less so abuse potency is less.
- Associated with prolonged QT syndrome.
METHADONE
45.
DEPARTMENT OF PHARMACOLOGY
47
Usesof Methadone:
Relief of chronic pain.
Treatment of opioid abstinence syndromes.
Treatment of heroin users – replacement modality to treat
heroin dependence.
46.
DEPARTMENT OF PHARMACOLOGY
48
•Plasma half life : 1-6hrs.
• 100 times more potent than morphine, given IV, intrathecal, epidural.
• Exhibit a short duration
• There is minimal depressant effect on the heart.
• Doesn’t increase intracranial pressure
Uses
Anesthetic adjuvants
Post operative pain – Transdermal patch
Cancer pain
Used as a component in neurolept analgesia.
FENTANYL
47.
DEPARTMENT OF PHARMACOLOGY
-1/10th
as potent as morphine.
- Potent mu agonist.
- Rapid onset of action but of short duration.
Uses –
Preanesthetic and obstetric analgesia
Adverse effects -
Atropine like effects(dry mouth, blurred vision,tachycardia).
49
PETHIDINE (MEPERIDINE)
48.
DEPARTMENT OF PHARMACOLOGY
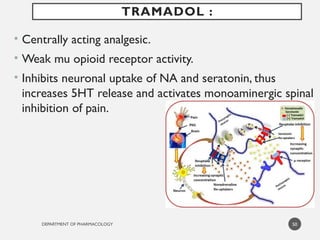
•Centrally acting analgesic.
• Weak mu opioid receptor activity.
• Inhibits neuronal uptake of NA and seratonin, thus
increases 5HT release and activates monoaminergic spinal
inhibition of pain.
50
TRAMADOL :
49.
DEPARTMENT OF PHARMACOLOGY
•Metabolized in liver and excreted through kidneys –
plasma t1/2 – 6 hours.
• Given orally for mild to moderate pain like in diagnostic
procedure, injury, for chronic cancer pain.
• Adverse effects :
• High incidence of nausea and dizziness.
• Dryness of mouth, sedation.
• May precipitate seizures.
• Seratonin syndrome.
51
TRAMADOL :
50.
DEPARTMENT OF PHARMACOLOGY
52
MIXEDAGONIST - ANTAGONISTS
Buprenorphine :
- mu partial agonist
- 25-50 times more potent than morphine
Sublingual - analgesia in post
operative patients
Treatment of opioid addiction - initiate with a
sublingual drug followed by maintenance
therapy with fixed dose combination
formulation of buprenorphine and naloxone.
51.
DEPARTMENT OF PHARMACOLOGY
Butorphanol:
Kappa agonist and mu antagonist
Best suited for relief of acute pain
Nasal formulation – relief of migraine pain
Side effects – Drowsiness,Weakness, Sweating ,
Feelings of floating and Nausea
53
52.
DEPARTMENT OF PHARMACOLOGY
54
Pentazocine:
Kappa agonist with weak mu antagonist or
partial agonist properties
Oldest mixed agent
Oral as well as injection.
Post-op pain, burns, trauma and cancer pain.
53.
DEPARTMENT OF PHARMACOLOGY
55
OPIOIDANTAGONISTS
Naloxone:
- Competitive antagonists at mu, delta and k receptors.
- Increases respiratory rate and BP.
- Reverses sedation and dysphoria.
- “Overshoot phenomenon”.
54.
DEPARTMENT OF PHARMACOLOGY
USES:
• Morphine over dosage (0.8 to 2mg I.M./ S.C.–very
2 to 3 mins to a total of 10mg max).
• Reverse neonatal asphyxia due to opioids used in
labor.
• Diagnosis of opioid dependence – Higher doses of
Naloxone will precipitate a withdrawal syndrome in
opioid dependent patients.
56
55.
DEPARTMENT OF PHARMACOLOGY
57
Naltrexone– Longer acting and potent -24hrs , pure
antagonist
- No euphoric effect and does not cause physical
dependence.
- Treating heroin addiction and also to prevent re-
addiction.
- Used in relapse of heavy drinking.
- Contraindicated in hepatitis and liver failure cases.
56.
DEPARTMENT OF PHARMACOLOGY
58
Nalmefene– Given by intravenous infusion.
- Onset of action is fast and longer duration of action
(10hrs).
- More potent than naltrexone.
- Used in maintenance therapy in treatment of opioid
addicts.
DEPARTMENT OF PHARMACOLOGY
60
Alvimopan:
-Mu receptor anatagonist.
- Does not cross BBB.
- Treatment of post operative ileus following bowel
resection surgery.
- Risk of myocardial infarction.
DEPARTMENT OF PHARMACOLOGY
64
Itis used for short surgical procedures – especially in
poor risk patients.
It is the combination of neurolept or antipsychotic –
Droperidol (2.5mg) and opioid analgesic Fentanyl (0.05mg).
Given IV – produces sedation and intense analgesia
without loss of consciousness.
It is maintained for 30 to 40 mins .
Have rapid and short action/
NEUROLEPT ANALGESIA
DEPARTMENT OF PHARMACOLOGY
66
IMPORTANTQUESTIONS:
1.Classify opioid analgesics. Explain the
pharmacological actions, uses and adverse effects
of morphine.
2.Write a note on morphine poisoning.
3.Naloxone.
4.Enumerate opioids and mention their use.





































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)













![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)